
Open Access, Volume 9
C.1241C>G mutation in NOTCH3: Evidence for pathogenicity in a family with CADASIL
A Dominguez-Mayoral1 ; P Menéndez-Valladares1 ; A Fuerte-Hortigón1*; S Pérez Sánchez1 ; F SánchezJiménez2 ; JJ Ríos-Martín3 ; M Alonso Riaño4 ; T Toledo-Pastrana5 ; T Benítez5 ; L Ferrandiz5 ; G Izquierdo1 ; E Tournier-Lasserve6 ; J Montaner-Villalonga1
1Stroke Unit, Virgen Macarena University Hospital, Seville, Spain.
2Department of Pathological Anatomy, Virgen Macarena University Hospital, Seville, Spain.
3Consultant, Department of Pathology, Virgen Macarena University Hospital, Sevilla, Spain.
4Department of Pathological Anatomy, 12th of October University Hospital, Madrid, Spain.
5Department of Dermatology, Virgen Macarena University Hospital, Seville, Spain.
6Department of Genetics, INSERM UMR 1161, Paris, France.
A Fuerte-Hortigón
Alejandro Fuerte Hortigón, C/José Laguillo 29, 3rd portal, 4ºA, Spain.
Tel: +34652524956;
Email: alfuerhorti@hotmail.com
Received : Aug 11, 2023,
Accepted : Sep 27, 2023
Published : Sep 29, 2023,
Archived : www.jclinmedcasereports.com
Abstract
This article discusses the diagnosis of CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy) in a Spanish family through clinical data, electron microscopy of skin biopsy, and genetic analysis of the NOTCH3 gene. Two mutations were identified in the family members through the next generation sequencing of the NOTCH3 gene: c.1241C>G and c.3421G>A. The first was previously reported and associated with CADASIL in the Korean population and classified as VUS. This study provides further scientific evidence to reclassify this variant from VUS to pathogenic. The other variant was classified as a variant of uncertain clinical significance. The importance of analyzing the functional combination of different variants in the same gene in families with patients displaying different phenotypes is highlighted.
Keywords: Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; NOTCH3; Novel mutation; Compound heterozygosis.
Copy right Statement:Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fuerte-Hortigón A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Dominguez-Mayoral A, Menéndez-Valladares P, Fuerte-Hortigón A, Pérez Sánchez S, Sánchez-Jiménez S, Ríos-Martín JJ, Alonso Riaño M, et al. C.1241C>G mutation in NOTCH3: Evidence for pathogenicity in a family with CADASIL. Open J Clin Med Case Rep. 2023; 2124.
Introduction
CADASIL is an abbreviation of Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (OMIM# 125310). It represents the paradigm of genetic cerebral microvascular diseases. The cardinal clinical feature is recurrent ischemic strokes since the early stages of life, vascular cognitive impairment, and migraine, at times with persistent aura. Associations with other diseases, such as antiphospholipid síndrome, have also been described, although rare [1]. CADASIL is suspected based on symptoms, family history, and brain MRI (Magnetic Resonance Image) lesions compatible with the disease, like ischemic lesions in the subcortical and deep white matter [2]. Microbleeds are also frequent, and their detection is vital, as their presence influences the decision on anticoagulation or acute reperfusion therapies [3].
Genetic studies are the gold standard for the diagnosis of the disease. At the molecular level, most genetic alterations are associated with NOTCH3, located on chromosome 19 [2]. The most frequent mutations are in the extracellular domain encoding part of the Epidermal Growth Receptor (EGFR), which involves different hypotheses related to a gain or a loss of function of Notch signalling [4]. In cases of variants of uncertain clinical significance (VUS), the diagnosis could be confirmed by identifying Granular Osmiophilic Material (GOM) inclusions on a skin biopsy [5].
The first patients of CADASIL from a Spanish family with Compound Heterozygous NOTCH3 Mutations (CHM) are reported in this study, whose analysis by electron microscopy of skin biopsies confirmed GOM deposits in the vessel walls of these patients. We provide further evidence to consider some mutations classified as VUS to be instead classified as pathogenic.
Case Presentation
Clinical data
Individual IV.1 (proband): This individual had a history of fully recovered internuclear ophthalmoplegia at 28. Multiple confluent supratentorial vascular lesions were found in the cerebral MRI. Skin biopsy with electron microscopy showed GOM inclusions. He was diagnosed with CADASIL.
Individual IV.2 (proband’s brother): This patient suffered a stroke at 42 and was treated with fibrinolysis without complications. In the following years, he experienced cognitive impairment and was diagnosed with CADASIL. Skin biopsy with electron microscopy findings was the same as patient IV.1.
Individual IV.3 (proband’s sister): The proband’s sister had a history of episodic migraine. She also had inherited coagulation disorders: Heterozygous G20210A mutation of the Prothrombin Gene (PG) and heterozygous C667T Mutation of the Tetrahydrofolate Reductase Gene (MTHFR). She suffered a stroke in her 30s, initially related to her inherited coagulation disorder, so anticoagulation was started. The skin biopsy with electron microscopy was not detected GOM.
Individual III.4 (proband’s mother): This patient had suffered recurrent ischemic strokes, the first in her twenties. At the age of 50, she developed a slowly progressive cognitive impairment. Among her family history, her father, now deceased, also had multiple strokes since his youth.
Individual III.3 (proband’s father): He had a history of hypertension and a similar inherited coagulation disorder as his daughter: Heterozygous G20210A (PG) and homozygous C667T (MTHFR). In addition, he was anticoagulated with Dabigatran due to Atrial Fibrillation (AF). He has suffered a transient ischemic attack and has been diagnosed with mild cognitive impairment with no neuroimaging findings compatible with CADASIL. There is no history of stroke or dementia in his family antecedents.
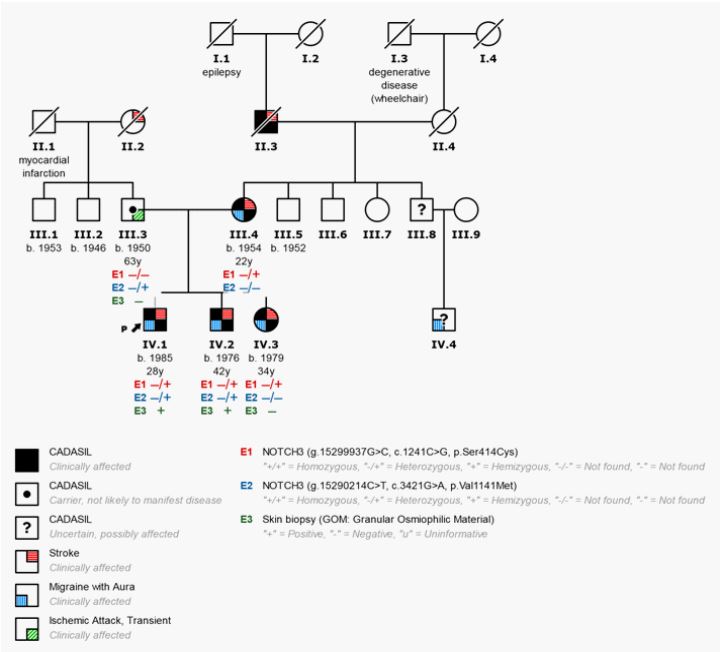
Figure 1: Pedigree of the family with CADASIL diagnosis. P: Proband. Four family members had symptoms
compatible with CADASIL (IV1/2/3 and III.4). Skin biopsy with electron microscopy revealed GOM inclusions
in two (IV.1/2). Next Generation Sequencing identified two mutations in the NOTCH3 gene: the heterozygous
missense c.1241C>G (p.Ser414Cys) and c.3421G>A (p.Val1141Met). c.1241C>G (p.Ser414Cys) was found in
all four symptomatic family members.
Genotypic data
By complete next generation sequencing of the NOTCH3 gene in the family members studied, the following findings were detected (Table 1):
The heterozygous missense c.1241C>G (p.Ser414Cys) mutation in exon 8 of NOTCH3, was detected in the proband, III.4, IV.2 and IV.3. This change has not been described before in the dbSNP database and its frequency in population databases is not registered (GenomAD frequency: 0.0). In silico analyses consider the change deleterious, as it alters a critical location within the protein and is expected to affect the function and cause disease. Although the lack of evidence initially suggested the consideration of VUS, it has just recently been reported in ClinVar as likely pathogenic.
The heterozygous c.3421G>A (p.Val1141Met) mutation in NOTCH3, was detected in the proband, III.3, and IV.2. This change has been described in the dbSNP database (rs373181668) and its frequency in population databases is relatively low (GenomeAD frequency: 0.00006), with no current evidence about its clinical implication. Most in silico prediction analyses for this variant consider it pathogenic (Polyphen2, SIFT, Mutation Taster) and benign in Provean. Based on the available information and the lack of current evidence, this change was considered VUS.
Table 1: Clinical information summary and genetic findings of family patients with CADASIL. Pb: Proband; HT: Hypertension; AF: Atrial Fibrillation; MRI: Magnetic Resonance Image; GOM: Granular Osmiophilic Material; ND: Not done; TIA: Transient Ischemic Attack; IS: Ischemic Stroke; MTHFR: Methylenetetrahydrofolate Reductase.
| III.3 | III.4 | IV.1Pb | IV.2 | IV.3 | ||
|---|---|---|---|---|---|---|
| Gender/Age (years) | ♂ 70 | ♀ 66 | ♂ 36 | ♂ 44 | ♀ 41 | |
| Risk factors | AF; HT; DM | HT | none | none | none | |
| Actual mRS | 1 | 4 | 0 | 4 | 0 | |
| MRI (CADASIL-like findings) | No | Yes | Yes | Yes | Yes | |
| Skin Biopsy | GOM - | ND | GOM + | GOM + | GOM - | |
| Thrombophilia | yes | no | yes | yes | yes | |
| Stroke | Yes [TIA] | Yes [Ischemic] | Yes [Ischemic] | Yes [Lacunar] | Yes [Ischemic] | |
| Other clinical characteristics | - |
Migraine with aura; cognitive decline |
Migraine | Migraine with aura | Migraine with aura | |
| Age at onset (years) | 63 | 22 | 28 | 42 | 34 | |
|
Genetic findings: mutation (Gene) |
C667T (MTHFR) | +/+ | -/- | +/+ | +/+ | +/+ |
| G20210A (Prothrombin) | -/+ | -/- | -/- | -/- | -/+ | |
| c.1241C>G, p.Ser414Cys (NOTCH3) | -/- | -/+ | -/+ | -/+ | -/+ | |
| c.3421G>A, p.Val1141Met (NOTCH3) | -/+ | -/- | -/+ | -/+ | -/- | |
Study subjects
A family in which all members have a history of stroke since youth is studied. The subjects were referenced according to the coordinates represented in the Pedigree (Figure 1). Written informed consent was obtained from all the family members reviewed. The study was approved by the Research Ethical Committee of the Hospital Universitario Virgen Macarena, Seville (S1900024).
Electron microscopy analysis of skin biopsies
A punch skin was available for patients III.3, IV.1, IV.2 and IV.3. Skin biopsy samples were fixed in glutaraldehyde and post-fixed in osmium tetroxide. After dehydration, tissue samples were embedded in Epon. Ultrathin sections were mounted on copper grids and stained with uranyl acetate and lead citrate as usual and examined with a transmission electron microscope.
Genetic analysis
NOTCH3 gene was sequenced by massive sequencing (NGS, Next-Generation Sequencing) in a NextSeq550 (Illumina), providing ~100% NOTCH3 gen coverage at a depth of >15x. Results were analysed by comparison with the reference sequence, and a search for the presence of mutations linked to the disease was carried out.
Discussion
The clinical features described for this family correlate with an autosomal dominant inheritance, which is characteristic of CADASIL disease. It is similarly expressed in both genders and shows a vertical pattern with at least one affected patient in each generation.
The variant which affects exon 8 of the NOTCH3 gene, c.1241C>G, was previously reported in the literature and associated with CADASIL in the Korean population [6]. However, it was classified as VUS. The variant c.1241C>G, which affects a cysteine in the typical EGF-like hotspot region in NOTCH3, could be reclassified according to new evidence as pathogenic (based on ACMG criteria [7]). This pathogenicity, which correlates with co-segregation data in the family studied, is also supported by the vast majority of in silico and bioinformatics prediction programs and the current evidence reported in ClinVar database. With maternal inheritance, this variant may be responsible for the ischemic events described in the proband, III.4, IV.2, and IV.3.
The stroke in IV.3 was attributed to heterozygous G20210A mutation of the Prothrombin Gene (PG) and heterozygous C667T Mutation of the Tetrahydrofolate Reductase Gene (MTHFR). However, given the low risk of arterial ischemic stroke posed by both conditions [8,9], the stroke is likely secondary to CADASIL. The fact that the skin biopsy of this patient does not show GOM is probably due to the low sensitivity of the technique, 45%, versus its high specificity (100%) [10].
The other variant (c.3421G>A), paternally inherited, was additionally found in IV.1 and IV.2, both patients with the most significant clinical involvement. As it is classified as VUS, there is still insufficient evidence at the genetic level for considering this variant as partially responsible for the phenotype of these patients or associated with the milder phenotype of patient III.3. The presence of GOM in such patients and not in their sister may be related to the fact of carrying the CHM.
CADASIL has been reported worldwide, but only some countries in Europe and East Asia have compiled large series of NOTCH3 mutations in CADASIL patients [11]. In the Caucasian population, the most frequently affected exons of NOTCH3 are 2-6 and 11 [12,13]. For this reason, genetic studies in most centres of our country were initially limited to these exons. However, screening all the NOTCH3 coding regions is beneficial for accurate CADASIL molecular diagnosis and a periodic reevaluation of VUS. The development of massive sequencing techniques has made it possible to extend the genetic study of these patients to the entire NOTCH3 gene in some centres, which has increased the diagnostic yield [14,15]. The expanded genetic test of the NOTCH3 gene allowed the CADASIL diagnosis and genetic counselling of this family. Although environmental factors cannot be excluded, these results highlight the importance of analysing the functional combination of different variants in the same gene, in families with patients displaying different phenotypes.
References
- Pantoni L, Sarti C, Pescini F, et al. Thrombophilic risk factors and unusual clinical features in three Italian CADASIL patients. Eur J Neurol. 2004; 11: 782-787.
- Chabriat H, Joutel A, Dichgans M, Tournier-Lasserve E, Bousser MG. Cadasil. Lancet Neurol. 2009; 8: 643-653.
- Tsai HH, Kim JS, Jouvent E, Gurol ME. Updates on Prevention of Hemorrhagic and Lacunar Strokes. J Stroke. 2018; 20: 167-179.
- Carare RO, Hawkes CA, Jeffrey M, Kalaria RN, Weller RO. Review: Cerebral amyloid angiopathy, prion angiopathy, CADASIL and the spectrum of protein elimination failure angiopathies (PEFA) in 4 neurodegenerative disease with a focus on therapy. Neuropathol Appl Neurobiol. 2013; 39: 593- 611.
- Tikka S, Mykkänen K, Ruchoux MM, et al. Congruence between NOTCH3 mutations and GOM in 131 CADASIL patients. Brain. 2009; 132: 933-939.
- Kim YE, Yoon CW, Seo SW, et al. Spectrum of NOTCH3 mutations in Korean patients with clinically suspicious cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Neurobiol Aging. 2014; 35: 726.e1-726.e7266.
- Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med. 2015; 17: 405-424.
- Moll S, Varga EA. Homocysteine and MTHFR Mutations. Circulation. 2015; 132: e6-e9.
- Varga EA, Moll S. Cardiology patient pages. Prothrombin 20210 mutation (factor II mutation). Circulation. 2004; 110: e15-e18.
- Markus HS, Martin RJ, Simpson MA, et al. Diagnostic strategies in CADASIL. Neurology. 2002; 59: 1134-1138.
- Maksemous N, Smith RA, Haupt LM, Griffiths LR. Targeted next-generation sequencing identifies novel NOTCH3 gene mutations in CADASIL diagnostics patients. Hum Genomics. 2016; 10: 38.
- Joutel A, Vahedi K, Corpechot C, et al. Strong clustering and stereotyped nature of Notch3 mutations in CADASIL patients. Lancet. 1997; 350: 1511-1515.
- Peters N, Opherk C, Bergmann T, Castro M, Herzog J, et al. Spectrum of mutations in biopsy-proven CADASIL: Implications for diagnostic strategies. Arch Neurol. 2005; 62: 1091- 1094.
- Muiño E, Gallego-Fabrega C, Cullell N, et al. Systematic Review of Cysteine-Sparing NOTCH3 Missense Mutations in Patients with Clinical Suspicion of CADASIL. Int J Mol Sci. 2017; 18: 1964.
- Dunn PJ, Maksemous N, Smith RA, Sutherland HG, Haupt LM, et al. Investigating diagnostic sequencing techniques for CADASIL diagnosis. Hum Genomics. 2020; 14: 2.
