
Open Access, Volume 9
Obstructive quandary: A comprehensive case report of gallstone ileus
Viveiros Fábio*; Mendes João; Monteiro Cristina; Gomes Diana; Escaleira Rui; Midões Alberto
Department of General Surgery, Local Health Unit of Alto Minho (ULSAM), Portugal.
Viveiros Fábio
Department of General Surgery, Local Health Unit of Alto Minho (ULSAM), Portugal.
Email: fabiocorreiaviveiros@gmail.com
Received : Sep 01, 2023,
Accepted : Oct 06, 2023
Published : Oct 12, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Gallstone ileus (GI), an infrequent but complex complication of cholelithiasis, poses a multifaceted challenge in the field of general surgery. We present a case report of a 99-year-old male with GI, characterized by mechanical obstruction within the small bowel due to gallstone impaction, and offer a review of the literature on this subject. GI emerges as a late-stage complication of gallstone disease, primarily manifesting in elderly individuals, with a higher incidence among women. The condition is driven by the migration of gallstones through fistulas, most commonly forming connections with the small bowel. Diagnosis is intricate due to nonspecific clinical symptoms, often requiring imaging modalities like abdominal CT scans. Treatment necessitates surgical intervention, addressing both intestinal obstruction and cholecystoenteric fistula management. The approach, whether one-stage or sequential, is guided by individual patient characteristics.
Keywords: Gallstone ileus; Cholelithiasis; Surgical management; Obstruction; Cholecystoenteric fistula.
Abbreviations: GI: Gallstone Ileus; ACE: Angiotensin-Converting-Enzyme; CRP: C-reactive Protein; CT: Computed Tomography
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fábio V (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Fábio V, João M, Cristina M, Diana G, Rui E, Alberto M. Obstructive quandary: A comprehensive case report of gallstone ileus. Open J Clin Med Case Rep. 2023; 2132.
Introduction
Cholelithiasis stands as one of the most prevalent surgical conditions, capable of a wide range of symptoms and complications, including acute cholecystitis, pancreatitis, choledocholithiasis, and cholangitis [1]. In more uncommon instances, it can evolve into a complex scenario known as gallstone ileus (GI).
GI entails a mechanical obstruction within the small bowel, triggered by the lodgment of a gallstone within the gastrointestinal tract. This condition emerges as a late-stage complication of gallstone disease, frequently attributed to a cholecystoenteric fistula. These fistulas are commonly found with the duodenum, due to its proximity to the gallbladder, less frequently with the colon, and exceedingly rarely with the stomach. Occurring in merely 1 to 4% of all cases of intestinal obstruction, GI remains an infrequent outcome of cholelithiasis, with a higher incidence noted in elderly patients. The optimal approach for treatment involves the mechanical removal of the impacted stones. This is most effectively achieved through surgical means, encompassing both open and laparoscopic procedures. In instances where the stones have become lodged in the colon, and endoscopic approach might also be considered as a viable option [2,3,4]. Here we present a case report of a GI, followed by a review of the literature on this subject.
Case Presentation
A 99-year-old independent male presented to the surgical emergency room with a chief complaint of abdominal pain that had started two days ago. The patient characterized the pain as acute and centralized in the midsection of the abdomen, noting a progressive increase in intensity over the past 48 hours. There was no radiation of pain to other areas. Additionally, the patient reported experiencing postprandial nausea and vomiting since the previous day. Notably, he had not experienced a bowel movement during the entirety of this two-day period. The patient explicitly denied the presence of fever, usual abdominal discomfort associated with these symptoms, or any other concurrent ailments.
In terms of his medical background, the patient had a documented history of heart failure characterized by a reduced ejection fraction, necessitating tailored pharmacological management including beta-blockade, ACE inhibitor administration, and diuretic therapy. Furthermore, the patient presented with a concurrent diagnosis of atrial fibrillation, warranting anticoagulation therapy (apixaban). The patient’s surgical history was devoid of any previous abdominal procedures or other surgical interventions, and he possessed no recollection or awareness of prior occurrences of gallstone disease.
Upon thorough clinical assessment, the patient presented without fever, exhibiting normal blood pressure and heart rate values. He displayed a state of overall well-being, characterized by adequate hydration, a healthy complexion, absence of jaundice, and unlabored breath. Upon conducting an abdominal examination, tenderness was discerned within the periumbilical region, albeit without evidence of involuntary muscle guarding. Bowel sounds were notably heightened get devoid of metallic resonance. Noteworthy, there were no indications of peritoneal irritation. A rectal examination revealed the absence of fecal matter or blood.
The preliminary hematological analysis conducted upon admission revealed a hemoglobin concentration of 12.2 g/dl. The white blood cell count was determined to be 14,000 cells/mm3 , featuring a predominance of 61% neutrophils. Platelet enumeration yielded a count of 320,000/mm3 . Furthermore, the CRP concentration registered at 5.00 mg/dl, while serum lactate levels were quantified at 2.1 g/dl. It is pertinent to note that all other hematological parameters remained within acceptable physiological ranges, inclusive of coagulation markers.
In light of these observations, an abdominal CT scan was requisitioned. The ensuing abdominal CT scan unveiled the presence of a nodular structure measuring approximately 30 mm within the lumen of the ileal loop. This condition was accompanied by dilation of the upstream loop, marked by ectasia encompassing the stomach. Additionally, multiple discrete areas of calculi were discerned within the gallbladder, though no indications of acute cholecystitis were noted (Figure 1).
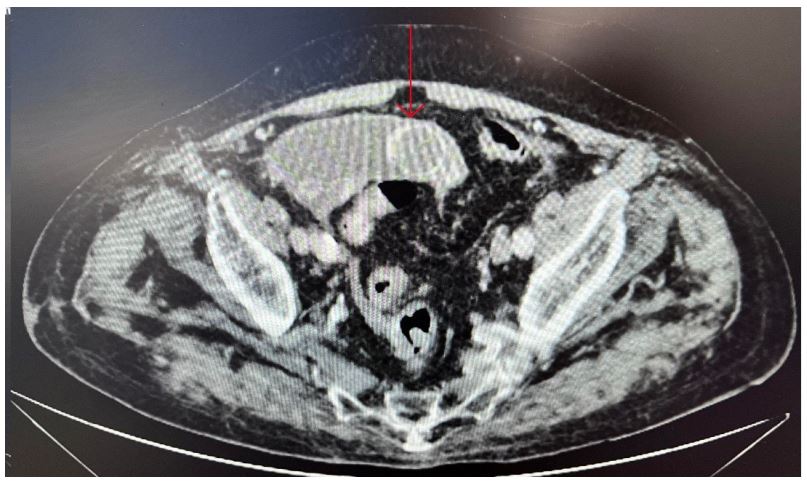
Figure 1: Axial section of the Abdominal CT scan - It can be seen as identified by the arrow a
nodular structure within the lumen of the ileal loop.
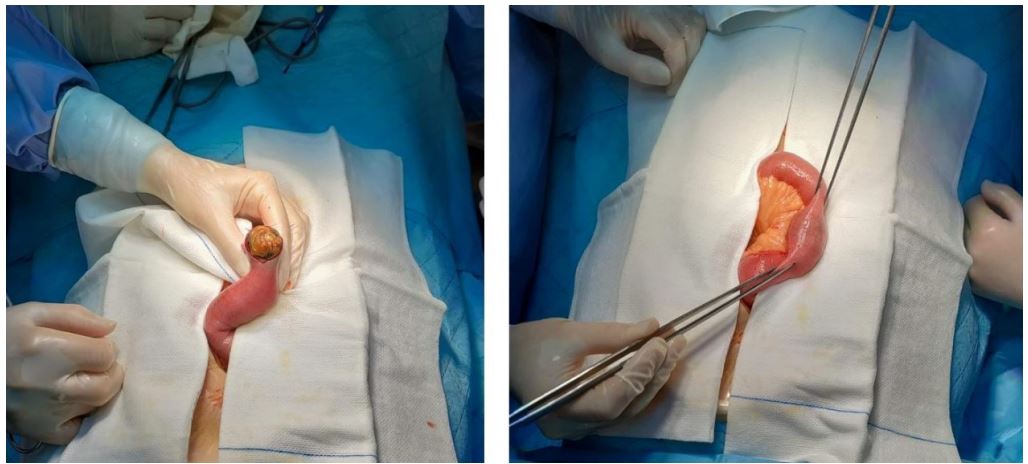
Figure 2: Gallstone extraction through enterectomy.
Based on these findings, coupled with the patient’s initially stable condition, an initially conservative approach was adopted within the initial 24 hours. Nonetheless, the patient’s clinical condition exhibited a progressive deterioration, manifested by aggravated abdominal distention and no bowel movements. After a comprehensive assessment of risks and benefits, in consultation with both the patient and their family, a surgical intervention was deemed advisable and subsequently proposed. The patient provided informed consent for the proposed surgical procedure.
Consequently, the patient underwent an enterectomy with concurrent extraction of the gallstone (as depicted in Figure 2), and the procedure went without any notable complications. Postoperatively, the patient encountered an abdominal evisceration complication, necessitating a subsequent surgical intervention for resolution. Not withstanding this setback, the subsequent postoperative period unfolded uneventfully, ultimately leading to the patient’s discharge.
Histological examination of the stone yielded results consistent with gallstone composition. Subsequent to this, the patient underwent a comprehensive revaluation in consultation, demonstrating stability and a favorable general condition. There were no indications of enduring complications identified during this assessment.
The consideration of a secondary intervention involving fistula closure and cholecystectomy was thoroughly deliberated. However, a comprehensive assessment of the potential risks and benefits was conducted, taking into account the patient’s age and existing comorbidities. Subsequently, a collaborative decision was reached in consultation with the patient and their family to decline the secondary intervention.
Discussion
GI emerges as a noteworthy complication of gallstone disease, affecting approximately 0.3% to 4% of patients afflicted with cholelithiasis [5]. This disorder, more prevalent among women with a female-tomale ratio of around 3.5 to 1, typically arises when gallstones obstruct the gastrointestinal tract. For an obstruction to occur, the stone must attain a diameter of at least 2 to 2.5 cm [6]. Remarkably, GI primarily manifests in elderly patients with underlying health issues, often in a frail state, amplifying the morbidity and mortality associated with this condition [7].
The development of GI is intricately linked to the migration of a gallstone through a fistula that forms due to chronic inflammation within the gallbladder. Subsequently, this fistula establishes a connection with the small bowel, although instances of connection with the colon or stomach are less frequent and extremely rare. An alternative but exceedingly rare pathway involves the direct passage of a stone from the ampulla of Vater, accompanied by local growth, which significantly escalates the risk of concurrent cholangitis [2,7].
Diagnosing GI is a complex attempt, often undertaken prior to surgery (in 43% to 73% of cases), given the intricate diagnostic challenges associated with this condition and the tendency for patients to present with non-specific clinical symptoms [7,8]. Clinical manifestations vary contingent on the site of obstruction. Given that the small bowel is the most common site of blockage [2], patients typically exhibit symptoms such as abdominal pain, abdominal distention, nauseas, vomiting, constipation, and fluid imbalance. In a chronic scenario, recurrent episodes of abdominal pain result from the gallstone’s passage through the intestines, interspersed with asymptomatic intervals, ultimately culminating in complete obstruction over successive stages. As the disease advances, there’s potential for perforation, leading to peritonitis and acute abdominal symptoms.
Laboratory investigations also lack specificity in diagnosing GI. Common findings may encompass an elevated white blood cell count, as observed in our patient’s case. Additionally, abnormalities in liver function may be noted, although they were absent in our patient. Furthermore, electrolyte imbalances can arise, although our patient did not present with such deviations, as previously indicated.
Imaging plays a fundamental role in the diagnostic approach of GI. Given that gallstones typically lack radiopacity, they might be visible on plain abdominal radiograms, often accompanied by air-fluid levels in patients with obstruction. Yet, the origin of the obstruction remains indiscernible through abdominal radiography. Abdominal ultrasound serves as a valuable tool, allowing not only identification of the impacted stone, but also visualization of the fistula site and the presence of cholelithiasis. However, its efficacy may be diminished in cases of bowel obstruction due to challenges posed by air interposition.
In scenarios where GI is suspected, the abdominal CT scan emerges as the imaging modality of choice. This method excels in pinpointing the site of obstruction, precisely locating the fistula, and offering enhanced accuracy in gauging the size of the ectopic stone [2,9].
The treatment approach primarily revolves around surgical intervention, with a dual focus on addressing intestinal obstruction and subsequently managing the cholecystoenteric fistula. The decision to perform these procedures simultaneously or sequentially hinges on the patient’s overall condition, bearing in mind that individuals with GI are often elderly and burdened by comorbidities.
The management of intestinal obstruction necessitates an enterolithotomy, typically conducted either laparoscopically or through laparotomy. In the case of our patient, considering his age, ability to tolerate the laparoscopy’s pneumoperitoneum, and the surgical team’s experience, the laparotomy route was chosen.
Managing cholelithiasis and the cholecystoenteric fistula typically entails the closure of the fistula alongside a cholecystectomy. However, as previously discussed, the prospect of a secondary intervention was not entertained in our patient’s situation.
According to existing literature, opting for one-stage procedure offers advantages such as diminished recurrences of gallstone ileus, prevention of malabsorption and consequential weight loss from a persisting cholecystoenteric fistula, as well as averting cholecystitis. Nonetheless, this approach carries an elevated risk of surgical morbidity and mortality [10].
Conclusion
In essence, GI represents a complex interplay between gallstone disease and complicated anatomical pathways. Predominantly affecting elderly individuals with comorbidities, this condition underscores the need for nuanced diagnostic and treatment strategies. With treatment pivoting around surgical intervention, the approach necessitates a personalized consideration of patient’s characteristics. This comprehensive analysis propels the medical community towards more informed decisions, enhancing outcomes for this intricate complication of gallstone disease.
Disclosure: The authors declare no conflict of interest.
References
- Kreve F, Takada J, Gatto J, Loss FS, Artifon EL). Íleo biliar: caso clinico. Revista de Gastroenterología del Perú. 2017; 37(2): 173-176.
- Jakubauskas M, Luksaite R, Sileikis A, Strupas K, Poskus T. Gallstone ileus: management and clinical outcomes. Medicina. 2019; 55(9): 598.
- Clavien PA, Richon J, Burgan S, Rohner A. Gallstone ileus. British Journal of Surgery. 1990; 77(7): 737-742.
- Suro-Santos Y, Serrato-Ruíz JA, Fuentes-Hernández JE, Macías-Landeros BH, Chávez-Rodríguez J. Biliary ileus an uncommon cause of intestinal occlusion: case report. Revista médica del Hospital General de México. 2023; 86(1): 43-46.
- Beuran, M, Ivanov, I, & Venter, M. Gallstone ileus–clinical and therapeutic aspects. Journal of medicine and life. 2010; 3(4): 365.
- Dai XZ, Li GQ, Zhang F, Wang XH, Zhang, CY. Gallstone ileus: case report and literature review. World Journal of Gastroenterology: WJG. 2013; 19(33): 5586.
- Orellana, M, Vegas L, Cáceres A, Villarroel M, Soto P. Laparoscopic management of gallstone ileus: A case report and literature review. International Journal of Surgery Case Reports. 2021; 85: 106171.
- Chang L, Chang M, Chang, H. M, Chang, A. I, & Chang, F. Clinical and radiological diagnosis of gallstone ileus: a mini review. Emergency radiology. 2020; 25, 189-196.
- Yu CY, Lin CC, Shyu RY, Hsieh CB, Wu HS, Tyan YS, et al. Value of CT in the diagnosis and management of gallstone ileus. World journal of gastroenterology. WJG. 2005; 11(14): 2142.
- Clavien PA, Richon J, Burgan S, Rohner, A. Gallstone ileus. British Journal of Surgery. 1990; 77(7): 737-742.
