
Open Access, Volume 9
Advanced metallothionein profile in children with malaria infection
Somieye Imaobong Brown; Mathias Abiodun Emokpae*
Department of Medical Laboratory Science, School of Basic Medical Sciences, University of Benin, Benin City, Nigeria.
Mathias Abiodun Emokpae
Department of Medical Laboratory Science, School of Basic Medical Sciences, University of Benin, Benin
City, Nigeria.
Email: mathis.emokpae@uniben.edu
Received : Aug 17, 2023,
Accepted : Oct 05, 2023
Published : Oct 12, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Malaria is a leading cause of death in sub-Sahara Africa including Nigeria. The oxidative stress associated with malaria infection may affect the plasma protective proteins and trace elements which participate in the antioxidant defensive system.
Aim: The aim of this study was to assess the Advanced Metallothionein Profile (AMP) of malaria infected children in Benin metropolis and determine its association with parasite density.
Methods: This case-control study had a total of 350 children between 6 months and 11 years with two hundred malaria positive children as case and 150 malaria negative children as control. Socio-demographic data was obtained through a semi-structured questionnaire. Blood samples were taken from participants to determine malaria parasite density using thick film microscopy. Serum Metallothionein (MT), Glutathione (GSH) and Ceruloplasmin (CP) were analyzed using Enzyme linked Immunosorbent assay (ELISA) techniques, while copper (Cu) and Zinc (Zn) levels were determined using Atomic Absorption spectrometry (AAS). The data were analyzed using appropriate statistical tools.
Results: The mean values of metallothionein, ceruloplasmin, and glutathione were significantly higher (p<0.001) among malaria infected children compared with the control. Zinc was lower though not significantly (p>0.05) but copper was significantly lower (p<0.05) in malaria infected children than control. The mean parasite density of the malaria infected children was parasites/µL of blood. Ceruloplasmin correlated inversely (r=-0.15, p=0.04) with parasite density, while other parameters showed no association with parasite density. The odds of having elevated serum metallothionein 62.67 (95% C.I 30.89-127.15), ceruloplasmin 13.58 (95% C.I 7.84-23.21) and glutathione 2.37 (95% C.I 1.48-3.81) were higher in malaria infected children than the control. The area under curve (AUC) shows that metallothionein (AUC=0.98±0.01, p<0.05), ceruloplasmin (AUC=0.91±0.02, p<0.05) and glutathione (AUC=0.76±0.03, p<0.05) maybe useful antioxidant biomarkers in malaria infection.
Conclusions: Data from this study indicate that marked changes occurred in the AMP of children with malaria infection and its inclusion in routine investigation may enhance management and reduce mortality due to malaria infection.
Keywords: Child; Metallothionein; Malaria; Falciparum.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Emokpae MA (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Brown SI, Emokpae MA. Advanced metallothionein profile in children with malaria infection. Open J Clin Med Case Rep. 2023; 2131.
Introduction
Malaria is a serious disease which is endemic to sub-Saharan Africa. It is responsible for about half a million deaths annually in the region [1]. Children under the age of 5 years are the most vulnerable and account for about 67% of all the malaria deaths that occurred globally in 2019 [2]. The impact is such that in 2018, the child mortality rate in Nigeria stood at 25% [3]. The disease is transmitted by the bites of female Anopheles mosquitoes while attempting to take a blood meal from a human host to nurture their eggs. Febrile illness occurs when conditions are favourable such as observed in individuals who have low immunity against the pathogen such as children and pregnant women. The combined response of the host defensive system and the effect of the P. falciparum pathogen usually produce free radicals which are mostly Reactive Oxygen Species (ROS) and Reactive Nitrogen Species (RNS) which can result in oxidative stress due to an imbalance between the free radicals and the plasma antioxidant defence system [4]. The host system responds to the infection by releasing pro-inflammatory mediators like Tumour Necrotic Factor (TNF) and cytokines (IL-6, IL-16, IL-18) which are responsible for symptoms such as fever, vomiting, diarrhoea, weakness of the joints and in severe cases anaemia, respiratory distress, and cerebral malaria [5]. Certain molecules within the immune system carry out protective functions. The sources of antioxidant defences involved in malaria infection are mainly: Host enzyme antioxidants, host non-enzymatic antioxidants such as vitamins and Glutathione (GSH), non-enzymatic antioxidants from the host’s metal chelation system such as iron, Copper (Cu), Zinc (Zn), Ceruloplasmin (CP) and metallothionein-chelating proteins, and exogenous antioxidants from drugs and food [6].
Not much work on the status of metallothionein in children has been done. Advanced Metallothionein Profile (AMP) measures not only Metallothionein (MT) but also Zinc (Zn), Copper (Cu), free copper, Ceruloplasmin (CP) and Glutathione (GSH) [7], which can be used to monitor the effectiveness of detoxification treatments and as a guide for modulating immune deficiencies. Moreover, the report on global and regional burden of disease on child mortality, has implicated zinc deficiency in 10% of malaria death [8,9]. AMP may be a useful guide for evaluation and modulation of immune status. A study of the AMP in children with malaria infection may be of great interest since metallothionein concentrations may be influenced by both exogenous and endogenous factors such as environment, diet, gender, age [10] including inflammatory conditions like malaria infection. Therefore, monitoring the ensuing immunopathology in malaria infected children to know the interplay between oxidative stress, inflammatory response, metal regulation, and the levels of immune parameters might enable healthcare professionals to know ways to intervene in the course of the disease. It is well established that early diagnosis allows for quick intervention that may improve survival rates/outcome. Therefore, the aim of this study was to determine the AMP being a measurable indicator of both antioxidants and immune status among subjects and its correlation with malaria infection severity among children with malaria infection.
Material and Methods
Study area/design
A case control study with quantitative and qualitative data collection from the Military Hospital, Central Hospital and Stella Obasanjo Children and Women Hospital, Benin City, Edo State. Nigeria between December 2019, and April 2020.
Clinical and anthropometric measurements
The Physical examination was done by the attending physicians while anthropometric measurements were done by qualified nurses using standard scales for the height and weight measurements. Other areas of special interest that were considered are body temperature, history of any underlying ailment, current medication regimen, socioeconomic status of parents or guardians and the parents’ general knowledge of malaria preventive measures which were obtained by questionnaire answered by the child’s parent or custodian.
Study Population
A total of 350 subjects attending Outpatient Department of the various clinics within Benin metropolis were consecutively recruited for this study. The age range of the participants was between 6 months and 11 years. They were 184 males and 166 females. After evaluation, those tested positive for malaria by thick blood film microscopy were used as cases with mean age 6.51±0.22 years. Children with mean age 6.0±0.25 who visited the hospitals for pre-school medical check that tested negative for malaria were used as controls. Sample size (n) was determined using the Fischer formula [11].
n=Z²P (1-P)/I²
Where:
n = minimum sample size
Z = Standard normal deviate that corresponds to 95% confidence limit (1.96)
I = alpha level of significance (5%)
P = Prevalence
Inclusion and exclusion criteria
Children with clinical signs/symptoms for malaria between 6 months and 11 years who tested positive to malaria by microscopy and have not used anti-malaria drugs in the past 1-2 weeks. Aged matched asymptomatic healthy children that were on routine medical screening who, tested negative for malaria were used as controls. Children that were malnourished, known history of sickle cell anaemia, HIV positive or any other ailment or disease which may contribute to the oxidative stress level of the participating subjects were excluded from the study. Also, those on anti-malaria drugs were excluded.
Ethical consideration
Ethical approval was obtained from the Ethics and Research Committee, Ministry of Health, Edo State with Reference number HA-737/28 dated 27th November 2019. Informed consent was given by the parents or guardians of study participants and the socio-demographic and medical history were obtained from the medical records or from the parents/guardians using questionnaire.
Sample collection/analysis
Blood samples (5 mL) were collected from the subjects and dispensed into plain containers. Blood samples were allowed to clot and after clot retraction, they were centrifuged at 3000 rpm for 10 min and sera were separated and aliquoted into properly labelled tubes and stored at -20˚C prior to analysis of metallothionein, ceruloplasmin, glutathione, zinc, and copper. Thick blood films were made immediately after the collection of blood on clean slides, allowed to dry, and stained with 10% Giemsa of pH 7.0 for 15 min. Slides were read microscopically with x100 objective (oil immersion). Parasite density per micro litre of blood was estimated from the thick film by assuming the number of white blood cell (WBC) per microliter of blood as 8,000 and expressed as follows:

Where N = number of asexual parasitic forms present in as many microscopic fields as possible to count 200 leucocytes.
Parasitaemia was quantified per 200 WBC; where less than 100 parasites were counted, 500 WBC was used to calculate parasitaemia. A slide was declared negative after about 100 high power field (HPF) were examined without malaria parasite detected.
Sample analysis for MT, CP GSH, Cu, and Zn
Metallothionein, Ceruloplasmin and Glutathione were measured using ELISA techniques, while copper and zinc were analysed using Atomic Absorption Spectrophotometer (AAS).
Principle for ELISA technique
This assay is based on the sandwich ELISA principle where each well of the supplied microtiter plate has been pre-coated with a target specific capture antibody. Standards or samples are added to the wells and the target antigen binds to the capture antibody. Unbound Standard or sample is washed away An avidin-Horseradish Peroxidase (HRP) conjugate is then added which binds specifically to the assayed antigen. Unbound avidin-HRP conjugate is washed away. A Tetramethyl benzidine (TMB) substrate is then added which reacts with the HRP enzyme resulting in color development. A sulfuric acid stop solution is added to terminate color development reaction and then the Optical Density (OD) of the well is measured at a wavelength of 450 nm ± 2 nm. An OD standard curve is generated using known antigen concentrations; the OD of an unknown sample can then be compared to the standard curve in order to determine its antigen concentration.
Principle of atomic absorption spectrometry
Atomic absorption spectrometry is based on the principle that free atoms in an atomizer can absorb radiation at specific wavelength or frequency. Radiation from a hollow cathode lamp (in which the cathode is made from the element of interest) is modulated and passed through a flame into which is sprayed the solution for analysis. The radiation then passes to a monochromator where the particular resonance line required is isolated, and any absorption due to the atomic vapor in the flame is measured by means of photomultiplier. The photocurrent is amplified, demodulated and fed either directly to a meter or to a Logarithmic Converter. The calibration curve obtained by plotting the response or absorbance of an analyte against concentration helps to determine the concentration of analyte in an unknown sample and by comparing the unknown to a set of standard samples of known concentration. The correlation coefficients of the standards prepared were between 0.95 and 0.999.
The measurement was taken two times and the average was calculated. Standard solutions were prepared in each case before metal concentrations were determined and were used to eliminate sample standard matrix indifferences. They were also used to calibrate the AAS instrument for all the analytes and also to prepare their calibration curves. The Multi element standards manufactured by Sigma Aldrich were used to prepare the standard of various concentrations.
Data analysis
The SPSS (Statistical package for social sciences) software version 26.0 and Jimovi version 2.3.1 was used for statistical analysis. Values obtained are expressed as mean ± standard deviation and were compared using the student t-test and Analysis of Variance (ANOVA). Pearson correlation coefficient was used to correlate the various parameters with parasite density. Receiver Operating Characteristic (ROC) was used to determine the diagnostic capability of the assayed parameters. The level of significance used was set at P<0.05.
Result
Table 1: Shows the socio-demographic characteristics of the study population. The mean age of the test subjects is 6.51±0.22 years and that of the controls is 6.00±0.23 years. Ninety-six (64.0%) of the controls are males, while 44.0% of the test subjects are males with significant statistical difference (X2 =13.751, p<0.001) between gender in the test and controls. Some 33.3% of the controls are between 0-4 years, 53.4% are 5-9 years and 13.3% are 10-11 years old of age. Again 30.0% of the test subjects are between 0-4 years, 49.0% are 5-9 years and 21% are 10-11 years of age with no significant statistical difference (X² =3.093, p=0.213) in age between the groups. Also, among the controls, 26.7% of the parents/ guardians are civil servant, 65.3% are into business, 8.0% are unemployed while among subjects, 31.0% are civil servants, 68.0% are into business and 1.0% are unemployed with significant statistical difference (X2 =11.143, p=0.004) in occupation among study group. Also, 70.0% of the control subjects use malaria preventive measures, 30.0% do not take malaria preventive measures, while 59.5% of the test subjects take malaria preventive measures and 40.5% do not take malaria preventive measures with significant statistical difference (X2 =4.012, p=0.043) among them as shown on Table 1.
Table 2: Shows the comparison of the mean values of measured parameters between malaria infected and control group. The mean values of metallothionein, ceruloplasmin, and glutathione were significantly higher (p<0.001) among children infected with malaria parasite than non-malaria infected control subjects. While zinc (p>0.05) and copper (p<0.004) in malaria infected children were lower than non-malaria infected control subjects. Similarly, the mean MT/GSH, MT/Zn and CP/Cu were significantly higher (p<0.001) while Cu/Zn ratio was lower (p<0.003) among malaria infected children than controls. Obviously, the mean parasite density of the malaria infected children was 716.75±61.14 cells/µl of blood.
Table 3: Shows the correlation between measured parameters and malaria parasite density. It showed that only ceruloplasmin (CP) showed a weak inverse correlation (r=-0.15, p=0.04) with malaria parasite density as there is no significant correlation between the other parameters and malaria parasite density in this study.
Table 4: Shows the levels of abnormal profile and the odd risk in subjects and controls. The odd of having elevated serum metallothionein 62.67 (95% C.I 30.89-127.15), ceruloplasmin 13.58 (95% C.I 7.84-23.21) and glutathione 2.37 (95% C.I 1.48-3.81) levels in malaria infected children were statistically significant (p<0.001) compared to the controls. In other words, the children with malaria infection are sixty-three times more likely to have elevated MT than those without malaria; they are thirteen times more likely to have elevated CP than those without malaria and twice more likely to have abnormal GSH than those without malaria.
Table 5 and figure 4.1: Show the Area under Curve (AUC) and the potential of measured parameters as antioxidant biomarkers in malaria infection. The area under curve of each of the parameters is as follows: metallothionein (AUC=0.98±0.01, p<0.05), ceruloplasmin (AUC=0.91±0.02, p<0.05) and glutathione (AUC=0.76±0.03, p<0.05), copper (AUC=0.41±0.03, p<0.05) and Zinc (AUC=0.54±0.03, p>0.05). All the parameters except Cu and Zn gave acceptable fit (AUC>0.7). The performance is in the order: MT>CP>GSH>Zn>Cu. All the AUC were statistically significant except Zn.
Table 1: Socio-demographic characteristics of the study population.
| Measured serum parameter |
Malaria infected. n=200 (Mean ± S.E) |
Non-Malaria infected. n=150 (Mean± S.E) |
t- value | p-value |
|---|---|---|---|---|
| Metallothionein (pg/ml) (20-41.2) | 118±4.54 | 30.6±0.87 | 16.51 | <0.001 |
| Ceruloplasmin(pg/ml) (14.2-74.7) | 98.2±1.93 | 44.7±2.45 | 17.39 | <0.001 |
| Glutathione (pg/ml)) (32.4-98.5) | 97.7±3.66 | 65.8±2.75 | 6.56 | <0.001 |
| Zinc (mg/l) (0.64-1.24) | 1.15±0.06 | 1.23±0.11 | -0.68 | 0.49 |
| Copper (mg/l) (0.75-1.53) | 1.33±0.03 | 1.49±0.05 | -2.89 | 0.004 |
| Cu/Zn ratio | 1.3±0.05 | 1.47±0.07 | -2.96 | 0.003 |
| MT/GSH ratio | 1.37±0.09 | 0.54±0.04 | 10.95 | <0.001 |
| MT/Zn ratio | 116.1±7.1 | 31.84±1.8 | 14.34 | <0.001 |
| CP/Cu ratio | 81.5±3.6 | 31.82±2.6 | -14.8 | <0.001 |
| Parasite density (cells/μl of blood) | 716.75±61.14 | 0.000±0.00 | - | - |
Table 2: Comparison of mean levels of measured parameters and their ratio in malaria infected non-malaria infected children (control).
| Parameters | Controls (%) n=150 | Subjects (%) n=200 | X2(p-value) | |
|---|---|---|---|---|
| Gender | Male | 96(64.0) | 88(44.0) | 13.751(0.001) |
| Female | 54(36.0) | 112(56.0) | ||
| Mean age of the children | 6.00±0.23 | 6.51±0.22 | 0.112 | |
| Age group of the children | 0-4 years | 50(33.3) | 60(30.0) | 3.093(0.213) |
| 5-9 years | 80(53.4) | 98(49.0) | ||
| 10-11 years | 20(13.3) | 42(21.0) | ||
| Occupation of the parents | Civil Servant | 40(26.7) | 62(31.0) | 11.143(0.004) |
| Business | 98(65.3) | 136(68.0) | ||
| Unemployed | 12(8.0) | 2(1.0) | ||
| Parents education level | Primary | 22(14.7) | 18(9.0) | 6.331(0.097) |
| Secondary | 54(36.0) | 65(32.5) | ||
| Tertiary | 64(42.7) | 109(54.5) | ||
| None | 10(6.7) | 8(4.0) | ||
| Prevention measures | Yes | 105(70.0) | 119(59.5) | 4.102 (0.043) |
| No | 45(30.0) | 81(40.5) |
p<0.05: Statistically Significant; p>0.05: Not statistically significant X² : Chi Square; n: Sample Size. N: Sample Size; P<0.05: Statistically significant; p>0.05: Not statistically significant; MT: Metallothionein; CP: Ceruloplasmin; GSH: Reduced glutathione; Zn: Zinc; Cu: Copper
Table 3: Association between measured variables and parasite density among malaria infected children
|
Correlation parameters |
r-value | p-value | |
|---|---|---|---|
| MT |
Parasite density |
0.03 | 0.72 |
| CP | -0.15 | 0.04* | |
| GSH | 0.05 | 0.52 | |
| Cu | -0.01 | 0.89 | |
| Zn | 0.03 | 0.73 | |
| MT/GSH | -0.09 | 0.18 | |
| MT/Zn | 0.005 | 0.95 | |
| CP/Cu | 0.04 | 0.56 | |
| Cu/Zn | -0.09 | 0.19 | |
Correlation is significant at p<0.05; MT: Metallothionein, CP: Ceruwloplasmin; GSH: Reduced glutathione; Zn: Zinc, Cu:Copper.
Table 4: The unadjusted Odd ratio (95% C.I) of normal and abnormal levels of measured parameters among malaria infected children and controls.
| Subjects | Control | OR (95% C.I) | χ2 | p | |
|---|---|---|---|---|---|
| MT | |||||
| Normal | 12(6.0) | 120(80.0) | 62.67(30.89-127.15) | 199.812 | <0.001 |
| Abnormal | 188(94.0) | 30(20.0) | |||
| CP | |||||
| Normal | 22(11.0) | 94(62.7) | 13.58(7.84-23.21) | 103.3 | <0.001 |
| Abnormal | 178(89.0) | 56(37.3) | |||
| GSH | |||||
| Normal | 118(59.0) | 116(77.3) | 2.37(1.48-3.81) | 13.002 | <0.001 |
| Abnormal | 82(41.0) | 34(22.7) | |||
| Cu | |||||
| Normal | 130(65.0) | 94(62.7) | 1.11(0.71-1.72) | 0.203 | 0.653 |
| Abnormal | 70(35.0) | 56(37.3) | |||
| Zn | |||||
| Normal | 150(75.0) | 106(70.7) | 0.80(0.50-1.29) | 0.819 | 0.365 |
| Abnormal | 50(25.0) | 44(29.3) |
Note: Abnormal consists of any value outside reference range. OR: Odd Ratio; MT: Metallothionein; CP: Ceruloplasmin; GSH: Reduced Glutathione; Zn: Zinc; Cu: Copper; CI: Confidence Interval; χ2: Chi Square; p<0.05: Statistically Significant; p>0.05: Not statistically significant
Table 5: Potential of measured parameters as antioxidant biomarker in malaria infection using receiver operating characteristics and Area under the curve (AUC).
| Parameter | AUC | SE | 95%CI | Significance |
|---|---|---|---|---|
| Metallothionein (pg/ml) | 0.98 | 0.01 | 0.97-0.99 | <0.001 |
| Ceruloplasmin (pg/ml) | 0.91 | 0.02 | 0.87-0.94 | <0.001 |
| Glutathione (pg/ml) | 0.76 | 0.03 | 0.71-0.81 | <0.001 |
| Zinc(mg/l) | 0.54 | 0.03 | 0.40-0.53 | 0.174 |
| Copper (mg/l) | 0.41 | 0.03 | 0.39-0.53 | 0.006 |
Auc: Area Under The Curve; Se: Standard Error; Ci: Confidence Interval; P<0.05: Statistically Significant, P>0.05: Not Statistically Significant.
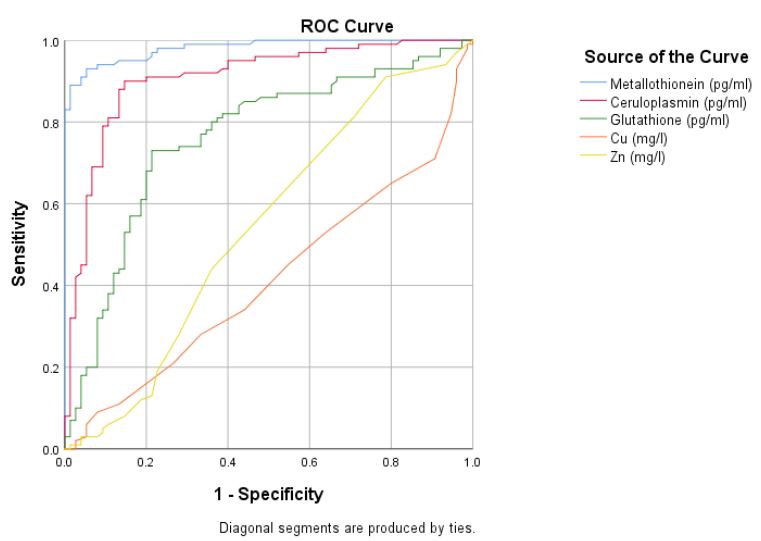
Figure 1: Receiver Operating Characteristics (ROC) of measured parameters among malaria infected children.
Discussion
Metallothionein level of children with malaria infection may be different from those without malaria infection due to oxidative stress associated with the physiopathology of malaria infection. Data from this study indicated that MT concentration was significantly higher (p<0.001) in malaria infected children than non-malaria infected subjects but had no correlation with the parasite density. Ruttkay-Nedecky et al. [12] opined that MT has the capacity to scavenge hydroxyl radical produced in malaria infection by quickly capturing the -SH group to terminate their oxidative damage property. Recently, MTs have increasingly been recognized as a vital component of the immune system, but rarely assayed routinely and the significantly higher levels of serum metallothionein observed in this study seem to support its antioxidant functions.
Ceruloplasmin (CP) levels of malaria infected children in this study was observed to be significantly higher (p<0.001) than the control group and correlated inversely (r=-0.15; p=0.04) with parasite density. This finding aligned with the previous study [13], a significantly higher CP level (p<0.001) in adult patients with P.falciparum infection was reported when compared with healthy individuals. The rupturing of blood cells by the malaria parasite causes the release of its iron contents which in its ferrous state is harmful to the body [14]. Ceruloplasmin through its ferroxidase activity detoxifies them from the system by binding to the free ferrous iron in circulation to get rid of them. Therefore, the high concentrations of CP seen in the malaria infected children in this study may not be unusual as they try to mop up excess free iron in circulation.
Glutathione (GSH) levels in malaria infected children was significantly higher (p<0.001) than those of the non-malaria infected children but had no correlation with parasite density. GSH is hydrophilic which enables it to permeate easily almost all cell types and would be readily available in any oxidative stress conditions as found in malaria infection. In Katsina northwestern. Nigeria, glutathione was reported to be significantly lower among children of the same age group who were infected with P. falciparum [15]. Malaria parasites are known to possess powerful and host-independent mechanisms which spontaneously synthesize or regenerate reduced glutathione (GSH) from oxidized glutathione (GSSG) to protect the parasites from oxidative damage particularly at the trophozoite stage in human erythrocytes [16]. The oxidized glutathione (GSSG) produced from the intact infected cell is said to be more than 60-fold higher than the rate observed in normal erythrocytes, and part of the GSSG that is expelled from the parasite is reduced to GSH in the host cell [17], which in addition to the pool of glutathione in the system may be responsible for the high levels seen in this study.
Some studies have shown that plasma concentrations of micronutrients are altered during acute infections or inflammatory stress, but the direction and level of change may be conflicting. In this study, it was observed that the serum zinc level in malaria infected children was not significantly different when compared to the non-malaria infected children and had no correlation with parasite density. Some authors have shown that malaria infection may reduce the availability of micronutrients by inducing loss of appetite with associated decreased intake of nutrients [18,19]. The infection may also result in a state of malabsorption or alter the body’s metabolism and increase demand for nutrients [20] which may be responsible for the low values observed in this study.
Similarly in this study, serum copper levels in malaria infected children were significantly lower (p=0.004) than the non-malaria infected children and had no correlation with parasite density. Otitoju [21], reported that children with acute malaria infection are reported to have very low plasma copper concentration which is inversely related to the C-reactive acute phase proteins which may not be unconnected to its functions as copper stimulates the immune system to fight infection, repair injured tissues, and promote healing [22]. Bjorkland [23], stated that increased expression of metallothionein in the liver due to host cytokine release in malaria infection, leads to poor mobilization of micronutrients from the liver to other organs hence their low concentrations in blood was observed in this study.
Conclusion
Advanced Metallothionein Profile (AMP) levels of children with malaria parasite are altered by the infection, and therefore different from those without the infection. Metallothionein, Ceruloplasmin (CP) and Glutathione (GSH) were observed to be significantly higher (p<0.001) in children with malaria infection compared to their control group. Zinc and Copper were observed to be low with copper being significantly lower (p=0.004) in the malaria infected subjects than the control group. There was no correlation between the parameters and parasite density except ceruloplasmin which showed a weak significant inverse association. MT, CP and GSH possess the ability to be used as antioxidant biomarkers for malaria infection as the area under the receiver operating characteristics curve (AUC) for each was greater than 0.7. Also, the odds of having elevated values of these parameters were higher in the malaria infected subjects than the control group. If we must stem the tide of malaria mortality in children, strategies that are directed towards early and accurate diagnosis of malaria infection in endemic areas should adopted. This study reveals that we can leverage on obvious and specific changes within the immune system which can serve as early warning signs in predicting dangerous outcomes during malaria infection especially in children. Advanced metallothionein profile can be added as a routine investigation to assess the immune and antioxidant status of children with malaria infection.
Declarations
Acknowledgement: The contributions of the clinicians, nurses and Medical Laboratory Scientist at the Military Hospital, Central Hospital and Stella Obasanjo Children and Women Hospital all in Benin City, Edo State are highly appreciated.
Funding Source: None
Conflict of interest: No conflict of interest was declared by the authors.
Abbreviations: AAS: Atomic Absorption Spectrophotometry; AMP: Advanced Metallothionein Profile; ELISA:-Enzyme Linked Immunosorbent Assay; Profileor: Odd Ratio; MT: Metallothionein; CP: Ceruloplasmin, GSH: Reduced Glutathione; ROS: Reactive Oxygen Species; RNS: Reactive Nitrogen Species; Zn: Zinc; Cu: Copper; CI: Confidence Interval; WHO: World Health Organization.
References
- World Health Organization. Global malaria, World Malaria Report 2018. 2018.
- World Health Organization. 20 years of Global Progress and Challenge, World malaria report, 2020 Geneva. Licence: CC BY-NCSA 3.0 IGO. 2020.
- Edelu BO, Ndu IK, Igbokwe OO, Iloh ON. Severe falciparum malaria in children in Enugu, Southeast Nigeria, Nigerian Journal of Clinical Practice 2018; 21: 1349-1355.
- Percário S, Moreira DR, Gomes BA, Ferreira ME, Gonçalves AC, et al. Oxidative stress in malaria. International Journal of Molecular Sciences. 2012; 13: 16346-16372.
- Gowda, D.C., and Wu, X. Parasite Recognition and Signalling Mechanisms in Innate Immune Responses to Malaria, Frontiers in Immunology. 2018; 9, 3006.
- Gomes ARQ, Cunha N, Varela ELP, Brígido HPC, Vale VV, et al. Oxidative Stress in Malaria: Potential Benefits of Antioxidant Therapy. Int J Mol Sci. 2022; 23: 5949.
- Shaw W. Metallothionein Update. 2009.
- King JC, Brown KH, Gibson RS, Krebs NF, Lowe NM, et al. Biomarkers of Nutrition for Development (BOND). Zinc Review. The Journal of Nutrition. 2016; 146: 858S-885S.
- Gammoh NZ, Rink L. Zinc in Infection and Inflammation, Nutrients. 2017; 9: 624.
- Isani G, Carpene E. Metallothioneins, Unconventional Proteins from Unconventional Animals: A Long Journey from Nematodes to Mammals, Biomolecules. 2014; 4: 435-457
- Ogbeibu AE. Biostatistics: A practical approach to research and data handling; 2nd Edition, 2014; 20-22.
- Ruttkay-Nedecky B, Nejdl L, Gumulec J, Zitka O, Masarik M, et al. The role of metallothionein in oxidative stress, International Journal of Molecular Science. 2013; 14: 6044-6066.
- Ezzi AAA, Salahy MBA, Shnawa BH, Abed GH, Mandour AM. Changes in Levels of Antioxidant Markers and Status of Some Enzyme Activities among Falciparum Malaria Patients in Yemen, Journal of Microbiology and Experimentation. 2017; 4: 00131.
- Ademolue TW, Awandare GA. Evaluating anti-disease immunity to malaria and implication for vaccine design, Immunology. 2018; 153: 423-443.
- Abubakar MG, Usman SM, Dandare SU. Oxidant status of children infected with Plasmodium falciparum in Katsina metropolis, Northwestern Nigeria, African Journal of Infectious Diseases. 2016; 10: 17-20.
- Lutgen P. The ambiguous role of glutathione in malaria, Malaria World Journal. 2015.
- Atamna H, Ginsburg H. The malaria parasite supplies glutathione to its host cell-investigation of glutathione transport and metabolism in human erythrocytes infected with Plasmodium falciparum, European Journal of Biochemistry. 1997; 250: 670-679.
- Shenkin A. Micronutrients in health and disease, Postgraduate Medical Journal. 2006; 82: 559-569.
- Oldenburg CE, Guerin PJ, Berthé F, Grais RF, Isanaka S. Malaria and Nutritional Status among Children with Severe Acute Malnutrition in Niger: A Prospective Cohort Study. Clinical infectious diseases: An official publication of the Infectious Diseases Society of America. 2018; 67: 1027-1034.
- Benzecry SG, Alexandre MA, Vítor-Silva S, Salinas JL, de Melo GC, et al. Micronutrient Deficiencies and Plasmodium vivax, Malaria among Children in the Brazilian Amazon, PloS One. 2016; 11: 23-25.
- Otitoju OO. Effect of Malaria Infection on Serum Copper, Iron and Beta-Carotene Levels in Nigerian Children, European Journal of Scientific Research. 2012; 86: 573-579.
- Mbugi EV, Meijerink M, Veenemans J, Jeurink PV, McCall M, et al. Alterations in early cytokine-mediated immune responses to Plasmodium falciparum infection in Tanzanian children with mineral element deficiencies: A cross-sectional survey. Malaria Journal. 2010; 9: 130-135.
- Bjorklund G. The role of zinc and copper in autism spectrum disorders, Acta Neurobiologiae Experimentalis. 2013; 73: 225-236.
