
Open Access, Volume 9
Clostridium perfringens bacteremia in an 89-year-old man with COVID-19 infection: Case report and brief literature review
Siasios Panagiotis1*; Zaires Aristidis1; Karapiperis Dimitrios2 ; Antoniou Dimitra1 ; Kachrimanidou Melina3
1Microbiology Department, 424 General Military Hospital, Thessaloniki, Greece.
2Clinic of Infectious Diseases, 424 General Military Hospital, Thessaloniki, Greece.
3First Department of Microbiology, Aristotle University of Thessaloniki, Medical School, Thessaloniki, Greece.
Siasios Panagiotis
Microbiology Department, 424 General Military Hospital, Thessaloniki, Greece.
Email: panossiassios@gmail.com
Received : Sep 08, 2023,
Accepted : Oct 10, 2023
Published : Oct 12, 2023,
Archived : www.jclinmedcasereports.com
Abstract
We present the rare case of bacteremia caused by Clostridium perfringens in an 89-year-old rehabilitation center resident with COVID-19 infection and we review the literature regarding C. perfringens bacteremia, as well as the association between SARS-CoV-2 and C. perfringens.
Keywords: Clostridium perfringens; Bacteremia; SARS-CoV-2; COVID-19 infection.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Panagiotis S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Panagiotis S, Aristidis Z, Dimitrios K, Dimitra A, Melina K. Clostridium perfringens bacteremia in an 89-year-old man with COVID-19 infection: Case report and brief literature review. Open J Clin Med Case Rep. 2023; 2134.
Introduction
Clostridium species are spore-forming anaerobic gram-positive rod bacteria, that are considered important constituents of the human microbiome, but also important agents in invasive infections, including bacteremia. Clostridial bacteremia is the second most frequent anaerobic bacteremia, ranging from 0.12-2% of all blood culture isolates [1-5]. Among Clostridium species, Clostridium perfringens is the most common species isolated from blood cultures [1-4]. Clostridium perfringens is normally part of the human gastrointestinal, genitourinary, and skin microbiota [6] but also a causative agent of skin and soft tissue infections, gas gangrene, myonecrosis, and liver abscess [7,8]. C. perfringens bacteremia is a rare clinical syndrome, accounting for less than 1% of all bloodstream isolates [1,9]. Although rare, C. perfringens bacteremia may be accompanied with high mortality rate, making it one of the most severe types of bacteremia [10].
Case Presentation
A 89-year-old male with a past medical history of atrial fibrillation and benign prostatic hypertrophy transferred to our hospital from a rehabilitation center, with an episode of atrial fibrillation with rapid ventricular response and COVID-19 infection. A day after the admission he presented with acute nausea and diarrhea, up to 3 green watery stools daily.
On admission, physical examination revealed him looking sick, emaciated and sometimes drowsy. He was oriented to place and to person but not to time. Vital signs demonstrated a blood pressure of 120/95 mm Hg, heart rate of 170 beats/minute, temperature of 37.4o C and oxygen saturation of 97% on room air. The cardiac examination revealed tachycardia, with normal heart sounds and no murmurs. His abdomen was soft and nondistended. The remainder of physical examination findings were normal. The performed ECG revealed an atrial fibrillation with rapid ventricular response, thus placing the patient under continuous electrocardiographic monitoring and later a decrease in heart rate was achieved pharmacologically with Digoxin and Lopressor in the emergency department. Because of the patient’s impaired level of consciousness, a brain CT scan was performed without pathological findings.
Complete blood count, comprehensive metabolic panel, urine, and blood cultures were done on admission. White blood cell was 9.64x103 /mm3 (NR: normal range 4-11x103 /mm3 ) with a left shift, while procalcitonin was slightly increased at 0.10 ng/ml (NR<0.08 ng/ml). Lactate dehydrogenase was 331 U/L (NR 125-220 U/L), troponin was 46.2 pg/ml (NR<34.2 pg/ml) and C-reactive protein was 9.5 mg/dl (NR <0.5 mg/dl). Total and direct bilirubin were also elevated at 2.21 and 1.04 mg/dl respectively (NR 0.2-1.2 mg/dl and 0.0-0.5 mg/dl respectively), indicating mild jaundice. D-dimer was elevated at 6.92 μg/mL (NR 0-0.5 μg/mL) and given the increased risk for thromboembolism a CT of the chest was obtained, which was negative for pulmonary embolism. The rest of his laboratory test results were within normal limits.
Empirical antibiotic treatment was initiated with intravenous piperacillin/tazobactam and remdesivir while the patient admitted to the infectious diseases clinic for further monitoring and treatment. The following days, a gradual and significant improvement of the patient’s clinical picture was observed.
Stool and blood cultures were requested. Stool specimen was tested for both glutamate dehydrogenase and toxins A/B of C. difficile by an enzyme immunoassay (EIA; C. DIFF QUICK CHECK COMPLETE, Alere/TechLab, Blacksburg, USA), which was negative.
Both sets of aerobic and anaerobic blood cultures (BACTEC Plus Aerobic, BACTEC Lytic Anaerobic, BD BACTEC™ FX40) yielded positive in 24 hours, and the initial Gram stain directly from the bottle revealed Gram-variable rods. The blood culture broth was sub-cultured onto the surface of Columbia (Columbia agar + 5% sheep blood; bioMerieux), chocolate agar (Chocolate agar + PolyViteX™, bioMerieux), and MacConkey agar, which incubated under aerobic and anaerobic conditions. The occurrence of anaerobic growth of Gram-positive boxcar-shaped rods on Gram stain (Figure 1), with negative catalase reaction and the phenotypic characteristic of the presence of double-zone hemolysis indicated the presence of Clostridia species. The microorganism was identified by mass spectroscopy as Clostridium perfrigens with a 99.0% confidence value using the Vitek® MS system (bioMerieux) and also by MALDI TOF (Brucker, MS system) with a score value of 2.31.
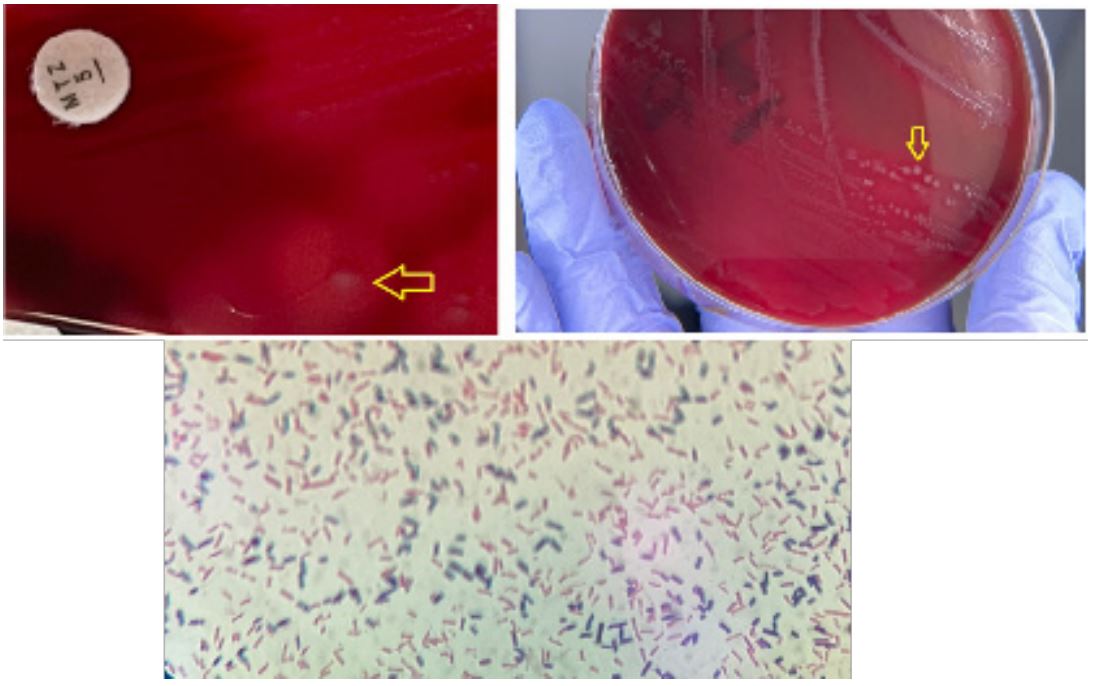
Figure 1: The colonies of Clostridium perfringens in Blood agar plate are surrounded by a double-zone
haemolysis, which consists of an inner clear zone and an outer hazy zone (yellow arrows). Gram stain of
Clostridium perfringens.
Literature Review
A PubMed and Google Scholar search of the English- language literature was performed using the keywords “Clostridium perfringens”, “bacteremia”, “SARS-CoV-2” and “COVID-19”. The systematic review of the literature revealed 19 studies that have been published since 1969, describing cases of C. perfringens bacteremia (Table 1). The literature shows that C. perfringens is the most common species identified in the blood cultures of patients with clostridial bacteremia, representing between 21.7-71% of Clostridium species bacteremia [1-5,12,15,18-20]. According to the medical literature, the main risk factor for acquiring Clostridial bacteremia is malignancy [1-6,8,10,12-20] and male gender (summarized in Table 1). (summarized in Table 1). The per- The per The percentage of males with clostridial bacteremia ranges from 27,3-88,2% [3-6,8,10-20]. Other risk factors for acquiring clostridial bacteremia include diabetes mellitus, older age, immunosuppression, haemodialysis, renal insufficiency, digestive surgery, chemotherapy, liver disease and Crohn’s disease [1-4,6,8,10,12,14, 16,18-19]. Yang et al. reviewed 93 cases of Clostridium bacteremia and found that 25.8% of patients had hypertension [10], while Benjamin et al. reviewed 80 cases and found that 12% of patients with clostridial bacteremia had alcohol use disorder [19]. The mean age of patients with clostridial bacteremia ranges from 46-76 years, with leukemia patients being younger [3-6,8,10-21].
Regarding the association between C. perfringens bacteremia and SARS-CoV-2, the literature revealed one case of COVID-19 infection associated with quadruple bacterial infection including C. perfringens bacteremia [22]. The present case is the second in the medical literature linking those two pathogens and emphasizes the fact that SARS-CoV-2 impacts the human immunity and promotes co-infections with unusual pathogens like C. perfringens.
Table 1: Review of Clostridial bacteremia.
| Author |
No cases of clostridium spp. bacteraemia/ Study period |
Clostridium perfringens (%) |
Most common comorbidities (%) | Mortality (%) |
Males (%) | Mean age |
|---|---|---|---|---|---|---|
| Suzaki et al. 2022 [11] | 60/2000-2014 | 100 | NR |
100 MIH 24.1 non- MIH |
58.1 |
66.5 MIH 77 non-MIH |
| Sarasoja et al. 2022 [12] | 386/2014-2019 | 40.4 |
Malignancy (47%) Immunosuppression (25%) |
26 | 56 | 76 |
| Liu et al. 2021 [13] | 17/1985-2020 | 100 | Leukemia | 58.8 | 88.2 | 46 |
| Yamamoto et al. 2020 [5] | 40/2004-2018 | 60 | Malignancy | 42.5 | 50.2 | 67.5 |
| Stabler et al. 2020 [4] | 81/2010-2018 | 64.3 |
Cancer (45.7%) Recent digestive surgery (24.7%) Chemotherapy (23.5%) Diabetes mellitus (22.2%) Renal insufficiency (22.2%) |
31.4 | 54.3 | 61.4 |
|
Lopez-Fabal et al. 2018 [14] |
28/2005-2015 | 100 |
Cancer (39.2%) Diabetes mellitus (25%) Immunosuppressants (21.4%) Recent surgery (17.8%) Liver disease (14.2%) Cholecystitis/cholelithiasis (14.2%) |
32.1 | 67.8 | 71.4 |
| Burgos et al. 2018 [15] | 18/2005-2016 | 38 | Cancer | 16 | 67 | 62.5 |
| Millard et al. 2016 [8] | 11 | 100 |
Older age ≥65 (64%) Diabetes mellitus (45%) Malignancy (18%) |
27 | 27.3 | 65.8 |
| Kim et al. 2015 [3] | 114/2002-2012 | 35.6 |
Neoplasm (76.3%) Gastrointestinal symptoms (73.7%) Diabetes mellitus (14.9%) Haemodialysis (5.3%) |
26.3 | 68.4 | 58 |
| Shindo et al. 2015 [16] | 33/2001-2013 | 100 |
Cancer Immunocompromised patients |
15.2 | 57.6 | 75.6 |
| Yang et al. 2013 [10] | 93/2002-2011 | 100 |
Renal insufficiency
(49,5%) Malignancy (41.9%) Hypertension (25.8%) |
26.9 | 58.1 | 70.7 |
|
van Bunderen et al. 2010 [6] |
40/1990-2010 | 100 |
Haematological disorder
(22.5%) Pancreatic/gastric cancer (12.5%) Diabetes mellitus (30%) |
80 | 55 | 65 |
| Fujita et al. 2010 [17] | 18/2001-2009 | 100 |
Hepatobiliary tract
diseases (gallbladder stones, hepatic carcinoma) |
27 | 72.2 | 75 |
| Shah et al. 2009 [18] | 25/1995-2003 | 60 |
Genitourinary/gastrointestinal
malig- nancies Diabetes mellitus |
48 | 44 | 64 |
| Leal et al. 2008 [2] | 138/2000-2006 | 42 |
Older age Hemodialysis Malignancy Crohn’s disease |
30 | NR | NR |
| Benjamin et al. 2006 [19] | 80/1997-2000 | 71 |
Neoplastic disease (31%) Diabetes mellitus (19%) Alcoholism (12%) |
28 | 59 | 70 |
| Rechner et al. 2001 [1] | 46/1990-1997 | 21.7 |
Older age ≥65 (67.4%) Diabetes mellitus (28.3%) Malignancy (47.8%) |
46 | NR | NR |
| Bodey et al. 1991 [20] | 135/1972-1983 | 32 | Malignancy | 58 | 52 | 52 |
|
Ellner and O'Donnell, 1969 [21] |
50/1964-1969 | 100 | NR | 901 | NR | 64 |
NR: Not reported, MIH: Massive intravascular haemolysis; Recovery rate.
Conclusion
Clostridium perfringens bacteremia, although relatively uncommon, is associated with high mortality due to advanced age and multiple comorbidities. The early recognition of this critical infection and early initiation of appropriate treatment are key factors of a positive outcome. SARS-CoV-2 impacts human im- SARS-CoV-2 impacts human immunity and co-infections with unusual bacteria like C. perfringens should be considered in patients with COVID-19 infection.
Declarations
Sources of funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of competing interest: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data availability: No data was used for the research described in this article.
References
- Rechner PM, Agger WA, Mruz K, Cogbill TH. Clinical features of clostridial bacteremia: a review from a rural area. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2001; 33(3): 349-353.
- Leal J, Gregson DB, Ross T, Church DL, Laupland KB. Epidemiology of Clostridium species bacteremia in Calgary, Canada, 2000-2006. The Journal of infection. 2008 ; 57(3): 198-203. https://doi.org/10.1016/j.jinf.2008.06.018
- Kim, Yeongbin & Yun, Jae & Chun, Sejong & Huh, Hee & Lee, Nam. Eleven-Year Experience of Clostridial Bacteremia at a Tertiary Care Hospital in South Korea. Annals of Clinical Microbiology. 2020 ; 18 : 126.
- Stabler S, Titécat M, Duployez C, Wallet F, Loïez C, et al. Clinical relevance of Clostridium bacteremia: An 8-year retrospective study. Anaerobe. 2020 ; 63: 102202.
- Yamamoto Y, Itoh N, Sugiyama T, Kurai H. Clinical features of Clostridium bacteremia in cancer patients: A case series review. Journal of infection and chemotherapy : official journal of the Japan Society of Chemotherapy. 2020 ; 26(1): 92-94.
- Van Bunderen CC, Bomers MK, Wesdorp E, Peerbooms P, Veenstra J. Clostridium perfringens septicaemia with massive intravascular haemolysis: a case report and review of the literature. The Netherlands journal of medicine. 2010 ; 68(9): 343-346.
- Shin DH, Park JH, Yoon KW, Shin JH, Kim SJ. (2003). Clostridium perfringens septicemia with thrombophlebitis of the portal vein. J Infect. 2003; 46: 253-5.
- Millard MA, McManus KA, Wispelwey B. Severe Sepsis due to Clostridium perfringens Bacteremia of Urinary Origin: A Case Report and Systematic Review. Case reports in infectious diseases. 2016; 2981729.
- Ingram CW, Cooper JN. Clostridial bloodstream infections. Southern Medical Journal. 1989; 82(1): 29-31.
- Yang CC, Hsu PC, Chang HJ, Cheng CW, Lee MH. Clinical significance and outcomes of Clostridium perfringens bacteremia--a 10-year experience at a tertiary care hospital. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2013; 17(11): e955-e960.
- Suzaki A, Komine-Aizawa S, Nishiyama H, Hayakawa S. Massive intravascular hemolysis is an important factor in Clostridium perfringens-induced bacteremia. Internal and emergency medicine, 2022; 17(7): 1959-1967.
- Sarasoja M, Nilson B, Wide D, Lindberg Å, Torisson G, Holm K. Epidemiology, aetiology and clinical characteristics of clostridial bacteraemia: a 6-year population-based observational study of 386 patients. European Journal of Clinical Microbiology and Infectious Diseases. 2022; 41(11): 1305-1314.
- Liu F, Xue S, Zhang Y, Yang J, Hu J, et al. Clostridium perfringens sepsis in three patients with acute leukemia and review of the literature. International journal of hematology. 2021; 113(4): 508-517.
- Lopez-Fabal, M.F, Sanz, N, Ruiz-Bastian, M, Barros, C, Gomez-Garces JL. Clostridium perfringens bacteraemia, an analysis of 28 cases over 10 years in a university hospital of Madrid. Enfermedades infecciosas y microbiologia clinica (English ed.). 2018; 36(4): 225-228.
- Burgos, Paula & Nanjappa, Sowmya & Snyder, Matthew & Bitetzakis, Christopher & Greene, John. (2018). Evaluation of Clostridium Bacteremia in the Cancer Population: A Case Series. Infectious Diseases in Clinical Practice. 26. 1. 10.1097/IPC.0000000000000655.
- Shindo Y, Dobashi Y, Sakai T, Monma C, Miyatani H, Yoshida Y. Epidemiological and pathobiological profiles of Clostridium perfringens infections: review of consecutive series of 33 cases over a 13-year period. International journal of clinical and experimental pathology. 2015; 8(1): 569-577.
- Fujita H, Nishimura S, Kurosawa S, Akiya I, Nakamura-Uchiyama F, Ohnishi K. Clinical and epidemiological features of Clostridium perfringens bacteremia: a review of 18 cases over 8 year-period in a tertiary care center in metropolitan Tokyo area in Japan. Internal medicine (Tokyo, Japan). 2010; 49(22): 2433-2437.
- Shah M, Bishburg E, Baran DA, Chan T. Epidemiology and outcomes of clostridial bacteremia at a tertiary-care institution. TheScientificWorldJournal. 2009; 9: 144-148.
- Benjamin B, Kan M, Schwartz D, Siegman-Igra Y. The possible significance of Clostridium spp. in blood cultures. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2006; 12(10): 1006-1012.
- Bodey GP, Rodriguez S, Fainstein V, Elting LS. Clostridial bacteremia in cancer patients. A 12-year experience. Cancer. 1991 ; 67: 1928-1942.
- Ellner PD, O’Donnell ED. Non-Fatal Clostridium perfringens Bacteremia. Journal of the American Geriatrics Society. 1969; 17: 644-647.
- Jimenez KP, Kaur KS, Chang AY, Chang E. A Case of Sars-Cov-2 Associated With Quadruple Bacterial Coinfection. Chest. 2022; 162(4): A604.
- Adams, B. N, Lekovic, J. P, & Robinson, S. Clostridium perfringens sepsis following a molar pregnancy. American journal of obstetrics and gynecology. 2014; 210(1): e13-e14.
- Chinen K. Sudden death caused by Clostridium perfringens sepsis presenting as massive intravascular hemolysis. Autopsy & case reports. 2020; 10(3): e2020185.
