
Open Access, Volume 9
Gastrointestinal bleeding caused by a hidden gastrointestinal stromal tumor of the stomach
Angelica Toppeta1,2*; Paola Molteni1 ; Alessandra Dell’Era1,2; Sandro Ardizzone1,2
1Department of Gastroenterology, Luigi Sacco Hospital, University of Milan, Milan, Italy
2Department of Clinical and Medical Sciences, University of the Study of Milan, Milan, Italy.
Angelica Toppeta
Department of Gastroenterology, Luigi Sacco Hospital, University of Milan, Milan, Italy.
Email: angelica.toppeta24@gmail.com
Received : Sep 05, 2023,
Accepted : Oct 09, 2023
Published : Oct 12, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Gastrointestinal stromal tumors (GISTs) are the most common type of mesenchymal tumor of the gastrointestinal tract. This report presents a case of a large exophytic stomach GIST that was not visible at esophagogastroduodenoscopy (EGD). A 70-year-old female presented to the emergency room with presyncopal symptoms and a history of several episodes of melena. Blood tests revealed severe anemia. She underwent an EGD, which yielded negative results. Subsequently, she was hospitalized and scheduled for ileo-colonscopy and videocapsule enteroscopy (VCE). Abdominal ultrasound showed the presence of a mass in the epigastric region near the liver. Computed tomography (CT) scans confirmed the presence of a mass in the gastric wall that, at endoscopic ultrasound (EUS) exam and biopsy, was diagnosed as a tumor that originated from the muscular layer of the stomach. Surgery was performed to excise the tumor, and the diagnosis of GIST was confirmed by histomorphological and immunohistochemical findings. According to the postoperative assessment, the tumor was classified as high risk, for which the recommended treatment is imatinib.
Keywords: GIST; Gastrointestinal stromal tumor; Gastric GIST; Gastrointestinal bleeding; Case report; Endoscopy; interstitial cells of Cajal.
Abbreviations: GISTs: Gastrointestinal stromal tumors; EGD: Esophagogastroduodenoscopy; VCE: Videocapsule enteroscopy; CT: Computed tomography; UGE: Ultrasound-guided endoscopy; Gi: Gastrointestinal tract; MRI: Magnetic Resonance Imaging.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Toppeta A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Toppeta A, Molteni P, Dell’Era A, Ardizzone S. Gastrointestinal bleeding caused by a hidden gastrointestinal stromal tumor of the stomach. Open J Clin Med Case Rep. 2023; 2133.
Introduction
Gastrointestinal stromal tumors (GISTs) are a type of mesenchymal tumor that originates from the interstitial cells of Cajal (ICCs), located within the muscular layer of the gastrointestinal tract (GI) [1]. GISTs are rare, constituting less than 1% of all gastrointestinal neoplasms. The stomach is the most common site of GISTs, accounting for 60% to 70% of all GIST tumors within the gastrointestinal tract. The small intestine is the second most common site, followed by the colon, rectum, and esophagus. GISTs are most frequently diagnosed in adults aged between 40 and 60 years. Men have a slightly higher incidence of GISTs compared to women [2-4]. Based on their location within the body, GISTs are classified as endoluminal, exoluminal, intramural, and mixed types.
GISTs are usually asymptomatic and are often incidentally discovered during endoscopies and radiological examinations. However, approximately 25% of patients may present with symptoms such as melena, hematemesis and anemia due to recurrent bleeding. Other common presenting symptoms and signs include early satiety, abdominal pain, and a palpable mass.
Around 80% of GISTs harbor activating mutations in the KIT or PDGFRA genes, which are receptor tyrosine kinases that regulate cell growth and proliferation. GISTs do not exhibit specific endoscopic characteristics, and their diagnosis relies on immunohistochemical analysis of markers such as KIT, CD34, or DOG1, which is essential for establishing a definitive diagnosis. Localized GISTs are potentially curable, and the standard treatment involves surgical resection. The primary goal of surgery is to remove the entire tumor with clear margins. In cases where complete removal is not achieved, there is a risk of recurrence, and chemotherapy becomes necessary [5].
Case Presentation
We present a 70-year-old female who was admitted to the Emergency Room following a pre-syncopal episode. Laboratory investigations showed severe anemia (hemoglobin 7.7 g/dL, MCV 78, hematocrit 22%). Other blood tests, including kidney and liver function, and coagulation profile, were normal. The physical examination revealed no abnormalities except for pallor. Her medical history included several episodes of melena over the past two years. For this reason, she had already undergone multiple upper and lower GI endoscopies, which failed to reveal any evidence of bleeding or potential bleeding sources. These examinations did, however, identify only the presence of hemorrhoids and diverticula. She also experienced intermittent symptoms of chronic dyspepsia and epigastric pain, which were managed with proton pump inhibitors. She had no history of changes in bowel habits or weight loss. She denied recent or past use of anti-inflammatory drugs. Her laboratory tests only once showed a mild anemia, which was successfully treated with iron supplementation. She also had a hematological evaluation, which was normal. Subsequently, she was admitted to the medical ward for further investigation of her anemia.
She repeated an upper GI endoscopy (Figure 1), which was completely normal without any sign of recent blood loss and was scheduled for ileo-colonoscopy and a video capsule endoscopy. In her diagnostic workup, we decided to perform an abdominal ultrasonography that revealed a giant mass measuring approximately 8-9 cm in the epigastric region, inferior and posterior to the liver. The lesion was composed of liquid and gas, featured a thickened wall measuring between 10 to 18 mm (Figure 2). All other abdominal organs appeared normal.
An abdominal CT scan confirmed the presence of a well-defined, giant, oval, heterogeneous enhancing mass, with extensive intralesional liquefaction and some bubbles, measuring about 10 x 6.7 x 5 cm (Figure 3). The mass appeared to be exophytic, originating from the wall of the lesser curvature, with no associated lymphadenopathy.
EUS (endoscopic ultrasound), performed three days after the initial emergency endoscopy, showed a slight bulging of the gastric wall of the lesser curvature and a small ulcer (Figure 4). The lesion, measuring 8.5 x 6 cm, was situated in the fourth layer and exhibited hypoechoic characteristics with mobile hyperechoic areas, indicative of liquefaction/necrosis (Figure 5). The lesion displayed a vascular Doppler signal and early enhancement with contrast medium. Fine needle aspiration biopsy was performed, and immunohistochemical staining revealed positive results for DOG1, CD117, Ki67 (<5%), while S-100, smooth muscle actin-negative, and p53 were negative. Cytological and immunohistochemical findings were consistent with a diagnosis of GIST.

Figure 1: Upper GI endoscopy.

Figure 2: Abdominal ultra-sound with the evidence of
the mass.
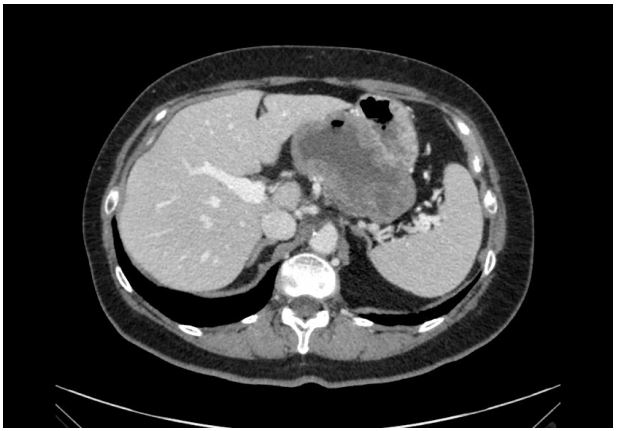
Figure 3: Abdominal CT scan with the evidence of the
gastric mass.

Figure 4: Abdominal ultra-sound with the evidence of
the mass.
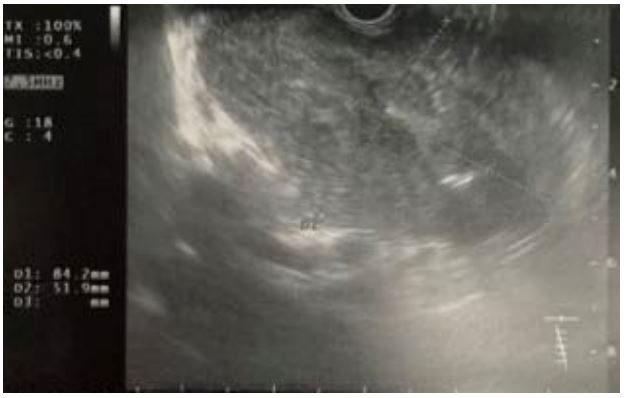
Figure 5: UGE with the evidence of the gastric mass.
A surgical laparotomy was performed, leading to a subtotal gastrectomy with reconstruction using a Y-shaped Roux-en-Y anastomosis. The resected tumor was well-circumscribed mass, measuring 11 cm. The decision to perform laparotomy was based on the collective findings of endoscopic, histopathological, and CT scans, all of which strongly indicated the presence of a gastric GIST. Pathologically, the mitosis count was 3/50 HPFs, and a mutation of exon 11 of KIT, a gene frequently mutated in GISTs, was identified. The resection margins were free of tumor. Therefore, the final diagnosis was malignant GIST with a KIT mutation. The patient is currently alive and well, receiving therapy with imatinib and undergoing regular oncologic follow-up.
Discussion
Patients with GISTs often remain asymptomatic, and this can lead to a missed initial diagnosis. When symptoms do manifest, the primary presentations include gastrointestinal bleeding, anemia, mucosal ulcers, or mass effect. Bleeding is the most common initial sign of GISTs, with hematemesis, melena, or anemia occurring as a consequence of the tumor eroding the gastrointestinal tract lumen, which serves as the origin of the condition. The diagnosis is usually established during endoscopy, where the presence of a bulging in the gastrointestinal wall, accompanied by either normal or ulcerated mucosa, can be seen. In rare cases where endoscopy fails to identify the source of bleeding, imaging techniques such as CT or magnetic resonance imaging (MRI) should be employed. UGE is a minimally invasive procedure that facilitates the visualization and biopsy of gastrointestinal lesions. It is often employed in the diagnose of GISTs, as it enables the identification of the specific wall layer from which the lesion originates and allows for the collection of biopsies [6]. The choice of treatment for GISTs depends on a several factors, including tumor size and location, the presence of metastasis, and the patient’s age and overall health.
Surgery stands as the first-line treatment for localized GISTs. If complete tumor removal is possible, the patient typically enjoys a favorable prognosis. In cases where complete resection is unattainable or if metastasis is present, alternative treatments such radiation therapy and chemotherapy may be considered.
In our case, the patient was fortunate enough to be suitable candidate for surgery. However, her diagnosis may have been delayed as she had been experiencing melena for approximately two years. It is crucial never to underestimate melena, and it is advisable to conduct a comprehensive evaluation that includes not only EGD and ileo-colonoscopy [7,8]. In instance where all these examinations yield negative results, imaging tests (e.g. abdominal ultrasound, CT scan or MRI) should be employed to evaluate the gastrointestinal tract for extraluminal lesions [9]. In our patient’s case, the implementation of these examinations at an earlier stage could have resulted in an earlier diagnosis.
Distinguishing GISTs from other mesenchymal-origin tumors is imperative due to their established resistance to chemotherapy and radiotherapy. Moreover, GISTs hold promise for targeted therapy using tyrosine kinase inhibitors (TKIs), such as imatinib, especially when KIT mutations are present [10].
Conclusion
GISTs have the potential to become malignant and can be life-threatening if left untreated. The recent increase in GISTs diagnoses can be attributed to advancements in imaging techniques, such as CT scans and MRI. These techniques can help to visualize tumors that are not visible on endoscopy. In cases of melena with repeatedly negative endoscopy results, it is crucial to always perform at least an imaging evaluation. Melena can arise from a spectrum of conditions, including GISTs, which may manifest as extraluminal sources of bleeding. Significant progress has been made in the development of novel treatment modalities for GISTs. Therefore, it is of paramount importance that all healthcare professionals are aware of the potential presence of conditions that might intermittently cause bleeding and, as a result, evade detection. It is crucial for all medical doctors to acknowledge the existence of GISTs, as diagnosing and treating them can be challenging. By recognizing the indications and symptoms of GISTs, doctors can contribute to ensuring that patients receive timely diagnosis and necessary treatment.
References
- Akahoshi K, Oya M, Koga T, Shiratsuchi Y. Current clinical management of gastrointestinal stromal tumor. World J Gastroenterol. 2018; 24(26): 2806-2817.
- Kim KM, Kang DW, Moon WS, Park JB, Park CK, Sohn JH, et al; Gastrointestinal Stromal Tumor Committee; Korean Gastrointestinal Pathology Study Group. Gastrointestinal stromal tumors in Koreans: it’s incidence and the clinical, pathologic and immunohistochemical findings. J Korean Med Sci. 2005; 20(6): 977-84.
- Tryggvason G, Gíslason HG, Magnússon MK, Jónasson JG. Gastrointestinal stromal tumors in Iceland, 1990-2003: the icelandic GIST study, a population-based incidence and pathologic risk stratification study. Int J Cancer. 2005; 117(2): 289-93.
- Goettsch WG, Bos SD, Breekveldt-Postma N, Casparie M, Herings RM, Hogendoorn PC. Incidence of gastrointestinal stromal tumours is underestimated: results of a nation-wide study. Eur J Cancer. 2005; 41(18): 2868-72.
- Blay JY, Kang YK, Nishida T, Von Mehren M. Gastrointestinal stromal tumours. Nat Rev Dis Primers. 2021 Mar 18; 7(1):22.
- Lee FD. Gastrointestinal Pathology and its Clinical Implications. Vols I and II. J Clin Pathol. 1992; 45(10): 943.
- Awadie H, Zoabi A, Gralnek IM. Obscure-overt gastrointestinal bleeding: a review. Pol Arch Intern Med. 2022; 132(5): 16253.
- Dziadkowiec KN, Stawinski P, Sánchez-Luna SA, Katz A. Gastrointestinal Stromal Tumor (GIST) Causing Obscure Gastrointestinal Bleeding: An Uncommon Way of Diagnosing an Uncommon Disease. Cureus. 2020; 12(8): e9558.
- Gerson, Lauren B; Fidler, Jeff L; Cave, David R; Leighton, Jonathan A. ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding. American Journal of Gastroenterology. 2015; 110(9): 1265-1287.
- Poveda A, García Del Muro X, López-Guerrero JA, Cubedo R, Martínez V, Romero I, et al. GEIS (Grupo Español de Investigación en Sarcomas/Spanish Group for Sarcoma Research). GEIS guidelines for gastrointestinal sarcomas (GIST). Cancer Treat Rev. 2017; 55: 107-119.
