
Open Access, Volume 9
An unexpected diagnosis: Metastasis of the gallbladder from breast cancer - A case report
Viveiros Fábio*; Couto José; Escaleira Rui; Martins Aires; Matos Carolina; Midões Alberto
Department of General Surgery, Local Health Unit of Alto Minho (ULSAM), Portugal.
Viveiros Fábio
Department of General Surgery, Local Health Unit of Alto Minho (ULSAM), Portugal.
Email: fabiocorreiaviveiros@gmail.com
Received : Aug 21, 2023,
Accepted : Oct 05, 2023
Published : Oct 12, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Breast cancer is nowadays the most frequently diagnosed cancer worldwide. It is often associated with the local and lymphatic spread and with metastatic disease of the lungs, liver, and bones. The metastatic lesions of the gallbladder are an uncommon clinical condition and the gallbladder is an extremely rare organ to be involved in breast cancer and only a few cases have been reported in the literature. Here we report a case of a gallbladder metastasis from a patient with breast cancer following a review of the literature for similar cases and an overview of this condition.
Keywords: Breast cancer; Gallbladder; Metastasis; Rare; Cholecystectomy.
Abbreviations: BC: Breast Cancer; ER: Estrogen Receptors; PR: Prolactin Receptors; CRP: C-Reactive Protein; ALP: Alkaline Phosphatase; GGT: Gamma-Glutamyl Transferase; AST: Aspartate transaminase; ALT: Alanine Transaminase; MRCP: Magnetic Resonance Cholangiopancreatography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fábio V (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Fábio V, José C, Rui E, Aires M, Carolina M, Alberto M. An unexpected diagnosis: Metastasis of the gallbladder from breast cancer - A case report. Open J Clin Med Case Rep. 2023; 2130.
Introduction
Breast Cancer (BC) is nowadays the most frequently diagnosed cancer worldwide. The most recent data estimate that there were over 2 million incident BC cases in 2020 and that BC is the leading cause of cancer mortality in females all over the world [1]. At the moment of initial diagnosis, almost 60% of the patient have lymph or distant organ metastases, and about 30 to 80% will develop metastatic disease following treatment (surgery, chemotherapy, radiotherapy, and/or hormonotherapy) [2].
This malignancy is a complex disease with a broad spectrum of clinical and subclinical presentations. It is often associated with the local and lymphatic spread and with metastatic disease of the lungs, liver, and bones. It can also spread to the central nervous system at a minor rate compared to the ones mentioned before. Pericardium, eye, abdominal cavity, and endocrine organs are infrequently involved [3]. Following this, metastasis in the extrahepatic digestive system is rare and typically appears after a long latent period, which can take up to 20 years [4].
Malignancy of the gallbladder is uncommon, in fact, metastatic lesions of the gallbladder are an uncommon clinical condition. When these lesions happen in most cases the metastases originate from malignant melanoma, renal cancer, and cervical carcinoma [5,6].
The gallbladder is an extremely rare organ to be involved in BC and only a few cases have been reported in the literature [2].
In this case report we present a report of a gallbladder metastasis from a patient with BC following a review of the literature for similar cases and an overview of this condition.
Case Report
A 74-year-old female was diagnosed with left BC in November 2008 and was submitted to a left total mastectomy with sentinel node biopsy. The histologic results showed an invasive lobular carcinoma ER, PR, and HER2 positive-T1N0M0. The patient then went through 5 years of treatment with tamoxifen.
In January 2015 a regional recurrence was detected (new left node) and in march 2015 a total axillary dissection was performed. The histologic results showed carcinoma in 14 of the 19 nodes that were removed -RE<10%, RP 50%, and HER negative. Then the patient went through adjuvant radiotherapy until October 2015 and by the decision of the Oncology group the patient started adjuvant hormonotherapy with letrozole in September 2015 to continue until 2025.
The patient continues to be followed in routine appointments and in June 2020 did mammography and a breast ultrasound that were normal, without signs of recurrence.
In August 2021 the patient presented at the surgical emergency room with abdominal pain associated with vomiting and anorexia that had started one week before. The patient described the abdominal pain as mainly epigastric and in the right hypochondrium, associated with nausea and vomiting. Fever, diarrhoea, acholuria, acholia or any other symptoms were denied.
As medical history, this was a patient that had (besides the history of BC) arterial hypertension, dyslipidaemia, and urinary incontinence and therefore medicated accordingly. In the physical examination, the patient was anxious but apyretic, with normal blood pressure and heart rate. She was hydrated, ruddy, anicteric, and eupnoeic. On abdominal examination, there was diffuse tenderness without guarding or other signs of peritoneal irritation. Vesicular Murphy’s sign was negative. Renal murphy was also negative.
The patient blood tests at admission revealed a normal haemoglobin, with blood cell count and CRP value. Bilirubin levels, ALP, GGT, AST and ALT were also in the normal range value. Amylase and Lipase were also negative. An abdominal ultrasound was preformed and it exhibited a small dilation of the common bile duct and signs of gallbladder lithiasis.
The patient complete symptomatic treatment and then was discharge with a scheduled General Surgery consult.
Investigation
In September 2021 the patient went to the appointment. At the moment, she was asymptomatic with a normal physical exam. A Magnetic Resonance Cholangiopancreatography (MRCP) and blood tests were ordered, and a follow-up consult was scheduled.
In November 2021 the patient performed a MRCP that exhibited very suggestive radiological signs of microlithiasis of the gallbladder with no intra and extrahepatic bile ducts described as normal and without dilation of the biliary system. The liver and the pancreas were also described as normal.
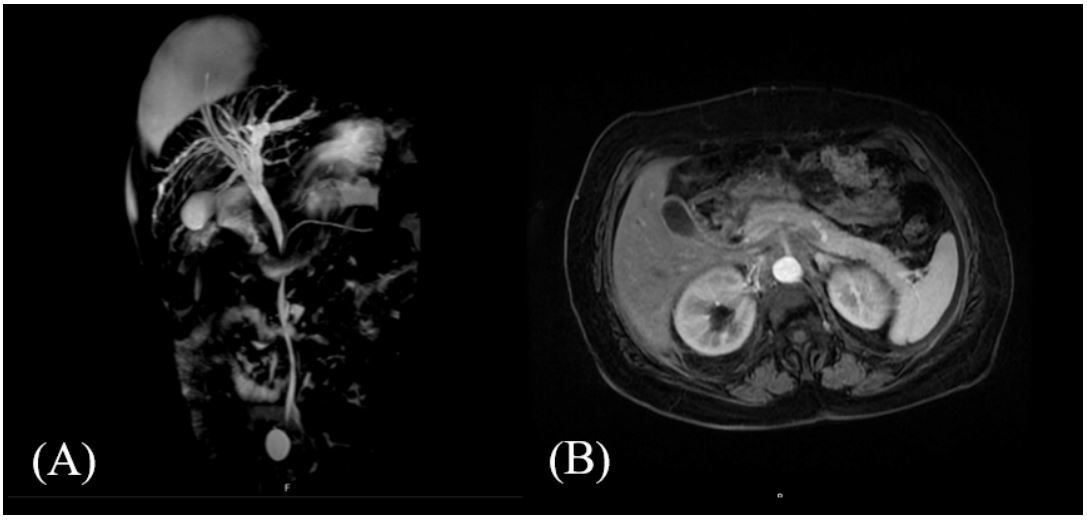
Figure 1: (A) Coronal section of a MRCP that shows the biliary tree. (B) Axial section of a MRCP in
which we can see the gallbladder with suggestive radiological signs of microlithiasis.
Then, in the follow-up appointment a laparoscopic cholecystectomy was proposed to the patient and she consented.
Surgery and Histology
The laparoscopic cholecystectomy took place in March 2022. At the inspection of the abdominal cavity, there were signs of chronic cholecystitis. The surgical procedure went perfectly without any complications. However, a surgical drain was left in the right flank. The postoperative period was uneventful and the patient was discharged 8 days after surgery and reassessed in consultation.
The histological evaluation was compatible with carcinoma, in which morphological and immunocytochemical features were compatible with metastasis of the preview diagnosed BC.
The patient was reassessed in consultation 2 weeks after surgery and was asymptomatic and with no complications from the surgery. However, in April 2022 the patient presented at the emergency room with blurred vision and, right orbital cellulitis was diagnosed. After investigation, it was found an eye metastasis of lobular BC. The patient is now stable and being followed by an oncology team
Discussion
Primary gallbladder malignancy is rare in most developed countries. Risk factors related to this kind of cancer include chronic cholecystitis, porcelain gallbladder, anomalous pancreaticobiliary duct junction, gallbladder polyp (which has a prevalence of 3 to 7% in the adult population), gallbladder chronic infection by some bacteria (Salmonella species, S. paratyphi and S. typhican), occupational exposure to Benzene, tobacco consumption, use of oral contraceptives and genetic factors [8,9].
BC is more frequently associated with metastatic disease of the lungs, liver, and bones. And, gallbladder metastasis from BC is very rare. According to the literature, lobular breast cancers are more likely to metastasize to the gastrointestinal tract compared to ductal breast cancers and this fact is not well understood yet [4]. Metastatic disease of lobular breast carcinomas presents preference for peritoneum/retroperitoneum, the gastrointestinal system (including gallbladder), and gynaecologic organs [3].
When it comes to the metastatic disease of the gallbladder, the literature reports that the most frequent carcinomas that are associated with gallbladder metastasis are melanoma, renal cell carcinoma, and cervical carcinoma [10]. Metastasis to the gallbladder is strongly associated with a poor prognosis due to a higher probability of widespread metastatic disease from the primary tumor [3].
In terms of clinical presentation of metastasis of the gallbladder, signs and symptoms of acute, and chronic cholecystitis and abdominal pain prevail [2,3]. As we saw in this case report, the patient came to the emergency room with abdominal pain and other symptoms that were compatible with biliary colic, and as mentioned before, at surgery, there were signs of chronic cholecystitis. However, there are other kinds of clinical presentations. Shah, RJ et al. [11] reported a more severe clinical presentation-bile peritonitis, which demanded an exploratory laparotomy. This team found a fragmented, necrotic gallbladder that histological exam later revealed a primary breast carcinoma. Unfortunately, this patient died 5 days after surgery to a declining clinical state and the autopsy revealed diffuse carcinomatosis involving the peritoneum, the gastrointestinal tract, and pleura.
In contrast to the cases above described, asymptomatic cases had also been reported. Riaz N et al. [12] described a case of a 42-year-old premenopausal woman with diagnosed BC that was submitted to an abdominal ultrasound that showed a focal area of thickening in the body of the gallbladder without any stones or sludge, with normal bile ducts. This patient had a bone scintigraphy that was suspicious for possible areas of diffuse metastatic disease. With those findings, a diagnostic laparoscopy with or without laparoscopic cholecystectomy was considered. Diagnostic laparoscopy showed a thick-walled gallbladder and a laparoscopic cholecystectomy was performed. Histopathology findings were compatible with metastatic disease of BC.
Conclusion
The present case report exhibits an extremely rare condition. However, gallbladder metastasis from a patient with BC, especially lobular BC cannot be neglected. Those patients usually present with abdominal pain and signs of acute or chronic cholecystitis, but can also present as asymptomatic.
Therefore, although clinicians normally do not associate BC with gallstone disease due to its rarity, when a patient with a BC history is admitted, we must take into account that gallbladder metastatic disease is a possibility especially if the patient has signs of local and/or lymphatic spread.
Disclosure: The authors declare no conflict of interest.
References
- Wilkinson L, Gathani T. Understanding breast cancer as a global health concern. The British Journal of Radiology. 2022; 95: 20211033.
- Giulia M, Serra F, Giorgia P, Aurelio RA, Lucio B, et al. Case report: Metastatic breast cancer to the gallbladder. F1000Research. 2020; 9.
- Zagouri F, Sergentanis TN, Koulocheri D, Nonni A, Bousiotou A, et al. Bilateral synchronous breast carcinomas followed by a metastasis to the gallbladder: a case report. World Journal of Surgical Oncology. 2007; 5: 1-4.
- Abdelilah B, Mohamed O, Yamoul R, Elkhiyat I, Al Bouzidi A, et al. Acute cholecystitis as a rare presentation of metastatic breast carcinoma of the gallbladder: A case report and review of the literature. The Pan African medical journal. 2014; 17.
- Fleres F, Rossitto M, Foti A, Macrì A, Cucinotta E. Metastasis of the gallbladder from the breast cancer. Ann Ital Chir. 2014; 85: S2239253X14023470.
- Di Vita M, Zanghì A, Lanzafame S, Cavallaro A, Piccolo G, et al. Gallbladder metastases of breast cancer: from clinical-pathological patterns to diagnostic and therapeutic strategy. Clin Ter. 2011; 162: 451-6.
- Murguia E, Quiroga D, Canteros G, SanMartino C, Barreiro M, et al. Gallbladder metastases from ductal papillary carcinoma of the breast. Journal of Hepato-Biliary-Pancreatic Surgery. 2006; 13: 591-593.
- Gautam A, Pandey A, Masood S, Chauhan S, Choudhary D, et al. Incidental gallbladder carcinoma in gallbladder polyps: challenges of gallbladder malignancy for an endemic population. The Malaysian Journal of Medical Sciences: MJMS. 2021; 28: 27.
- Sharma A, Sharma KL, Gupta A, Yadav A, Kumar A. Gallbladder cancer epidemiology, pathogenesis and molecular genetics: Recent update. World journal of gastroenterology. 2017; 23: 3978.
- Scully OJ, Bay BH, Yip G, Yu Y. Breast cancer metastasis. Cancer genomics & proteomics. 2012; 9: 311-320.
- Shah RJ, Koehler A, Long JD. Bile peritonitis secondary to breast cancer metastatic to the gallbladder. The American Journal of Gastroenterology. 2000; 95: 1379.
- Riaz N, Ahmed R, Afzal S, Masood N. Breast carcinoma with asymptomatic metastasis to the gallbladder. Singapore Med J. 2012; 53: e136-8.
