
Open Access, Volume 9
Fetal extra-abdominal umbilical vein varix: Two cases of a rare malformation
Barbara Baur Cavegn*; Julia Popelka; Suekrue Arioglu; Monya Todesco Bernasconi
Women’s Department, Kantonsspital Aarau, Switzerland.
Barbara Baur Cavegn
Women’s Department, Kantonsspital Aarau, Switzerland.
Email: Barbara.baurcavegn@ksa.ch
Received : Aug 29, 2023,
Accepted : Sep 22, 2023
Published : Sep 29, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Fetal umbilical vein varix is a rare malformation of the umbilical cord. Most of the varices arise intraabdominally and there have been multiple studies about the diagnosis and management of fetal intra-abdominal umbilical vein varices. However fetal extra-abdominal umbilical vein varices are much rarer and up to date there are no clear criteria for the diagnosis or the clinical management of the condition. We saw two cases within a month in our ultrasound department in 2022 and had a favorable outcome in both pregnancies. In the first case the diagnosis was only established at 39 weeks of gestation, and we performed a cesarean section the next day. The second case was diagnosed at 31 weeks of gestation. The patient was admitted to hospital, and we administered Betamethasone for RDS prophylaxis. At 34 weeks of gestation there were fetal heartbeat abnormalities, and a cesarean section was performed. We also reviewed the literature of previous cases and our two cases included, so far only 19 cases of fetal extra-abdominal umbilical vein varix have been described.
Keywords: Umbilical cord; Diagnosis; Cases.
Copy right Statement:Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Baur Cavegn B (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Baur Cavegn B, Popelka J, Arioglu S, Todesco Bernasconi M. Fetal extra-abdominal umbilical vein varix: Two cases of a rare malformation. Open J Clin Med Case Rep. 2023; 2120.
Introduction
Fetal Umbilical Vein Varix (FUVV) is a rare malformation of the umbilical cord.
In most cases the varix is located intra abdominally arising between its entry into the abdomen and the portal system (fetal intra-abdominal umbilical vein varix FIUVV).
FIUVV accounts for approximately 4% of the malformation of the umbilical cord with an incidence of 0.4-1-1/1000 [1-4].
Fetal extra-abdominal umbilical vein varix (FEUVV) is much rarer and there are only few cases described in the literature.
The diameter of a normal umbilical vein increases during pregnancy from 2 mm at 15 weeks to about 7-8 mm at term [5-7]. Previous studies have proposed criteria for the diagnosis of FIUVV: umbilical vein diameter larger than 9mm and subhepatic umbilical vein diameter >50% of the intrahepatic umbilical vein diameter [1].
There are no such clear criteria for the diagnosis of FEUVV [8].
Fetal umbilical vein varix may have serious clinical consequences in the course of the pregnancy. Fetal Intrauterine Growth Restriction (IUGR) or even fetal death due to thrombosis of the umbilical vein have been previously described. Therefore, a detailed ultrasound to detect this anomaly is important. Close follow up of the varix is required and the option of a cesarean delivery to prevent dislodgment of the thrombus should be discussed with the patient.
We saw two cases of fetal extra-abdominal umbilical vein varix in our hospital in 2022. To our knowledge so far only 17 cases have been described in the literature [8-24].
Case Presentation
The first case is a 28-year-old gravida 3 para 2. She was first referred to our unit because of breech position of the baby at 38 1/7 weeks of gestation. Up until the she has received antenatal care and ultrasound examinations at a private practice nearby. She had a first trimester ultrasound but no combined screening for aneuploidies and the second trimester ultrasound with no observed anomalies was performed at 27 weeks of gestation.
On our first ultrasound examination we discovered the varix of the umbilical vein right at the placenta insertion site. The widest diameter was 22 mm (Figure 1).
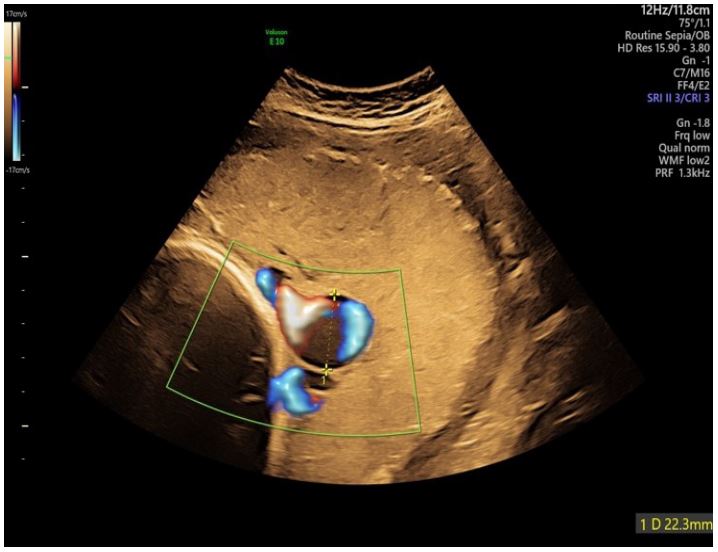
Figure 1: Transabdominal 2D ultrasound using color doppler (transverse view) at 39 weeks
showing a dilated umbilical vein on the surface of the placenta.
Apart from the extra-abdominal umbilical vein varix the female fetus was normally developed with an estimated weight of 2900 g (20th percentile), with a normal amount of amniotic fluid and physiological perfusion both in the umbilical artery and the Middle Cerebral Artery (MCA).
Due to the newly discovered varix of the umbilical vein, we didn’t perform an external cephalic version but scheduled a cesarean section for the next day because of the increased risk of intrauterine fetal demise [1,3,25].
We delivered a healthy female fetus with a weight of 3020 g (32nd percentile), APGAR 9/10/10 and an umbilical cord arterial pH of 7.29.
We sent the placenta to pathology and our diagnosis of an extra-abdominal umbilical vein varix with a diameter of up to 30 mm was confirmed (Figure 2). There were no signs of thrombosis.

Figure 2: Placenta with a dilated umbilical vein at the insertion of the umbilical cord.
The second case is a 33-year-old gravida 1. She was referred to our unit at 27 weeks of gestation due to a newly diagnosed growth restriction and reduced amniotic fluid. So far, she had received her prenatal care including ultrasound examinations at a private practice.
The pregnancy was conceived via in vitro fertilization. Due to a beta thalassemia minor of both parents a preimplantation diagnostic was performed, and the fetus also tested positive for beta thalassemia minor.
A combined first trimester screening showed a small risk for Trisomy 21,13 and 18 and the ultrasound at 22 weeks was normal as well.
On her first visit to our unit at 26 6/7 weeks of gestations we saw a female fetus with a severe early growth restriction (estimated fetal weight of 670 g, <3rd percentile) with no major anomalies. Amniotic fluid was at the lower end of the normal range. All long bones were shortened, furthermost femur and humerus. There were no signs of thoracic hypoplasia, no cardiomegaly or signs of heart failure. The fetal perfusion including Ductus Venosus (DV) was normal ant there were no signs of fetal anemia.
We interpreted these findings as an early placental insufficiency and recommended an amniocentesis. The couple declined the amniocentesis due to lacking consequences.
So, we scheduled weekly ultrasound checks with fetal hemodynamics and fetal biometry every two weeks. The fetus showed an accurate growth below the third percentile, amniotic fluid was stable at a low level and the perfusion in umbilical artery, MCA und DV remained normal.
At 30 3/7 weeks of gestation, we first discovered an extra-abdominal varix of the umbilical vein with a diameter of 16.5 mm (Figure 3).

Figure 3: Transabdominal 2D ultrasound (transverse view) showing a dilated umbilical vein
within the cord.
Due to the increased risk of intrauterine fetal demise in the presence of umbilical vein varix, combined with the growth restriction the patient was admitted to our hospital. She received RDS prophylaxis with Betamethasone 12 mg i.v. at 30 4/7 and 30 5/7 weeks of gestation, cardiotocography twice daily and doppler follow up every 2-3 days.
At 33 5/7 weeks of gestations cardiotocography showed signs of placental insufficiency with repeated decelerations so we decided to perform a cesarean section.
We delivered a female preterm fetus with a birthweight of 1365 g (<P3), APGAR of 8/10/10 and an umbilical cord arterial pH of 7.35.
She was immediately admitted to the NICU and needed CPAP support.
We sent the placenta to pathology and our diagnosis of an extra-abdominal umbilical vein varix was confirmed with no signs of a thrombus (Figure 4).
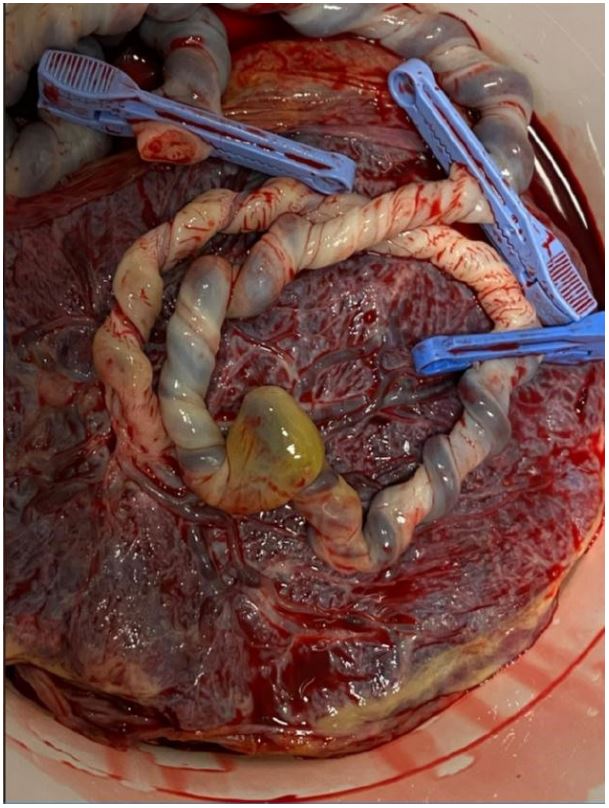
Figure 4: Placenta with a dilated umbilical vein in the central part of the cord.
Discussion
We saw two cases of an extremely rare condition within a month and had a favorable outcome in both cases.
The diagnosis of an extra-abdominal umbilical vein varix prenatally is often difficult and there is only very little data on the accurate method of surveillance and management [21].
We reviewed the literature of the so far published 17 cases of extra abdominal umbilical vein varix.
The diagnosis was established between 20 and 39 weeks of gestation, in 5 cases the diagnosis was only established postdelivery. In the majority of the cases a thrombosis of the varix was found. The Diameter of the varices ranged for 1 cm to 5 cm.
Fetal heartbeat abnormalities were often the reason for delivery and in 12 of the cases a cesarean section was performed.
In 4 of the cases there was fetal demise, either pre- or postnatal. Further information is collected in table 1 (modified from Io et al) [23].
Studies showed that fetal extra-abdominal umbilical vein varix increases the risk of intrauterine fetal demise, fetal heart failure, fetal anemia, hydrops fetalis, thrombosis, umbilical cord twisting with subsequent ulceration and blood loss [1,3,20,23-25].
There is also an increased risk of chromosomal abnormalities in the presence of intra-abdominal vein varix (Trisomy 21,18,) [5,25]. To our knowledge no chromosomal abnormality was detected in the presence of extra-abdominal umbilical vein varix.
Table 1: Clinical characteristics of 10 cases with extra umbilical vein varix (modified from Io et al).
| Case No |
Diagnosis (WG) |
Location of varix | Diameter (cm) |
Thrombosis |
Non-reassuring fetal status |
Delivery mode | Birth (WG) | Birth weight (g) |
APGAR Score 1/5 min |
Comment | Reference | Year of publication |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Postdelivery | 1 cm from Fetus | NA | + |
Decreased fetal movement |
VD | 37 | 2250 | NA |
Long cord Fetal death |
Ghosh et al [9] | 1984 |
| 2 | 34 | 10 cm from Fetus | 5 | + | FHB abnormalities |
CS | 36 | 2420 | 4/6 | Vesce et al [10] | 1987 | |
| 3 | postdelivery | 4 cm from placenta |
3 | + | Fetal death | - | 39 | 3130 | - | SUA |
Schrocksnadel et al [11] |
1991 |
| 4 | 32 |
2 cm from the fetus |
2 | (+) artery |
FHB abnormalities |
CS | 25 | 2041 | NA/8 |
White and Kofinas [12] |
1994 | |
| 5 | 24 | 8 cm from placenta |
4 | + | - | VD | 33 | NA | NA | VSD | Shipp et al [13] | 1995 |
| 6 | Postdelivery | 8 cm from fetus | 5 | + | - | VD | 41 | 3920 | 9/10 | Zachariah et al [14] | 2004 | |
| 7 | 31 | 3 cm from fetus | 3 | - | - | CS | Term | NA | NA | Akar et al [15] | 2012 | |
| 8 | 20 | 3 cm from fetus | 4 | + | FHB abnormalities |
CS | 35 | 1990 | 8/9 | SUA | Trobs et al [16] | 2012 |
| 9 | 35 | 10 cm from fetus | 2 | + | - | CS | 35 | 2501 | 8/9 | Kanenishi et al [17] | 2013 | |
| 10 | postdelivery | Midportion | NA | - | FHB abnormalities |
CS | 37 | 3050 | 4/8 | Soriano et al [18] | 2015 | |
| 11 | 24 | Midportion | 4 | + | Fetal death | - | 32 | NA | - |
Klippel-Trenaunay- Weber syndrome |
Cruise and Rouse [19] | 2016 |
| 12 | postdelivery | Midportion | 1.9 | + | Fetal death | VD | 38 | NA | - | Cord hematoma | Al-Maghrabi et al [20] | 2017 |
| 13 | 36 |
Attachementpoint of fetus |
5 | + | FHB abnormalities |
VD | 36 | 3647 | 8/9 | Cassidy-Vu et al [8] | 2019 | |
| 14 | 23 | Midportion | 3 | + | FHB abnormalities |
CS | 32 | 1744 | 8/9 | Matsumoto et al [21] | 2019 | |
| 15 | 39 | Fetal side | NA | - | FHB abnormalities |
CS | 39 | NA | NA | Hayden et al [22] | 2020 | |
| 16 | 27 | 5 cm | 1 | - | FHB abnormalities |
CS | 33 | 1334 | 4/7 | Neonatal Anemia | Io et al [23] | 2021 |
| 17 | 24 | On the placenta | 10.5 | + | FHB abnormalities |
CS | 24 | 610 | 4/5 |
Fetal Anemia, neonatal death |
Jackson et al [24] | 2021 |
| 18 | 39 | On the placenta | 3.3 | - | - | CS | 39 | 3020 | 9/10 | This study | 2022 | |
| 19 | 31 | Midportion | 1.6 | - | FHB abnormalities |
CS | 34 | 1365 | 8/10 | This study | 2022 |
If an umbilical vein varix is detected fetal echocardiogram should be performed to exclude cardiac malformations und a close surveillance of the pregnancy is recommended [21].
If fetal anemia is suspected a diagnostic cordocentesis can be offered to evaluate the need for fetal transfusion [23,24].
There are no clear recommendations of how to monitor a pregnancy with diagnosed fetal extraabdominal umbilical vein varix. Expert opinions suggest weekly ultrasound prior to 28 weeks of gestation and bi-weekly examinations thereafter until delivery to evaluate for the presence of thrombosis in the umbilical vein varix [7].
The dislodgment of a thrombus is a great risk for the fetus and might be responsible for fetal loss [11,14,16,199,21].
Time of delivery should be planned individually but it seems appropriate to induce between 36 and 37 weeks gestation. In case of present thrombus in the varix a vaginal delivery increases the risk of thrombus dislodgement, and a cesarean section should be offered.
Declarations
Data availability: Data supporting this case report are available from the corresponding author on reasonable request.
Consent: Written informed consent was obtained from the patients for the publication of this case report.
Disclosure of interest: The authors declare that they have no conflicts of interest.
References
- Beraud E, Rozel C, Milon J, Darnault P. Umbilical vein varix: Importance of ante- and post-natal monitoring by ultrasound. Diagn Interv Imaging. 2015; 96: 21-6.
- Konstantinova B. Malformations of the umbilical cord. Acta Genet Med Gemellol (Roma). 1977; 26: 259-66.
- Byers BD, Goharkhay N, Mateus J, Ward KK, Munn MB, et al. Pregnancy outcome after ultrasound diagnosis of fetal intraabdominal umbilical vein varix. Ultrasound Obstet Gynecol. 2009; 33: 282-6.
- Mankuta D, Nadjari M, Pomp G. Isolated fetal intra-abdominal umbilical vein varix: clinical importance and recommendations. J Ultrasound Med. 2011; 30: 273-6.
- Mahony BS, McGahan JP, Nyberg DA, Reisner DP. Varix of the fetal intra-abdominal umbilical vein: Comparison with normal. J Ultrasound Med. 1992; 11: 73-6.
- Weissman A, Jakobi P, Bronshtein M, Goldstein I. Sonographic measurements of the umbilical cord and vessels during normal pregnancies. J Ultrasound Med. 1994; 13: 11-4.
- Weissmann-Brenner A, Simchen MJ, Moran O, Kassif E, Achiron R, et al. Isolated fetal umbilical vein varix--prenatal sonographic diagnosis and suggested management. Prenat Diagn. 2009; 29: 229-33.
- Cassidy-Vu L, Clark S, Cuka N. Extra-abdominal umbilical vein varix in a newborn. BMJ Case Rep. 2019; 12.
- Ghosh A, Woo JS, MacHenry C, Wan CW, O’Hoy KM, et al. Fetal loss from umbilical cord abnormalities--a difficult case for prevention. Eur J Obstet Gynecol Reprod Biol. 1984; 18: 183-98.
- Vesce F, Guerrini P, Perri G, Cavazzini L, Simonetti V. Ultrasonographic diagnosis of ectasia of the umbilical vein. J Clin Ultrasound. 1987; 15: 346-9.
- Schrocksnadel H, Holbock E, Mitterschiffthaler G, Totsch M, Dapunt O. Thrombotic occlusion of an umbilical vein varix causing fetal death. Arch Gynecol Obstet. 1991; 248: 213-5.
- White SP, Kofinas A. Prenatal diagnosis and management of umbilical vein varix of the intra-amniotic portion of the umbilical vein. J Ultrasound Med. 1994; 13: 992-4.
- Shipp TD, Bromley B, Benacerraf BR. Sonographically detected abnormalities of the umbilical cord. Int J Gynaecol Obstet. 1995; 48: 179-85.
- Zachariah M, Vyjayanthi S, Bell-Thomas S. Umbilical vein varix thrombosis: a rare pathology. J Obstet Gynaecol. 2004; 24: 581.
- Akar M, Dilli D, Sandal G, Oncel MY, Erdeve O, et al. Prenatally diagnosed umbilical vein aneurysm with good prognosis. J Clin Ultrasound. 2012; 40: 368-9.
- Trobs RB, Teig N, Neid M, Gernaianu G, Kozlowski P. Pseudotumerous enlargement of the umbilical cord owing to an intraamniotic varicosity associated with thrombocytopenia. J Pediatr Surg. 2012; 47: 1760-2.
- Kanenishi K, Nitta E, Mashima M, et al. HDlive imaging of intra-amniotic umbilical vein varix with thrombosis. Placenta. 2013; 34: 1110-2.
- Soriano-Lillo P, Padilla VC, Blazquez RA, Crespo V. Extra-abdominal umbilical vein varix. A case report. Ginecol Obstet Mex. 2015; 83: 356-62.
- Cruise KRL, Rouse G. Klippel-Trenaunay-Weber Syndrome Complicated by Extrafetal Umbilical Vein Varix. Journal of Diagnostic Medical Sonography. 2016; 18: 317-320.
- Al-Maghrabi HA, Contreras LHC, Martinez S. Extra abdominal Umbilical Vein Varix Causing Stillbirth: a Case Report. Annals of Pathology and Laboratory Medicine. 2017; 4: C94-C97.
- Matsumoto Y, Yanai A, Kamei S, Yamaguchi A, Nakamine H, et al. A Case Report of Umbilical Vein Varix with Thrombosis: Prenatal Ultrasonographic Diagnosis and Management. Case Rep Obstet Gynecol. 2019; 2019: 7154560.
- Hayden J, Boyle MA. Images in paediatrics: Intra-amniotic umbilical vein varix. Arch Dis Child. 2020; 105: 190.
- Io S, Kondoh E, Iemura Y, et al. Severe fetal anemia as a consequence of extra-abdominal umbilical vein varix: A case report and review of the literature. Congenit Anom (Kyoto). 2021; 61: 4-8.
- Jackson J, Castro E, Belfort MA, Shamsirshaz AA, Nassr AA, et al. Massive Extra-Abdominal Umbilical Vein Varix: A Case Report. Fetal Diagn Ther. 2021; 48: 158-162.
- Fung TY, Leung TN, Leung TY, Lau TK. Fetal intra-abdominal umbilical vein varix: What is the clinical significance? Ultrasound Obstet Gynecol. 2005; 25: 149-54.
