
Open Access, Volume 9
A novel epidermal nevus syndrome associated with congenital pulmonary airway malformation
Cristina Gioioso-Datta1#; Bianca Russell2#; Kathryn E Singh3 ; Stephen Romansky4 ; Rudolf Happle5 ; Virginia E Kimonis3*
1Department of Obstetrics and Gynecology, University of California, Irvine, California, USA.
2Department of Human Genetics, Cincinnati Children’s Medical Center, Cincinnati, Ohio, USA.
3Division of Genetic and Genomic Medicine, Department of Pediatrics, University of California, Irvine, California, USA.
4Department of Pathology, Memorial Hospital, Long Beach, California, USA.
5Department of Dermatology, Freiburg University Medical Center, Freiburg, Germany
Virginia Kimonis
Professor, Department of Pediatrics, UC Irvine Division of Genetics and Genomic Medicine, University of
California-Irvine Medical Center, 101 The City Drive South, ZC4482, Orange CA 92868, USA.
Tel: 714-456-5791; 714-456-5330 & 949-266-7946;
Email: vkimonis@uci.edu
Received : Aug 16, 2023,
Accepted : Sep 29, 2023
Published : Oct 06, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Epidermal nevus syndromes involve a group of disorders characterized by the type of epidermal nevus and are associated with an extracutaneous abnormality. Most epidermal nevus syndromes involve skin lesions associated with central nervous system, ocular or skeletal anomalies. We report a previously undescribed type of epidermal nevus syndrome in a preterm infant. The face and mouth were remarkable for large exophytic verrucous lesions and extensive pedunculated tumors involving the scalp. The infant was additionally affected by type 3 Congenital Pulmonary Airway Malformation (CPAM). Microscopic examination of the skin lesions revealed multiple layers of immature epithelium and the complete absence of adnexal structures. Chromosomal microarray analysis demonstrated no abnormalities. Family history was significant for numerous maternal relatives with multiple first and second trimester pregnancy losses. The distribution of lesions in this patient was characteristic of postzygotic mosaicism. We believe this case may represent a new histological subtype of epidermal nevi associated with a CPAM lesion. Future molecular research may indicate whether this disorder may be categorized as a distinct entity.
Keywords: Epidermal nevus syndrome; Keratinocytic nevus; Congenital cystic adenomatoid malformation (CCAM); Epidermis; Nevus; Congenital abnormalities.
Copy right Statement:Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kimonis V (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Gioioso-Datta C, Russell B, Singh KE, Romansky S, Happle R. A novel epidermal nevus syndrome associated with congenital pulmonary airway malformation. Open J Clin Med Case Rep. 2023; 2126.
Introduction
Epidermal nevus syndrome is a general term for a group of disorders distinguished by the type of associated epidermal nevus either organoid, referring to sebaceous glands and hair follicles, or keratinocytic, referring to the epidermis. The appearance of the epidermal nevi varies according to the type of tissue that is overgrown. The lesions are thought to originate from a postzygotic mutation during the development of the embryonal ectoderm and usually-follow the lines of Blaschko [1-5]. The usual associated anomalies include skeletal, CNS, eye, and rare cardiac abnormalities [6]. Well-defined syndromes characterized by organoid epidermal nevi comprise Schimmelpenning syndrome including phacomatosis pigmentokeratotica, nevus comedonicus syndrome, angora hair nevus syndrome, and Becker nevus syndrome [7]. The molecular basis of these disorders has so far not been identified, except for schimmelpenning syndrome including phacomatosis pigmentokeratotica [8,9]. By contrast, the group of syndromes characterized by keratinocytic nevi comprises five phenotypes with a known molecular etiology in the form of CHILD (Congenital Hemidysplasia with Ichthyosiform nevus and Limb Defects) syndrome, type 2 segmental PTEN hamartoma syndrome fibroblast growth factor receptor 3 epidermal nevus syndrome (Garcia-Hafner-Happle Syndrome). Proteus syndrome, and CLOVES syndrome [7].
We report a new epidermal nevus syndrome characterized by large exophytic verrucous lesions of the head and type 3 Congenital Pulmonary Airway Malformation (CPAM). A review of the literature revealed only one reported case of large pedunculated facial and scalp lesions associated with pulmonary airway malformations [8]. However, the skin lesions were identified by gross appearance rather than by histopathology. To our knowledge, the histopathological characteristics of our case are distinct from those described with any other epidermal nevus.
Materials and Methods
Clinical case
The female infant was born to a healthy 17-year-old mother and an 18-year-old father at 25 weeks gestation. The pregnancy was complicated by polyhydramnios first diagnosed at 22 weeks. The mother had presented to our facility at 25 weeks with severe pre-eclampsia. On admission, fetal ultrasound revealed a large solid chest mass displacing the heart to the right with deviation of the mediastinum suggestive of a CPAM with no evidence of hydrops. Given the diagnosis of severe preeclampsia, an induction of labor was initiated. The patient was counseled extensively regarding the likely lethal fetal anomaly at a severely premature gestational age, and a decision was made for no fetal monitoring during labor. A female infant was delivered vaginally with an Apgar score of 1 at one minute and 1 at five minutes and a birth weight of 945 gm (normal 655+/-105 gm). Per the family’s wishes at the time of delivery, the infant was resuscitated and intubated. A chest x-ray revealed a large thoracic mass involving the entire left lung and the right upper lobe. Despite maximum ventilatory support, adequate oxygen saturation could not be maintained and the infant expired within a few hours of life.
Results
Gross and pathologic examination
Gross examination of the infant revealed extensive verrucous and papillomatous lesions on the scalp and forehead. These lesions were solid and pink in color and appeared as bilateral symmetrical plates on the scalp involving the ears causing deformation of the pinnae. The lesions followed the lines of Blaschko. Several lesions streaked down the right side of the face and left temple and extended down the nose and around the mouth. The oral lesions were observed to stop at the gingival mucosa. The scalp was intermixed with fleshy tags, verrucous lesions, and normal areas of skin covered with hair. Smaller lesions extended over the shoulders and on the right forearm, ending in a linear distribution of minor lesions on the hands and feet (Figure 1). Otherwise, there were no facial defects, limb deformities, asymmetry, or other birth defects.
Autopsy revealed a thoracic mass involving the entire left lung and right upper lobe, which had expanded to fill the pleural cavity. The lung mass was histopathologically classified as type 3 CPAM with cut surfaces showing cystically dilated spaces up to 0.2 cm in dimension throughout the lung parenchyma (Figure 2). Other findings included bilateral 0.2 cm adrenal nodules and small intraventricular hemorrhages. The placenta was noted to have features of chronic uteroplacental insufficiency. No other significant abnormalities were noted.
Microscopic examination of the skin lesions revealed an extensive exophytic, papillomatous epidermal proliferation (Figure 3). The abnormally broad epidermis was comprised of a duplication of simple immature epithelium consisting of clear cells without evidence of significant differentiation into epidermal cell layers. The epithelial cells exhibited a glycogen-rich clear cytoplasm, confirmed by PeriodicAcid Schiff stain, and lack of maturation. Absence of the granular layer was noted. The typical dermal underlying adnexal structures such as immature sebaceous glands or hair follicles were absent. Viral inclusions were not identified.
Microarray analysis of blood performed using the Genzyme 44K oligonucleotide v1.1 array was normal [arr(1-22,X)x2].
Family history
This infant was the second pregnancy for her non-consanguineous parents. Their first pregnancy resulted in a spontaneous miscarriage at 2-3 months gestation. The infant’s maternal grandmother had four pregnancies with the infant’s grandfather, all of which were delivered prior to 34 weeks, including two twin gestations. The maternal grandmother also had six pregnancy losses (2 to 7 months gestation) with a prior partner over a three-year span. To the family’s knowledge, all autopsies were normal and no genetic testing was performed on any of the fetuses. The infant’s paternal grandmother experienced one spontaneous miscarriage at 3-4 months gestation. Family history was otherwise non-contributory. The infant is of mixed Mexican Indio, Spanish, Cherokee Indian, Scottish, Irish, German, and English descent.
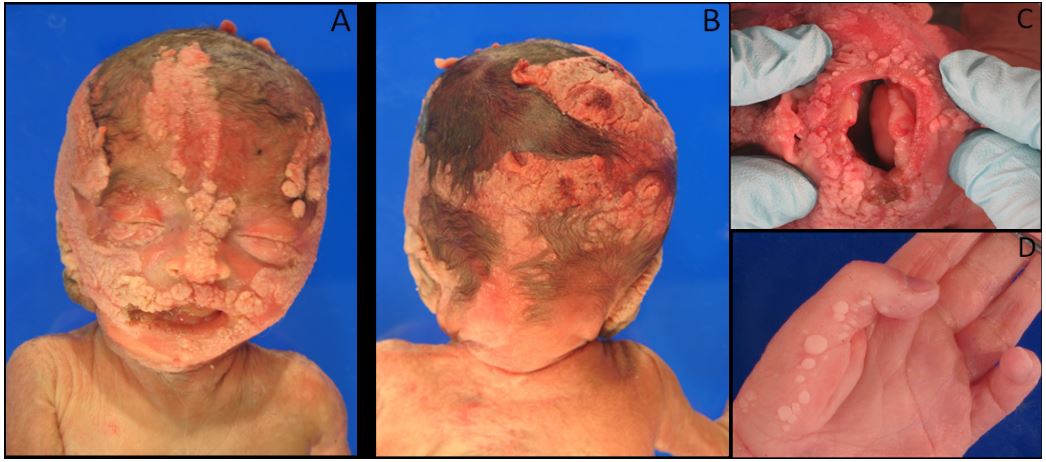
Figure 1: Lesions on the infant’s face (A), occiput (B), perioral region (C), and hand (D).
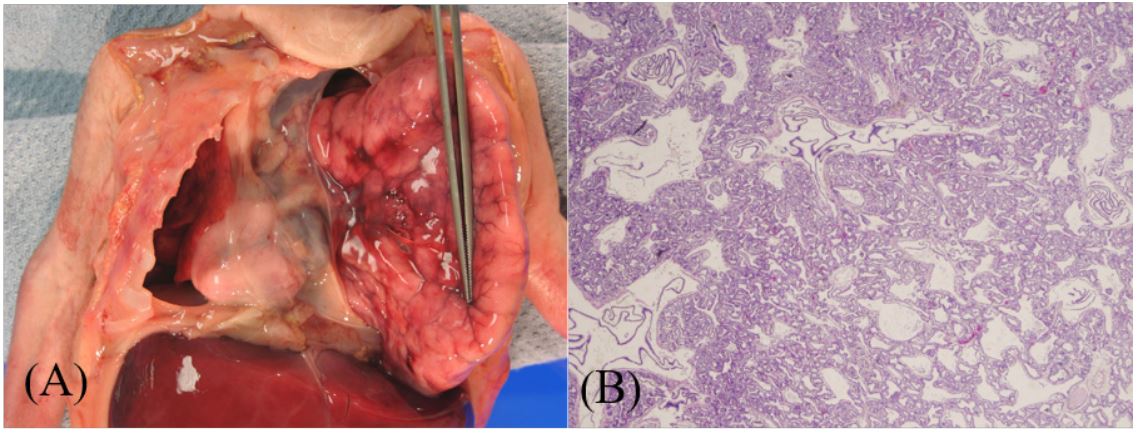
Figure 2: Gross appearance of congenital pulmonary airway malformation of the left lung, which has been retracted
to reveal the displacement of the heart to the right and pulmonary hypoplasia of the right lung (A). Histology of
cystic pulmonary lesions with adenomatous overgrowth of the terminal bronchioles and a consequent absence of
alveolar growth at 2x magnification (B).
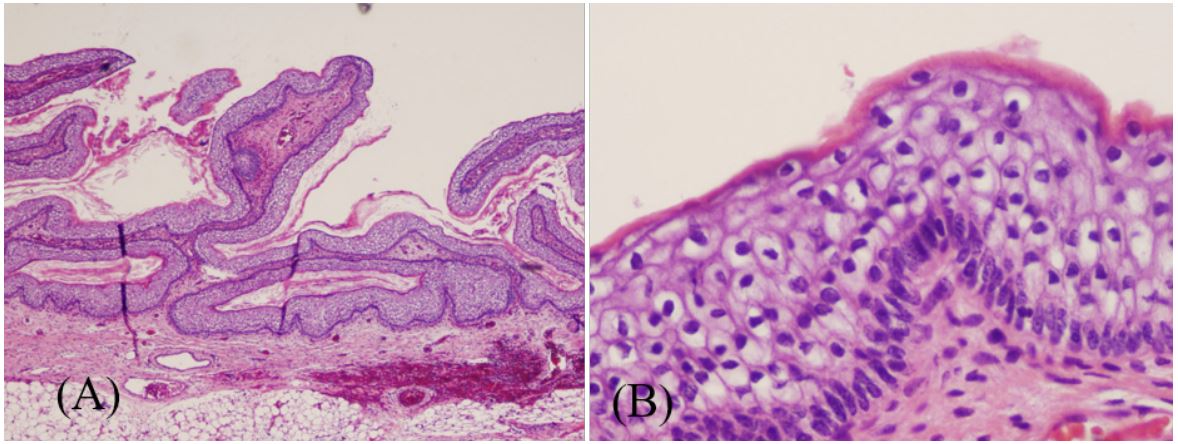
Figure 3: Gross appearance of congenital pulmonary airway malformation of the left lung, which has been retracted
to reveal the displacement of the heart to the right and pulmonary hypoplasia of the right lung (A). Histology of
cystic pulmonary lesions with adenomatous overgrowth of the terminal bronchioles and a consequent absence of
alveolar growth at 2x magnification (B).
Discussion
We have classified our patient as having an Epidermal Nevus Syndrome (ENS) given the presence of epidermal nevus associated with an extracutaneous feature [6,9]. Initially, the systematized nevus was grossly considered to be a nevus sebaceus, but the typical histopathological features of immature hair follicles and sebaceous glands were absent [6]. Other cases have been reported of isolated large, papillomatous, pedunculated nevus sebaceus lesions that grossly resemble our patient’s lesions but that differ histologically [10,11]. Moreover, as far as we could ascertain from the literature, there is no description of a nevus with the histology of duplication of immature clear cells and an epithelium with absence of both mature keratinocytes and adnexal structures. In addition, the prematurity of the infant cannot account for the findings in this epidermis, as the skin from a 25-week-old scalp should show evidence of differentiation into the various cell layers and increased keratinization. Immature sebaceous glands and hair follicles of the scalp would also be present at this gestational age [12].
The lung masses were histopathologically classified as CPAM 3 which comprises 5-10% of all CPAMs. As with our patient, when pulmonary malformation is large enough to cause a mass effect on lung and cardiopulmonary vasculature, poor fetal and neonatal outcomes result due to pulmonary hypoplasia, heart failure, and hydrops [13]. This malformation is thought to arise from an insult early in gestation causing a dysregulation of developmental factors during the canalicular phase leading to overgrowth of terminal respiratory bronchioles and lack of alveoli [14]. Increased expression of the HOXB5 gene in CPAM tissue has been proposed as a likely mechanism of CPAM genesis given its critical role in cell apoptosis and proliferation as well as branching morphogenesis [15]. Mice induced to over-express Fibroblast Growth Factor 7 (FGF7) are found to have CPAM-like phenotypes [16], but no change in expression of FGF7 has been found in human CPAM versus normal lung tissue [17]. FGF7 has also been found to play a central role in epithelial wound healing leading us to hypothesize that over-expression of FGF7 may be implicated in overgrowth of epithelial tissue [18]. We have also considered an over-expression of FGF7 to be a molecular mechanism for overgrowth of lung and epithelial tissue in our patient as it has been implicated in both lung and epidermal tissue tumors [17,18].
Given the lung and epidermal findings, an insult could have occurred early in embryonic development leading to a mosaic somatic mutation affecting regulation of tissue growth causing a dysplastic overgrowth syndrome. The severe and lethal phenotype of our patient could be due to a high percentage of affected somatic cells [19]. Recently, the PIK3CA pathway has been implicated in several overgrowth syndromes with cutaneous findings including Proteus and CLOVES (Congenital, Lipomatous, Overgrowth, Vascular Malformations, Epidermal Nevi and Spinal/Skeletal Anomalies and/or Scoliosis) syndrome [20,21]. Another possible mechanism is the dysregulation of the RAS/MPK pathway, which has been associated with many overgrowth and tumor syndromes [22]. Mosaic activating RAS mutations have been associated with keratinocytic and sebaceous epidermal nevi [4,5,23]. Costello syndrome caused by somatic H-RAS mutation mosacisim, is also associated with papillomata, and it has been suggested there may be pulmonary airway involvement [24-26]. An association with K-Ras, β-catenin and FGFR3 mutations in mice has been found to cause lung and epithelial tumors [27]. These are promising molecular mechanisms for our novel syndrome but presently we are unable to correlate these theories with molecular data. Clarification of the molecular pathway in this unique disorder has implications for genetic counseling for this family and for understanding the pathogenesis of other overgrowth syndromes with cutaneous findings.
Declarations
Conflict of interest statement: All authors report no conflicts of interest.
Acknowledgements: The authors wish to thank the staff of the Division of Genetics and Genomic Medicine, Department of Pediatrics and Department of Obstetrics and Gynecology at the University of California Irvine and Long Beach Memorial as well as the Department of Pathology at Memorial Hospital in Long Beach, California for their assistance in the care of this patient.
References
- Moss C, Larkins S, Stacey M et al. Epidermal mosaicism and Blaschko’s lines. J Med Genet 1993: 30(9): 752-755.
- Paller AS, Syder AJ, Chan Y et al. Genetic and clinical mosaicism in a type of epidermal nevus. New Eng J Med 1994: 331(21): 1408-1415.
- Garcia-Vargas A, Hafner C, Perez-Rodriguez AG et al. An epidermal nevus syndrome with cerebral involvement caused by a mosaic FGFR3 mutation. Am J Med Genet A 2008: 146A(17): 2275-2279.
- Bourdeaut F, Hérault A, Gentien D et al. Mosaicism for oncogenic G12D KRAS mutation associated with epidermal nevus, polycystic kidneys and rhabdomyosarcoma. J Med Genet 2010: 47(12): 859-862.
- Hafner C, Toll A, Gantner S et al. Keratinocytic epidermal nevi are associated with mosaic RAS mutations. J Med Genet 2012: 49(4): 249-253.
- Happle R. The group of epidermal nevus syndromes. Part I: Well defined phenotypes. J Am Acad Dermatol 2010: 63(1): 1-22.
- Happle R. Mosaicism in Human Skin: Understanding Nevi, Nevoid Skin disorders, and Cutaneous Neoplasia. Berlin, Springer 2014.
- Groesser L, Herschberger E, Ruetten A et al. Postzygotic HRAS and KRAS mutations cause nevus sebaceus and Schimmelpenning syndrome. Nat Genet 2012: 44(7): 783-7.
- Groesser L, Herschberger E, Sagrera A et al. Phacomatosis pigmentokeratotica is caused by a postzygotic HRAS mutation in a multipotent progenitor cell. J Invest Dermatol 2013; 133(8): 1998-2003.
- Sweeney WJ, Kuller J, Chescheir NC, Veness-Meehan K. Prenatal ultrasound findings of linear nevus sebaceous and its association with cystic adenomatoid malformations of the lungs. Obstet Gynecol 1994: 83(5 Pt 2): 860-862.
- Solomon LM, Fretzin DF, Dewald RL. The epidermal nevus syndrome. Arch Dermatol 1968: 97(3): 273-285.
- Correale D, Ringpfeil F, Rogers M. Large, papillomatous, pedunculated nevus sebaceous: a new phenotype. Pediatr Dermatol 2008: 25(3): 355-358.
- Lin HC, Lee JY, Shieh SJ, Hsu CK. Large papillomatous and pedunculated nevus sebaceous. J Dermatol 2011: 38(2): 200-202.
- Ersch J, Stallmach T. Assessing gestational age from histology of fetal skin: an autopsy study of 379 fetuses. Obstet Gynecol 1999: 94(5 Pt 1): 753-757.
- Mann S, Wilson RD, Bebbington MW, Adzick NS, Johnson MP. Antenatal diagnosis and management of congenital cystic adenomatoid malformation. Semin Fetal Neonat Med 2007: 12(6): 477-481.
- Stocker JT, Madewell JE, Drake RM. Congenital cystic adenomatoid malformation of the lung. Classification and morphologic spectrum. Hum Pathol 1997: 8(2): 155-171.
- Volpe MV, Pham L, Lessin M et al. Expression of Hoxb-5 during human lung development and in congenital lung malformations. Birth Defects Res A Clin Mol Teratol 2003: 67(8): 550-556.
- Simonet WS, DeRose ML, Bucay N et al. Pulmonary malformation in transgenic mice expressing human keratinocyte growth factor in the lung. Proc Natl Acad Sci U S A 1995: 92(26): 12461–12465.
- Liechty KW, Quinn TM, Cass DL, Flake A, Adzick NS. Elevated platelet-derived growth factor-B in congenital cystic adenomatoid malformations requiring fetal resection. J Pediatr Surg 1999: 34(5): 805–809.
- Werner S, Smola H, Liao X et al. The function of KGF in morphogenesis of epithelium and reepithelialization of wounds. Science 1994: 266(5186): 819-822.
- Happle R. Lethal genes surviving by mosaicism: a possible explanation for sporadic birth defects involving the skin. J Am Acad Dermatol 1987: 16(4): 899–906.
- Lindhurst MJ, Parker VER, Payne F et al. Mosaic overgrowth with fibroadipose hyperplasia is caused by somatic activating mutations in PIK3CA. Nat Genet 2012: 44(8): 928-933.
- Kurek KC, Luks VL, Ayturk UM et al. Somatic mosaic activating mutations in PIK3CA cause CLOVES syndrome. Am J Hum Genet 2012: 90(6): 1108-1115.
- Tidyman WE, Rauen KA. The RASopathies: developmental syndromes of Ras/MAPK pathway dysregulation. Curr Opin Genet Dev 2009: 19: 230-236.
- Groesser L, Herschberger E, Ruetten A et al. Postzygotic HRAS and KRAS mutations cause nevus sebaceous and Schimmelpenning syndrome. Nat Genet 2012: 44(7): 783-787.
- Gripp KW, Stabley DL, Nicholson L, Hoffman JD, Sol-Church K. Somatic mosaicism for an HRAS mutation causes Costello syndrome. Am J Med Genet A 2006: 140A(20): 2163–2169.
- Lo IF, Brewer C, Shannon N et al. Severe neonatal manifestations of Costello syndrome. J Med Genet 2008: 45(3): 167-171.
- Myers A, Brennan ML, Bernstein J, Hudgins L. Respiratory tract involvement in Costello Syndrome results in significant morbidity. Presented by Hudgins L at 33rd Annual David W. Smith Workshop on Malformations and Morphogenesis. Lake Lanier, Georgia, 2012.
- Ahmad I, Singh LB, Foth M et al. K-Ras and β-catenin mutations cooperate with Fgfr3 mutations in mice to promote tumorigenesis in the skin and lung, but not in bladder. Dis Model Mech 2011: 4(4): 548-555.
