
Open Access, Volume 9
A study on the prediction of kallistatin levels in the development and progression of pre-eclampsia
Shihua Li1†; Lu Zeng1†; Mingxiao Chen2*; Wenyan Geng2*; Ping Yin1*
1Department of Clinical Laboratory Medicine, The Third Affiliated Hospital of Guangzhou Medical University, Guangzhou Guangdong, China.
2Department of Clinical Laboratory Medicine,The Second Affiliated Hospital of Guangzhou Medical University, Guangzhou Guangdong, China.
3Department of Blood Transfusion, The Third Affiliated Hospital of Guangzhou Medical University, Guangzhou Guangdong, China.
†Equal Contribution.
Mingxiao Chen*
Department of Clinical Laboratory Medicine,The Second Affiliated Hospital of Guangzhou Medical University, Guangzhou Guangdong, China.
Wenyan Geng*
Department of Blood Transfusion, The Third Affiliated Hospital of Guangzhou Medical University, Guangzhou Guangdong, China.
Ping Yin*
Department of Clinical Laboratory Medicine, The Third Affiliated Hospital of Guangzhou Medical University, Guangzhou Guangdong, China.
Email: 735488852@qq.com
Received : Aug 14, 2023,
Accepted : Sep 29, 2023
Published : Oct 06, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Objective: To explore the expression level of kallistatin in plasma of patients with Pre-Eclampsia (PE) and the predictive value of kalistatin and other parameters in before 20 weeks of pregnancy for PE.
Methods: The peripheral blood plasma of pregnant women with gestational age less than 20 weeks was collected indiscriminately from 2020 to 2022 in the obstetrics clinic of the Third Affiliated Hospital of Guangzhou Medical University, and follow up until the end of the labor process. Enzyme-Linked Immunosorbent Assay (ELISA) was used to quantitatively detect the plasma kallistatin level and analyzes the difference of kallistatin levels between pregnant women with PE and normal pregnancy. We utlized ROC curve to explore the predictive value of Kallistatin for preeclampsia.Subsequently, we explore the correlation between kallistatin level and other parameters, such as pregnancy blood pressure (after 20 weeks), Maternal Mass Index (BMI), White Blood Cell (WBC), Platelet (PLT), glutamic oxalacetic transaminase (AST), Alanine Aminotransferase (ALT), Creatinine, Uric Acid (UA), Hemoglobin (HGB), Total Cholesterol (TC), Triglyceride (TG) and total days of pregnancy.
Results: The plasma kallistatin level of preeclampsia patients is higher than that of normal pregnant women with gestational age matching (6.96 ± 0.80 vs. 6.32 ± 1.00 ug/mL, P<0.05). Besides, the differences of Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), creatinine, delivery pregnany week and WBC between two groups were statistically different. ROC analysis revealed that the cut-off value of plasma kallistatin of predicting preeclampsia is 6.64 ug/ml (AUC=0.707, Youden Index=0.456, 95% CI: 0.547-0.867, P<0.05, Sensitivity=80%, Specificity=65.6%). When combined kallistatin with WBC, AUC=0.701, Sensitivity =81.8%, Specificity=57.1%.
After correlation analysis, plasma kallistatin was negatively correlated with PLT in PE patients (Spearman correlation coefficient=-0.687, P=0.028) and positively correlated with AST (Spearman correlation coefficients = 0.836, P=0.001) and TC (Spearman correlation coefficients = 0.745, P=0.008). In pregnant women, however, plasma kallistatin was negatively correlated with ALT (Spearman correlation coefficient =0.229, P=0.044), creatinine (Pearson correlation = -0.247, P=0.029) and UA (Pearson correlation = -0.242, P=0.036).
Conclusion: The plasma kallistatin level was significantly increased in pre-eclampsia women before 20 weeks of pregnancy when compared with normal pregnant women. Plasma kallistatin is a potential biomarker to predict PE before 20 weeks of pregnancy.
Keywords: Kallistatin; Preeclampsia; Biomarker; Predict.
Copy right Statement:Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Chen M, Geng W, Yin P (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Li S, Zeng L, Chen M, Geng W, Yin P. A study on the prediction of kallistatin levels in the development and progression of pre-eclampsia. Open J Clin Med Case Rep. 2023; 2125.
Introduction
Pre-Eclampsia (PE), is a clinical syndrome that occurs after 20 weeks of gestation which eventually leads to maternal hypertension, proteinuria and other multi-system organ dysfunction due to placental and maternal disease [1]. Pre-eclampsia is a common cause of intrauterine growth restriction, fetal malformation and maternal death. It is estimated that 2-8% of pregnancies in the world are complicated by preeclampsia [2]. In Latin America and the Caribbean, hypertension causes almost 26% of maternal deaths, while in Africa and Asia, hypertension causes 9% of maternal deaths. Although the maternal mortality rate in high-income countries is much lower than that in the developing countries, 16% of maternal mortality can be attributed to hypertension [3]. At the moment, the pathogenesis of pre-eclampsia is still unclear. Studies have shown that the pathogenesis is related to endothelial cell dysfunction, insufficient uterine spiral artery remodeling [4,5], placental oxygenation, over-activation of inflammation and immunity, and the imbalance between angiogenesis and anti-angiogenic factors. Early Pre-clampsia is characterized by hypertension and proteinueia, and may cause renal dysfunction, liver damage, decreased platelets count, blurred vision and dizzy. Risk factors include first-time mothers, multiple pregnancies, young women (<18 years old) olderly women (≥40 years old); gestation interval ≥10 years, history of pre-eclampsia, history of chronic hypertension, chronic kidney disease, diabetes and thrombotic disease, malnutrition and obesity [6]. With the delay of the age of marriage and childbearing in China, more and more elderly pregnant women appeared which increases the incidence of various pregnancy complications. Because it is hard to recognize early signs of pre-eclampsia, and once it occurred, it will progress rapidly, and do harm to the health of mother and fetus. Therefore, early prediction of pre-clampsia is very important. Up to date, sFlt1/PIGF was found to be a good biomarker of early-onset pre-clampsia after 20 weeks [7-12], but there is no specific marker before 20 weeks.
Kallistatin is a serine protease inhibitor, also known as tissue kallikrein binding protein, and an endogenous angiogenesis inhibitor. Kallistatin is mainly produced in liver, vascular smooth muscle cells and endothelial cells [13], which has many biological functions, including regulating blood pressure, preventing inflammation, vasodilation and stimulating neointimal hyperplasia. Kallistatin has two functional parts, including an active part and a heparin-binding part. While it inhibits the tissue kallikrein, it stimulates endothelial Nitric Oxide Synthase (NOS) [14], sirtuin 1, and cytokine three signal suppressors’ expression through its active part. It inhibits many growth factors as well as cytokines, such as Vascular Endothelial Growth Factor (VEGF), Tumor Necrosis Factor-α (TNF-ɑ), High-Mobility Group Protein 1 (HMG-1), Wnt, Tumor Growth Factor-β (TGF-β) and Epidermal Growth Factor (EGF) through its heparin-binding part [14-15]. Kallistatin plays a dual role in vascular repair. Heparin-binding part inhibits angiogenesis by interfering with angiogenesis factor VEGF-mediated vascularization and inhibiting VEGF expression, while kallistatin promotes angiogenesis and vascular repair by stimulating the fluidity and function of Endothelial Progenitor Cells (EPCs) through its active site [16]. Besides, it has been found that kallistatin can regulate the key enzyme KLK1 [17] in the Kinin System (KKS), and its metabolism and activity are regulated by kallistatin. Kallistatin can play an anti-inflammatory role by inhibiting the activity of KLK1 [18] and affecting the KLK1-Kinin pathway. KLK1 has good renal protection and hypotensive effect, and has good control effect on renal parenchymal hypertension [19,20]. Previous research found that serum kallistatin is increased in type 1 diabetes patients with vascular complications [21]. In addition, researchers found that serum kallistatin is decreased in pre-clampsia patients after diagnosis. Therefore, we speculate whether the circulating kallistatin has changed before pre-clampsia was confirmed, and could the variation can be used to predict preeclampsia before it actually occured.
In this study, we aimed to study the expression model of kallistatin in pre-clampsia patients before it diagnosed, explore the possibility of kallistatin being a promising early predictive biomarker, and try to find the relationship between kallistatin and other laboratory features.
Materials and Methods
This case-control study is part of a cohort study aimed to screen risking factors of PE in normal pregnancy. This cohort study included 800 patients admitted to the Gynecology and Obstetrics Clinic of Third Affiliated Hospital of Guangzhou Medical University (Intensive maternity treatment center in South China) between 2020 and 2022. Inclusion criteria: Pregnant women between 18 and 40 years old. Exclusion criteria: Women with a history of inflammatory diseases such as inflammatory bowel disease, vacuities and rheumatic diseases; complicated with acute or chronic infection; any fetal chromosome or developmental abnormality; Systematic diseases of pregnant women, such as known liver, kidney and adrenal diseases. The plasma samples were collected at two time-points, before 20 weeks of gestation and after 34 weeks. We select 11 cases diagnosed PE and 74 cases of randomized normal pregnancy as our experimental subjects. Kallistatin of the samples collected before 20 weeks was detected by ELISA (Human Serpin A4/Kallistatin, P257070, Bio-Techne R&D SYSTEMS, Shanghai, China) to explore its predictive value of PE.
Pre-eclampsia was diagnosed according to the Obstetrics and Gynecology Branch of Chinese Medical Association The Guidelines for the Diagnosis and Treatment of Hypertensive Disorders during Pregnancy (2020) [22]. After 20 weeks of pregnancy, systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg accompanied by any of the following: urinary protein ≥0.3 g/24 h, or urinary protein/ creatinine ratio ≥0.3, or random urinary protein ≥(+). There is no proteinuria but any of the following organs or systems is involved: abnormal changes in important organs such as heart, lung, liver and kidney or blood system, digestive system and nervous system, and placenta-fetus are involved [23].
The clinical characteristics and biochemical results of pregnant women were recorded. Blood parameters at about the same gestation weeks include white blood cell count, platelet count, hemoglobin (SYSMEX, XN-9000), AST, ALT, creatinine, uric acid, triglyceride, total cholesterol (Roche, c702) and plasma kallistatin. Pre-pregnancy BMI and blood pressure (after 20 weeks) were recorded.
Statistical analysis
The data are analyzed by IBM SPSS Statistics 20 statistical software, and the outliers are eliminated by box diagram. For continuous variables, the normality test should be carried out first. When the sample size is more than 50, Kolmogorov-Smirnov test should be used; Shapiro-Wilk test otherwise. Independent sample t-test is used to compare the differences between two groups if it conforms to the normal distribution and non-rank sum parameter test otherwise. The Receiver Operator Characteristic (ROC) curve was used to evaluate the diagnostic value of differential indicators for preeclampsia. Pearson correlation test or Speaman was utilized to evaluate possible correlation. The significance level was P<0.05.
Table 1: Demographic, clinical and laboratory data.
| variable | Control (n=74) | Preeclampsia (n=11) | P |
|---|---|---|---|
| Age (years) | 31.10 ± 4.16 | 31 ± 3.44 | 0.859 |
| Gestational age of blood collection (weeks) | 16.14 ± 1.63 | 15.64 ± 1.36 | 0.342 |
| Gestational week of labor (weeks) | 39.01 ± 1.32 | 37.90 ± 1.52 | <0.05 |
| BMI (kg/m2) | 21.90 ± 3.19 | 22.33 ± 4.76 | 0.708 |
| *Systolic blood pressure (mm/Hg) | 124.58 ± 13.51 | 153.64 ± 13.49 | <0.01 |
| *Diastolic blood pressure (mm/Hg) | 78.66 ± 10.69 | 93.82 ± 12.85 | <0.01 |
| WBC (×109/L) | 9.45 ± 1.83 | 10.14 ± 0.84 | <0.05 |
| PLT (×109/L) | 264.20 ± 42.76 | 261.60 ± 46.81 | 0.859 |
| AST (IU/L) | 16.65 ± 5.64 | 13.80 ± 3.33 | 0.098 |
| ALT (IU/L) | 14.28 ± 8.58 | 11.25 ± 4.25 | 0.264 |
| Creatinine (umol/L) | 48.00 ± 6.71 | 43.36 ± 4.13 | <0.05 |
| Uric acid (umol/L) | 243.33 ± 58.04 | 218.36 ± 47.43 | 0.181 |
| Hemoglobin (g/L) | 120.04 ± 8.63 | 124.45 ± 9.07 | 0.120 |
| Total cholesterol (mmol/L) | 5.01 ± 0.72 | 4.57 ± 0.56 | 0.062 |
| Triglycerides (mmol/L) | 1.58 ± 0.58 | 1.64 ± 0.42 | 0.749 |
| Kallistatin (ug/mL) | 6.32 ± 1.00 | 6.96 ± 0.80 | <0.05 |
Note: BMI: pre-pregnancy body mass index of pregnant women; WBC: white blood cell; PLT: platelets; AST: aspartate aminotransferase; ALT: alanine aminotransferase.*blood pressure were after 20 weeks.
Results
Table 1 presents the maternal demographic characteristics and delivery outcomes of both groups. The labor comes early (37.90 ± 1.52 vs 39.01 ± 1.32; P<0.05), the WBC was higher (10.14 ± 0.84 × 109 /L vs 9.45 ± 1.83 × 109 /L; P<0.05), and plasma kallistatin was higher (6.96 ± 0.80 vs. 6.32 ± 1.00 ug/mL, P<0.05) in preeclampsia women when compared with the control group, while there was no significant difference in maternal BMI, platelet count, uric acid, hemoglobin, triglyceride, total cholesterol, gestational age, AST, ALT and age between the two groups with gestational age matching.
ROC curve analysis of plasma kallistatin and other parameters in predicting pre-eclampsia
Based on ROC curve, the best cut-off value of plasma kallistatin for predicting preeclampsia is 6.64 ug/Ml (AUC=0.707, Youden index=0.456, 95%, CI: 0.547-0.867, P<0.05). When plasma kallistatin≥6.64 ug/ mL is used to predict preeclampsia, the sensitivity is 80% and the specificity is 65.6%.The best cutoff value of WBC in predicting preeclampsia is 9.31 × 109 /L (AUC=0.604, Youden index=0.384, 95% CI: 0.476-0.731, P<0.05). When predicting preeclampsia, the sensitivity is 90% and the specificity is 48.4%. The predictive value of Kallistatin is higher than WBC.
Although blood pressure is collected after 20 weeks, there was still something interesting. The best cutoff value of SBP in predicting preeclampsia is 135.5 mm/Hg (AUC=0.932, Youden index=0.728, 95% CI: 0.856-0.999, P<0.05), and the sensitivity and specificity in predicting preeclampsia are 90% and 82.8%, which is evidently better than DBP, of which the best cutoff value is 82.5 mm/Hg (AUC=0.805, Youden index =0.572, 95%, CI: 0.644-0.967, P<0.05), with the sensitivity is 90% and the specificity is 67.2%. In this case, SBP should be paied more attention than DBP in detecting pre-eclampsia. The results are shown in Figure 1.
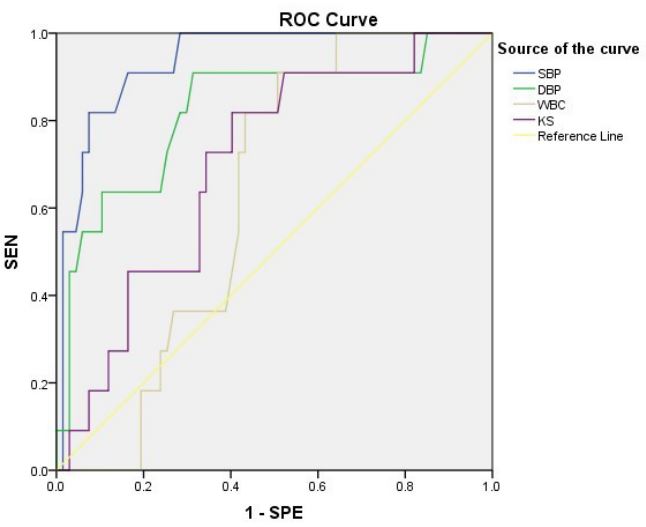
Figure 1: ROC curve of plasma kallistatin, WBC, systolic
blood pressure, and diastolic blood pressure used to predict pre-eclampsia.
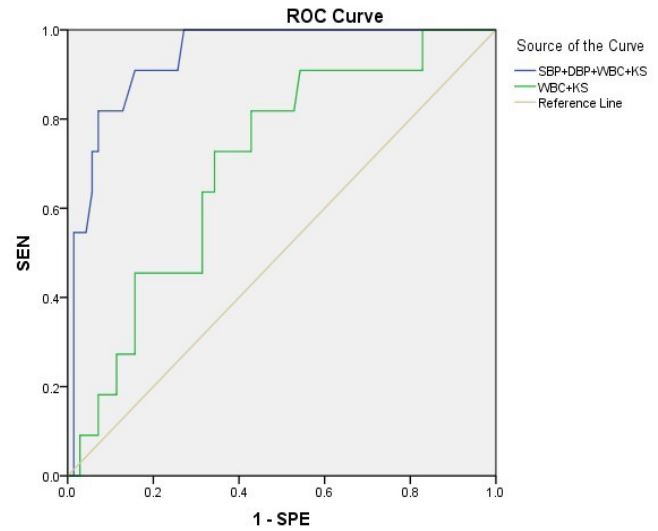
Figure 2: ROC curve of plasma Kallistatin combined with
WBC, SBP and DBP for predicting preeclampsia.
Table 2: Spearman correlation analysis of plasma Kallistatin and other experimental characteristics in patients with preeclampsia.
| PLT | AST | Total cholesterol | ||
|---|---|---|---|---|
| kallistatin | Correlation coefficient | -0.687 | 0.836 | 0.745 |
| N=11 | Sig.(bilateral) | 0.028 | 0.001 | 0.008 |
In pregnant women, plasma kallistatin is negatively correlated with creatinine and uric acid, and positively correlated with ALT. The results are shown in Tables 5.
Table 3: Pearson correlation analysis of plasma Kallistatin and other experimental charac- teristics.
| Creatinine | uric acid | ALT | ||
|---|---|---|---|---|
| kallistatin | Pearsoncorrelation | -0.247 | -0.242 | 0.029 |
| N=85 | significance (bilateral) | 0.029 | 0.036 | 0.044 |
ROC curve analysis showed that when plasma kallistatin, SBP, DBP and WBC are combined to predict preeclampsia, the sensitivity was 90.9% and the specificity was 84.3% (AUC=0.939, Youden index=0.752, 95%, CI: 0.881-0.997, P<0.05). Besides, when kallistatin and WBC are combined to predict preeclampsia, the sensitivity is 81.8% and the specificity is 57.1% (AUC=0.701, Youden index=0.390, 95%, CI: 0.550- 0.852, P< 0.05).The results are shown in Figure 2.
Correlation between plasma kallistatin and other experimental characteristics.
In patients with preeclampsia, plasma kallistatin is negatively correlated with PLT, and positively correlated with AST and total cholesterol. This revealed that increased kallistatin was possibly associated with more sever situation in pre-eclampsia patients, even the number is limited. The results are shown in Table 2.
Discussion
In this study, we selected 11 pre-eclampsia and 74 normal gestation women as our experimental subjects, retrospectively utilize their plasma samples collected before 20th week of pregnancy. Results showed that the plasma kallistatin level in patients with preeclampsia was significantly higher than that in normal pregnant women (6.96 ± 0.80 vs. 6.32 ± 1.00 ug/ml, P=0.047 <0.05), indicating that kallistatin had increased before PE was diagnosed. Furthermore, ROC analysis revealed that plasma kallistatin before 20 weeks can be a good predictor and biomarker of preeclampsia with the best cutoff value is 6.64 ug/mL and AUC=0.707. At the same time, factors combined could achieve a better diagnosis effectiveness with the best cut-off values of systolic blood pressure, diastolic blood pressure and WBC for predicting pre-eclampsia are 135.50 mmHg, 82.50 mmHg and 9.31 × 109 /L, respectively. ROC results show that the specificity and sensitivity of the combined diagnosis of the four factors were 84.3% and 90.9% (AUC=0.939, Youden index =0.752). Correlation analysis in patients with preeclampsia showed that plasma kallistatin was negatively correlated with PLT, and positively correlated with AST and Total Cholesterol (TC). Correlation analysis in pregnant women showed that plasma kallistatin was positively correlated with ALT, and negatively correlated with creatinine and uric acid. Therefore, we can conclude that kallistatin has a good correlation with liver function, PLT counts, and lipid metabolism, which is commonly involved organ damage indicators in severe pre-eclampsia, which can testifies kallistatin can be a good biomarker of pre-eclampsia.
The latest guidelines for the diagnosis and treatment of hypertensive disorders in pregnancy (2020) published by pregnancy-induced hypertension disease group, Obstetrics and Gynecology Branch of Chinese Medical Association emphasized that the form and degree of clinical manifestations are complex in gestational women with hypertension, the first symptoms of pre-eclampsia are also diverse. Therefore, it is challenging to identify early warning information and make early diagnosis. In recent years, the liberalization of the birth policy in China has increased the proportion of elderly pregnant women, it is necessary to found reliable predictors to alert the occurrence of pre-eclampsia at an early stage, so as to carry out early prevention and intervention, which is of great significance for reducing the incidence of pre-eclampsia and improving the pregnancy outcome of mother and baby. However, up to now, there are few protein markers for early diagnosis of preeclampsia. Researcher found that factors such as sFLt-1, PIGF, sEng may be useful to predict pre-eclampsia in the middle trimester [24,25], sFLt-1/PIGF has clinical value for short-term prediction of pre-eclampsia. Based on this paper, serum kallistatin has the potential to be a good predictor of pre-eclampsia before 20 weeks of gestation. Of course, more convencing conclusion needs more objects to verify.
Kallistatin is uniformly expressed in various tissues of human body, not only in the circulatory system, but also in urine, saliva, semen, amniotic fluid, milk, sweat and tears, among of which the content of kallistatin in human plasma is the highest [26]. Kallistatin has anti-inflammatory, anti-oxidative stress, anti-tumor, anti-angiogenesis, anti-fibrosis and anti-lymph angiogenesis and other biological functions [27-29]. It is closely related to many clinical diseases such as inflammatory bowel disease, hypertension, tumor, diabetes, cirrhosis, pancreatitis, coronary atherosclerosis, pulmonary inflammation, septic shock and so on. At the same time, kallistatin plays a dual role in angiogenesis, apoptosis and oxidative stress, maintaining the balance of our body. In normal pregnancy, normal vasodilation and contraction are indispensable, and NO plays an important role in vasodilation and contraction. Kallistatin can stimulate the expression and activation of endothelial Nitric Oxide Synthase (eNOS) in endothelial cells and Endothelial Progenitor Cells (EPCs) through active sites, which has a positive effect on the formation and relaxation of blood vessels [30,31]. Meanwhile, kallistatin can also inhibit angiogenesis and vascular permeability mediated by Vascular Endothelial Growth Factor (VEGF) through heparin-binding sites, thus playing an antagonistic role in angiogenesis [32,33]. If kallistatin is unbalanced in the dual role of angiogenesis, it will cause abnormal changes in blood pressure.
However, Güralp O [34] and others found that the serum kallistatin in patients with preeclampsia was lower than that in normal pregnant women with gestational age matching, and the serum kallistatin content in patients with early-onset preeclampsia (EOPE) was lower than that in patients with LateOnset Preeclampsia (LOPE). The difference between our study and theirs can be attributed to limited number, different race, different sampling time, and different detection method. Since researchers found that kallistatin can reduce blood pressure in hypertensive rats in the rat hindlimb ischemia model [35], we reasonable conjecture that the increased kallistatin is the body protecting response to imminent preeclampsia. In order to further study the value of plasma kallistatin in predicting preeclampsia, ROC analysis showed that the sensitivity and specificity of plasma kallistatin level in pre-eclampsia patients before 20 weeks of pregnancy for predicting preeclampsia were 80% and 65.6% (Youden index=0.456). Because we collected plasma samples before 20 weeks of pregnancy, it was detected that plasma kallistatin would increase long before the diagnosis of preeclampsia. Therefore, we can predict the occurrence of preeclampsia through the change of plasma kallistatin level. Because the renal function of the patients with preeclampsia in our study is normal, there is no correlation between kallistatin in PE and creatinine.
In this study, we found that kallistatin is increased in pre-eclampsia patients before 20 weeks of gestation when compared with healthy gestation age-matched pregnant women. Furthmore, the increased kalliatatin can be used to predict pre-eclampsia with cut-off value 6.64 ug/ml (AUC=0.707, Youden Index=0.456, 95%, CI: 0.547-0.867, P<0.05, Sensitivity=80%, Specificity=65.6%). In PE patients, plasma kallistatin was negatively correlated with PLT, and positively correlated with AST and Total Cholesterol (TC). In pregnant women, plasma kallistatin is positively correlated with ALT. The limitation of our study is that the number of cases with preeclampsia is small. Therefore, plasma kallistatin has certain clinical application value in predicting the occurrence and development of preeclampsia, and is a promising marker for predicting preeclampsia.
References
- Poon LC, Shennan A, Hyett JA, Kapur A, Hadar E, et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia: A pragmatic guide for first-trimester screening and prevention. Int J Gynaecol Obstet. 2019; 145: 1-33.
- Ives CW, Sinkey R, Rajapreyar I, Tita ATN, Oparil S. Preeclampsia-Pathophysiology and Clinical Presentations: JACC State-ofthe-Art Review. J Am Coll Cardiol. 2020; 76: 1690-1702.
- Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin Summary, Number 222. Obstet Gynecol. 2020; 135: 1492-1495.
- Staff AC, Benton SJ, von Dadelszen P, et al. Redefining preeclampsia using placenta-derived biomarkers. Hypertension. 2013; 61: 932-942.
- Chaiworapongsa T, Chaemsaithong P, Yeo L, Romero R. Pre-eclampsia. Part 1. Current understanding of its pathophysiology. Nat Rev Nephrol. 2014; 10: 466-480.
- Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin Summary, Number 222. Obstet Gynecol. 2020; 135: 1492-1495.
- Verlohren S, Galindo A, Schlembach D, et al. An automated method for the determination of the sFlt-1/PlGF ratio in the assessment of preeclampsia. Am J Obstet Gynecol. 2010; 202: e1, e11.
- Verlohren S, Herraiz I, Lapaire O, et al. The sFlt-1/PlGF ratio in different types of hypertensive pregnancy disorders and its prognostic potential in preeclamptic patients. Am J Obstet Gynecol. 2012; 206: e1-8.
- Villa PM, Hämäläinen E, Mäki A, et al. Vasoactive agents for the prediction of early- and late-onset preeclampsia in a high-risk cohort. BMC Pregnancy Childbirth. 2013; 13: 110-110.
- Rana S, Powe CE, Salahuddin S, et al. Angiogenic factors and the risk of adverse outcomes in women with suspected preeclampsia. Circulation. 2012; 125: 911-919.
- Zeisler H, Llurba E, Chantraine F, Vatish M, Staff AC, et al. Predictive Value of the sFlt-1: PlGF Ratio in Women with Suspected Preeclampsia. N Engl J Med. 2016; 374: 13-22.
- Kifle MM, Dahal P, Vatish M, Cerdeira AS, Ohuma EO. The prognostic utility of soluble fms-like tyrosine kinase-1 (sFlt-1) and placental growth factor (PIGF) biomarkers for predicting preeclampsia: A secondary analysis of data from the INSPIRE trial. BMC Pregnancy Childbirth. 2022; 22: 520.
- El-Asrar MA, Andrawes NG, Ismail EA, et al. Kallistatin as a marker of microvascular complications in children and adolescents with type 1 diabetes mellitus: Relation to carotid intima media thickness. Vasc Med. 2015; 20: 509-17.
- Chao J, Guo Y, Chao L. Protective Role of Endogenous Kallistatin in Vascular Injury and Senescence by Inhibiting Oxidative Stress and Inflammation. Oxid Med Cell Longev. 2018; 2018: 4138560.
- Chao J, Bledsoe G, Chao L. Protective Role of Kallistatin in Vascular and Organ Injury. Hypertension. 2016; 68: 533-41.
- Chao J, Li P, Chao L. Kallistatin: Double-edged role in angiogenesis, apoptosis and oxidative stress. Biol Chem. 2017; 398: 1309-1317.
- Alexander-Curtis M, Pauls R, Chao J, Volpi JJ, Bath PM, et al. Human tissue kallikrein in the treatment of acute ischemic stroke. Ther. Adv. Neurol. Disord. 2019; 12: 1756286418821918.
- Ma L, Wu J, Zheng Y, Shu Z, Wei Z, et al. Heparin Blocks the Inhibition of Tissue Kallikrein 1 by Kallistatin through Electrostatic Repulsion. Biomolecules. 2020; 10: 828.
- Chao J, Shen B, Gao L, Xia CF, Bledsoe G, et al. Tissue kallikrein in cardiovascular, cerebrovascular and renal diseases and skin wound healing. Biol Chem. 2010; 391: 345-55.
- Chao J, Bledsoe G, Chao L. Tissue kallikrein-kinin therapy in hypertension and organ damage. Prog Drug Res. 2014; 69: 37-57.
- Jenkins AJ, McBride JD, Januszewski AS, Karschimkus CS, Zhang B, et al. Increased serum kallistatin levels in type 1 diabetes patients with vascular complications. J Angiogenes Res. 2010; 2: 19.
- Lin JH, Lyu X. Difficulties and Confusion Concerning the Management of Hypertensive Disorders in Pregnancy--Interpretation of the Guidelines for the Diagnosis and Treatment of Hypertensive Disorders in Pregnancy (2020). Sichuan Da Xue Xue Bao Yi Xue Ban. 2022; 53: 1007-1011.
- Lambert G, Brichant JF, Hartstein G, Bonhomme V, Dewandre PY. Preeclampsia: An update. Acta Anaesthesiol Belg. 2014; 65: 137-49.
- Kaaja R. Predictors and risk factors of pre-eclampsia. Minerva Ginecol. 2008; 60: 421-9.
- Baumann MU, Bersinger NA, Surbek DV. Serum markers for predicting pre-eclampsia. Mol Aspects Med. 2007; 28: 227-44.
- Chao J, Schmaier A, Chen LM, et al. Kallistatin, a novel human tissue kallikrein inhibitor: levels in body fluids, blood cells, and tissues in health and disease. J Lab Clin Med. 1996; 127: 612-20.
- CR. Wang, SY Chen, CL Wu, et al. Prophylactic adenovirus-mediated human kallistatin gene therapy suppresses rat arthritis by inhibiting angiogenesis and inflammation 〔J〕. Arthritis Rheum. 2005; 52: 1319-1324.
- J Chao, H Yin, YY Yao, et al. Novel role of kallistatin in protection against myocardial ischemia-reperfusion injury by preventing apoptosis and inflammation 〔J〕. Hum Gene Ther. 2006; 17: 1201-1213.
- RQ Miao, J Agata, L Chao, et al. Kallistatin is a new inhibitor of angiogenesis and tumor growth〔J〕. Blood. 2002; 100: 3245-3252.
- Shen B, Gao L, Hsu YT, Bledsoe G, Hagiwara M, et al. Kallistatin attenuates endothelial apoptosis through inhibition of oxidative stress and activation of Akt-eNOS signaling. Am J Physiol Heart Circ Physiol. 2010; 299: H1419-27.
- Guo Y, Li P, Bledsoe G, Yang ZR, Chao L, et al. Kallistatin inhibits TGF-β- induced endothelial-mesenchymal transition by differential regulation of microRNA-21 and eNOS expression. Exp Cell Res. 2015; 337: 103-10.
- Miao RQ, Chen V, Chao L, Chao J. Structural elements of kallistatin required for inhibition of angiogenesis. Am J Physiol Cell Physiol. 2003; 284: C1604-13.
- Yin H, Gao L, Shen B, Chao L, Chao J. Kallistatin inhibits vascular inflammation by antagonizing tumor necrosis factor-α induced nuclear factor κB activation. Hypertension. 2010; 56: 260-7.
- Güralp O, Tüten N, Gök K, et al. Serum kallistatin level is decreased in women with preeclampsia. J Perinat Med. 2020; 49: 60-66.
- Chao J, Miao RQ, Chen V, et al. Novel roles of kallistatin, a specific tissue kallikrein inhibitor, in vascular remodeling. Biol Chem. 2001; 382: 15-21
