
Open Access, Volume 9
Association between iron deficiency anaemia and ischaemic stroke: A systematic review
Preethy Manoj1,2; Rosemarie Derwin1; Pinar Avsar1; Eamon Dolan1,2; Zena Moore1,3,4,5,6,7; Declan Patton1,9,10; Tom O’Connor1,8,9; Linda Nugent1; Sherly George1
1School of Nursing and Midwifery ,Royal College of Surgeons in Ireland, St Stephens Green, St Peters, Dublin 2, Ireland.
2Connolly Hospital, Blanchardstown, Dublin 15, Ireland.
3Adjunct Professor, School of Nursing & Midwifery, Griffith University, Queensland, Australia.
4Visiting Professor, School of Health Sciences, Faculty of Life and Health Sciences Ulster University, Northern Ireland.
5Honorary Visiting Professor, Cardiff University, Cardiff, Wales.
6Adjunct Professor, Department of Nursing, Fakeeh College for Medical Sciences, Jeddah, KSA.
7Professor, Department of Public Health, Faculty of Medicine and Health Sciences, Ghent University, Belgium.
8Honorary Professor, Lida Institute, Shanghai, China.
9Adjunct Associate Professor, Fakeeh College of Health Sciences, Jeddah, Saudi Arabia.
10Honorary Senior Fellow, Faculty of Science, Medicine and Health, University of Wollongong, Australia.
Preethy Manoj
School of Nursing and Midwifery, Royal College of Surgeons in Ireland, St Stephens Green, St Peters, Dublin 2, Ireland.
Email: preethymanoj@rcsi.ie
Received : July 31, 2023,
Accepted : Sep 20, 2023
Published : Sep 22, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Stroke is a leading cause of disability and death in adults. Hypertension, diabetes mellitus, hyperlipidaemia and atherosclerosis are reported to be the most common causes for stroke. The World Health Organisation has reported that the most common nutritional deficiency in the world is iron deficiency anaemia [IDA] affecting 30% of the world’s population. However, very little is known about the association between IDA and stroke in adults. This systematic review aims to evaluate the association between IDA and ischemic stroke in adults.
Methods: The Preferred Reporting Items for Systematic Review and Meta-Analyses [PRISMA] was used to guide the review. The main databases such as CINAHL, PUBMED, MEDLINE, COCHRANE, HSE online library, and Wiley Online library were searched. Twelve relevant articles including one case presentation, one case control study, and ten case reports were included in the review. Quality Appraisal was undertaken using the JBI [Joanna Briggs Institute] critical appraisal checklist. Following data extraction, a narrative analysis of the results was completed.
Results: Total 107 participants were included in this review [females n = 58, males n = 49]. Patients in the included studies, were diagnosed with ischaemic stroke. They had low haemoglobin level. Their stroke symptoms improved with iron treatment and transfusions. From this review it appears that an association exists between IDA and ischaemic stroke. Menorrhagia was identified as the main cause of IDA in females. Among men, IDA was associated with rectal bleeding.
Conclusion: Considering this review, IDA should be considered as a possible risk factor for stroke. However, more primary research studies are necessary to authenticate this finding.
Keywords: Iron deficiency anaemia; IDA; Ischaemic stroke; Cerebral infarction.
Abbreviations: WSO: World Stroke Organisation; IDA: Iron Deficiency Anaemia; TIA: Transient Ischaemic Attack; SR: Systematic Review; PRISMA: Preferred Reporting Items for Systematic Review and Meta Analyses; HSE: Health Service Executive; JBI: Joanna Briggs Institute; ED: Emergency Department; Hb: Haemoglobin; TIBC: Total iron binding capacity; MRI: Magnetic Resonance Imaging; NIHSS: National Institutes of Health Stroke Scale; CINAHL: Cumulated Index to Nursing and Allied Health Literature; MCV: Mean Corpuscular Volume; MCH: Mean Corpuscular Haemoglobin; MCA: Middle Cerebral Artery; MRC: Medical Research Council; CT Scan: Computed Tomography Scan; TEE: Trans Oesophageal Echo; PAG: Periaqueductal Gray; pRBC: Packed Red Blood Cells; DM: Diabetes Mellitus; ASTRAL: Acute Stroke Registry and Analysis of Lausanne; MRC: Medical Research Council.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Manoj P (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Manoj P, Derwin R, Dolan E, Moore Z, Patton D, O’Connor T, Nugent L, et al. Association between iron deficiency anaemia and ischaemic stroke: A Systematic Review. Open J Clin Med Case Rep. 2023; 2118
Introduction and background
The term “apoplexy” was used in the ancient Greco-Roman era to describe a condition in which the patient “suddenly falls with abrupt abolition of all activities of the mind while retaining pulse and respiration “ [1]. The term “stroke” to symbolize apoplexy was first used by Mr. William Cole in 1689 [1]. According to World Stroke Organisation [WSO], Global stroke fact sheet 2022, there are over 12.2 million new strokes each year [2]. Globally, one in four people over 25 years of age will have a stroke in their lifetime [2]. Stroke is the second most important cause of death worldwide and a prominent cause of disability [3]. Two million brain cells die every minute in stroke increasing the risk of permanent brain damage, disability, or death [4]. Stroke is usually caused by hypertension and atherosclerosis [5]. In one-third of all ischemic strokes the cause will be cryptogenic [6].
Anaemia accounts for 8.8% of the total global health burden [7]. World Health Organisation [WHO] reports anaemia as the most common nutritional deficiency in the world affecting 30% of the population [8]. Almost 50% of the anaemia worldwide is due to iron deficiency [9]. The association between iron deficiency anaemia [IDA] and stroke was first reported by Alexander in 1983 [10]. But earlier in 1970 one study [11] reported an association between neurological symptoms and low haemoglobin. Dubyk et.al 2012 [12], explored the association between IDA and ischemic stroke in patients ≥65 years of age diagnosed with their first ischemic stroke or Transient Ischaemic Attack [TIA]. The overall prevalence of IDA associated ischemic stroke/TIA was 6.4% in the sample group. Similarly, the association between IDA and stroke based on the secondary data from the Taiwanese Longitudinal Health Insurance Database was reported in 2013 [13]. Anaemia may worsen regional hypoxia in the areas of decreased cerebral perfusion [so called “anaemic infarction”] [14]. An Asian study undertaken in Pakistan reported a significant association between anaemia and severity of stroke [15]. There are numerous studies that have reported a correlation between low haemoglobin and neurological symptoms [5,16,17,18,19]. Patients with anaemia have increased mortality with stroke [20] and there is significant association of anaemia and cerebral venous thrombosis [21].
The above case reports draw attention to the increasing indication for a potential link between severe IDA and ischemic stroke. No systematic review [SR] has been completed on this topic. The impact of anaemia on stroke patients is unreasonably underestimated [22]. This SR aims to explore the complex relationship between IDA and ischemic stroke.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA] [23] guidelines were followed in this review.
Aims and objectives: This SR aims to explore the link between IDA and ischemic stroke in adults.
SR question: What is the impact of IDA on the clinical presentation and treatment outcome of patients with ischaemic stroke?
Search strategy: Between November 2020 and April 2023, a systematic literature search was undertaken to ensure that all the articles that met the inclusion criteria were incorporated in the review. The last search was carried out on 14th April 2023. The key search terms used were, iron deficiency anaemia, IDA, and ischaemic stroke. The main databases such as CINAHL, PUBMED, MEDLINE, COCHRANE, HSE online library, and Wiley Online library were used for the literature search.
Inclusion criteria: In this review, the target population is men and women ≥18 years with confirmed diagnosis of ischaemic stroke. All published trials, observational studies, case reports, cohort studies, case presentations, case control studies mentioning IDA and ischaemic stroke in at least one patient are included in this review. Only English language studies are included in this SR.
Exclusion criteria: Patients <18 years, patients diagnosed with other stroke types like haemorrhagic stroke, consensus statements and foreign language studies were excluded from this SR.
Primary outcome
Serum haemoglobin/iron level.
Secondary outcomes
• Clinical presentation and treatment outcomes.
• Predictors of IDA.
Data extraction: The available data was extracted from the included studies under the following headings using a data extraction table: Author and year, demographics and country, method of stroke diagnosis, type of study, haemoglobin level on admission, reason for IDA, diagnosis, treatment given and the outcome. The extracted data was reviewed and validated by the co-authors. Any disagreement in data extraction was resolved through discussions. Characteristics of the included studies is given in table 1.
Data synthesis: Most of studies included in this SR were case reports. Meta-analysis was not deemed suitable for this SR because of the wide-ranging variability of the studies in relation to their study design, study population, type of intervention and measured outcome. A narrative synthesis was carried out to synthesize the findings of the various studies. Firstly, a preliminary synthesis was carried out in the form of thematic analysis. Then the results were structured into themes. Finally, the included studies were summarised in a narrative synthesis within a structured framework. The framework consisted of the geographical location, demographics, serum haemoglobin level of the participants in the included studies, predictors of IDA, clinical presentation of the patients, method of stroke diagnosis, the treatment they received and the outcome.
Quality appraisal: Quality appraisal of the included studies were carried out using the JBI [Joanna Briggs Institute] critical appraisal checklists [24] (Supplementary Table 1). JBI critical appraisal tools has been peer reviewed approved by the JBI Scientific Committee [24]. The quality of the included studies was verified by two authors.
Results
Search results
A total of 70 articles were identified through database searches. The reference lists of the retrieved articles were scrutinized to find more studies. The initial screening was carried out based on the title and abstract of the retrieved articles. After removing duplicates [n = 18] and irrelevant studies [n = 10], 42 articles were screened for eligibility. Out of 42 articles, 22 articles were selected for full screening. Out of the 22 full text articles, 10 were excluded as they did not meet the inclusion criteria. The excluded articles with reasons are included in Table 4.
The full texts of the remaining studies were read in detail and assessed for suitability. Twelve articles that met the predefined inclusion were included in the review. One case presentation [16], ten case reports [5,6,9,15,25-30], and one case control study [12] were included in this SR. The PRISMA flowchart outlines the study selection process (Figure 1).
Description of the included studies
Geographical location: Nine case reports [5,6,9,15,25-30] and one case control study [12] were conducted in USA. Two cases were reported from Japan [17,28].
Demographic characteristics: A total of 107 participants were included in this review [Dubyk et al. [2011] n = 94, Yakushiji et al. [2005] n = 2, Naito et al. [2014] n = 2 and rest of the included studies had one participant each] of which 58 were females representing 54.2% of the total participants. Male participants accounted for 45.75% of the study population [n = 49]. All participants were over 20 years of age. Demographic characteristics of the participants are included in Table 2.
Primary outcomes
Serum haemoglobin/ Iron level: The World Health Organization [32] defines anaemia as blood haemoglobin values of less than 7.7 mmol/l [13 g/dl] in men and 7.4 mmol/l [12 g/dl] in women. IDA is characterized by microcytic, hypochromic erythrocytes and low iron and ferritin with an elevation of total iron binding capacity [16]. Iron studies diagnostic for IDA consist of a low haemoglobin [<7.7 mmol/l in men and 7.4 mmol/l in women], a low serum iron [<7.1 µg/l], a low serum ferritin [storage form of iron] [<30 ng/l], a low transferrin saturation [<15%], and a high total iron-binding capacity [>13.1 µmol/l] [33].
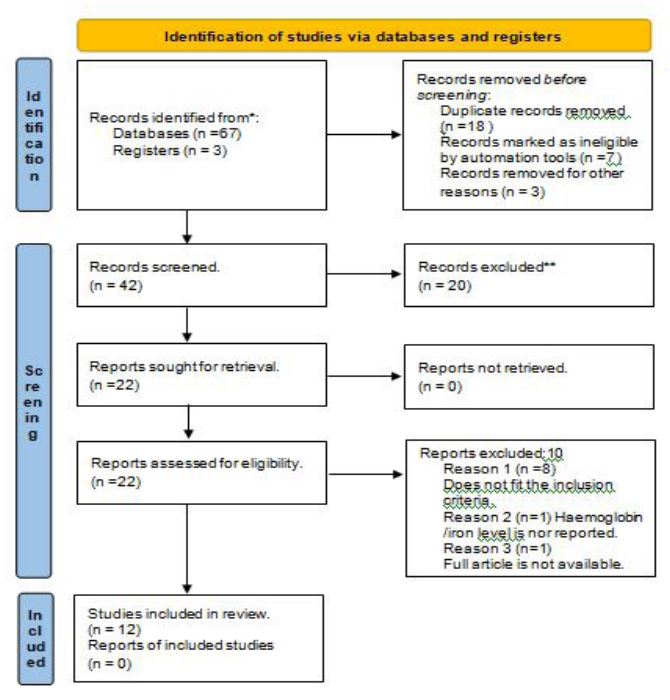
Figure 1: PRISMA 2009 Flow Diagram (OVERALL SEARCH)
Eleven of the included studies did give the haemoglobin/iron level of the patients on admission. [5,6,9,16,17,25-30]. In four studies [5,6,25,27], the peripheral blood smear displayed severely microcytic and hypochromic red blood cells indicative of IDA. Dubyk et al. [2012] [12] reported the mean value of the iron/haemoglobin level of the patients in their study. In all the included studies patients presented with low haemoglobin level. The serum haemoglobin and iron levels in the included studies is shown in table 3.
Secondary Outcomes
Clinical presentation and treatment outcome: Kandinata et al. [2021] [30] presented the case of a 34-year-old female who presented to the emergency department [ED] with difficulty in speaking and right arm weakness. Her initial physical examination revealed right facial droop. Laboratory analysis identified haemoglobin [Hb] of 9.1 g/dL, and haematocrit of 31.3%. Anaemia studies showed iron of 10 ug/dL, ferritin of 3.2 ng/mL, 3% iron saturation, and total iron-binding capacity [TIBC] of 338 ug/dL. Magnetic resonance imaging [MRI] of the brain revealed acute ischaemic stroke. On further history, it was identified that she has been having issues with menorrhagia. The patient’s haemoglobin continued to drop from 9.1 g/dL on admission to 8.6 g/dL and then to 8.3 g/dL. She received multiple doses of intravenous iron infusion during her stay in the hospital, and her condition improved gradually. This study concluded that the stroke was caused due to IDA secondary to menorrhagia as she was undergoing menstruation at the time of presentation and no other causes were identified.
Zhang et al. (2020) [16] described the case of a 29-year-old lady who presented with left sided numbness, National Institutes of Health Stroke Scale [NIHSS ] Score of 2 , Hb of 7.2 gm/dl and ferritin level of <1 ng/ml. MRI of the brain revealed acute left occipital lobe infarction. Her past medical history was significant for IDA associated with menorrhagia. Hb improved to 12.0 g/dl after receiving two units of packed red blood cell transfusions and a five-day course of iron transfusions. She was discharged with no residual neurological deficits. Her stroke was most likely secondary to IDA as her cardiovascular risk factors were low and her stroke work up was negative.
Similarly, in another study, Awad et al. [2020] [6], reported the case of a 42-year-old-lady who presented to the ED following an unwitnessed fall. On examination, her NIHSS score was 13 with left hemi sensory loss, left upper and lower extremity drift, aphasia, left facial palsy, GCS 14/15, with altered mental status, bilateral rightward eye deviation, Hb level of 7.7 gm/dl, ferritin level of 7 ng/ml and blood pressure of 200/113 mmHg. MRI of the brain revealed infarct of her middle cerebral artery and anterior cerebral artery territories. She had history of menorrhagia. Although her blood pressure was elevated on admission, it was controlled with intravenous bolus of labetalol and intravenous nicardipine infusion. All her subsequent blood pressure readings during hospitalisation were within normal range and she didn’t require any blood pressure lowering therapy. Her symptoms improved with oral doses of 325 mg of ferrous sulphate every other day and the patient was discharged home on oral anticoagulant and iron supplements. Six months later her haemoglobin normalized to 13.2 gm/dl and the iron therapy was discontinued. Her stroke was likely secondary to IDA.
Nisar and Hanumanthu [2019] [26] acknowledged the case of a 48-year-old lady with history of menorrhagia, Hb of 6.0 g/dl and ferritin level of 4 ng/dl, who presented to the ED with complaint of transient weakness and numbness in her left arm and leg lasting only two minutes. MRI of the brain showed acute infarctions in the right frontal lobe and left cerebellar hemisphere. This patient received one unit of packed red blood cells and was commenced on anticoagulation. Repeat MRI brain four days later did not show any new strokes, and the patient’s neurological examination remained stable. No clinical events were reported in the eight months follow up, patient remained on warfarin and iron repletion.
In another case report Gopalratnam et al. [2017] [9] presented the case of a 20-year-old female with Hb of 5.8 mg/dl and ferritin level of 39ng/dl, presented to the hospital following a motor vehicle accident. History revealed severe IDA associated with menorrhagia. On arrival to the hospital, she reported chest pain, dizziness, blurred vision, photophobia, and weakness to her left arm and leg. Her neurological findings revealed worsening left upper extremity strength, bilateral dysmetria and a positive Romberg sign. MRI of the brain revealed bilateral cerebellar and left occipital lobe non haemorrhagic infarcts. Her neurological function improved over a period of two weeks after multiple blood transfusions, intravenous iron infusion and ferrous sulfate 325 mg three times daily. In this case report, the author highlights the possibility that the stroke in this young patient was caused by severe IDA.
Naito et al. [2014] [17] described the case of a 42-year-old woman who experienced a half hour episode of right upper and lower extremity weakness, numbness and aphasia which had occurred soon after the end of her menstrual period. Her MRI Brain revealed subacute cerebral infarction. She had no significant past medical history other than two-year history of menorrhagia. Laboratory testing showed a remarkable decrease in haemoglobin concentration [9.1 mg/dL], high platelet count [48.0 × 104 /μL], low serum iron concentration [14 μg/dL], high unsaturated iron-binding capacity [400 μg/dL], low serum ferritin level [3.6 ng/mL], and a high transferrin saturation [329.0 mg/dL]. Based on these findings, she was diagnosed with IDA. In this case, her IDA was due to bleeding from uterine fibroid , and it was removed surgically. Patient’s anaemia improved after surgery and there was no recurrence of ischemic stroke.
In the same study Naito et al [2014] [17] portrayed the case of another 42- year -old woman with low haemoglobin concentration of 5.3 g/dl who presented with left facial and left upper extremity weakness. Her neurological examination revealed mild dysarthria and left central facial weakness. She had three-year history of menorrhagia and one year history of IDA. Brain MRI showed an acute infarction in the right cerebellar hemisphere, right frontal lobe and left frontal lobe. Based on the laboratory findings such as low haemoglobin level [5.3 gm/dl], low haematocrit [20.4%], low MCV [59.5 fL], low mean corpuscular haemoglobin [MCH] [15.5 pg/cell], low serum iron concentration [11 μg/dL], high unsaturated iron-binding capacity [359 μg/dL], and low serum ferritin level [4.0 ng/mL], she was diagnosed with IDA. In this case, patient refused blood transfusion and received intravenous iron therapy. Her anaemia and neurological functions improved, and no recurrence of stroke was reported. The two cases of ischaemic stroke reported by Naito et al. [2014] [17] among middle aged women were considered to be caused by IDA secondary to bleeding uterine fibroid.
The case of a 47-year-old lady with hypoxia induced stroke secondary to IDA associated with menorrhagia was reported by Mehta et al. [2012] [5]. Her menorrhagia was due to uterine fibroid. Patient presented with mild dysarthria and decreased repetitive finger movements in her left upper extremity. Laboratory investigations showed Hb of 7.6 gm/dl, haematocrit 23%, ferritin 4.6 ng/ml, all below normal levels. MRI of the brain revealed acute infarction in right middle cerebral artery [MCA] distribution. During the hospital stay, the patient had an unresponsive episode, with bowel incontinence, eyes deviated to the right side, left face weakness, and left upper extremity with 0/5 on MRC [Medical Research Council] scale for motor strength. She slowly became responsive over time. Her Hb at the time of this incident was 6.9 gm/dl. A repeat CT scan of the head showed a larger right MCA infarction compared to the previous MRI. Patient’s haemoglobin improved between 9-10 g/dl after receiving two units of packed red blood cells. She was discharged on the fifteen day with residual left arm upper weakness. All the known causes of stroke including thrombus formation was investigated and ruled out in this case. IDA was identified as the cause for her stroke.
Bukharovich et al. [2012] [29] described the case of a 49-year-old lady with history of severe menorrhagia who presented with new onset of left hemiparesis. MRI of the brain showed multiple small infarcts with restricted diffusion throughout the right cerebral white matter and cortex. Laboratory studies showed IDA, with haemoglobin of 8.4 g/dL, MCV of 68 fL, MCH of 20, elevated platelets of 567,000/mL. Iron studies showed: ferritin of 15ng/mL, serum iron of 20 µg/dL, and transferrin of 263 mg/dL. Transoesophageal echogram [TEE] showed a large mobile thrombus in the mid aortic arch. Patient received warfarin anticoagulation and oral iron therapy. Her neurological symptoms improved and was able to ambulate independently. She was discharged home. In this case severe IDA was identified as the cause of the hypercoagulable state and acted as a co factor for thromboembolism.
Yakushiji et al. [2005] [28] reported the case of a 50-year-old pale and emaciated [Body mass index 15.2] lady who presented to the hospital with sudden onset of disturbance in consciousness. She was drowsy, aphasic and had right sided hemiplegia. She had history of anorexia since the age of 17 and occasional haematochezia for 2 months before the admission. No risk factors were identified other than smoking. Laboratory examinations revealed haemoglobin level of 5.5 gm/dl and ferritin level of 21 μg /dl. There was no identifiable cause for IDA except internal haemorrhoids. Brain diffusion-weighted imaging showed an acute infarction in the left middle cerebral artery area. Her IDA improved with blood transfusion. She was discharged from hospital on warfarin therapy. Patient had no recurrence of stroke, IDA or thrombophilia after 2 years follow up.
In the same study, Yakushiji et al. [2005] [28] reported another case of a 41-year-old female who presented with sudden onset of dysarthria and right sided hemiplegia. She had epimenorrhagia since the age of 20 years. Laboratory examinations revealed haemoglobin level of 7.9 gm/dl and ferritin level of 2 μg /dl. Adenomyosis uteri was identified as the cause of IDA. Brain diffusion-weighted imaging showed acute infarctions in the bilateral cerebellum and the territories of the left middle cerebral artery and the left anterior cerebral artery. Patient’s IDA was successfully treated with ferro therapy. She was discharged from hospital with mild right sided hemiplegia on warfarin and ferro therapy. In the two cases reported by Yakushiji et al. [2005] [28], severe IDA was considered as a contributing factor of stroke.
The case of a 28-year-old male who presented with severe fatigue, dizziness, blurred vision, esotropia, diffuse retinal haemorrhage and Roth spots in the left eye was described in another case report [Fluss et al. 2019] [25]. Patient’s Hb level on admission was only 1.12 g/dl. Laboratory results also revealed thrombocytopenia with platelet count of 16000/µL. MRI brain revealed evidence of stroke in the right periaqueductal gray [PAG]. Patient had no past medical history of anaemia or thrombocytopenia. He endorsed heavy marijuana and alcohol use. After extensive workup, microcytic anaemia likely due to iron deficiency was found. Interestingly, after receiving three units of packed red blood cells [pRBC], the patient’s presenting clinical symptoms, including focal neurological deficit of esotropia began resolving. Haemoglobin level post treatment is not mentioned in the study. IDA was identified as the cause of stroke in this patient.
The case of a 41-year-old man who developed acute stuttering, right upper extremity weakness and paraesthesia’s associated with mild slurred speech and right facial droop was reported in the case study of Roshal [2016] [27]. Patient also stated having several episodes of right upper extremity numbness and intermittent tingling over that past month. His past medical history was remarkable for rectal bleeding. Patient’s Hb was 8.9 g/dl, haematocrit 30.8%, mean corpuscular volume [MCV] 59.6 fL, and platelets 355,000/ μL. Serum iron was 14 μg/dL, ferritin 2.1 ng/mL, total iron binding capacity 480 μg/dL and transferrin saturation 3%. Severe iron deficiency in this case was attributed to a gastrointestinal source. His NIHSS was 2 which included a mild right lower facial droop and upper extremity pronator drift. MRI of the brain showed acute and sub-acute embolic small volume cortical infarcts in the left middle cerebral artery territory as well as an old right frontal wedge-shaped moderate volume cortical embolic infarct. This patient received intravenous iron replacement and no recurrent ischemic emboli event was reported. Stroke workup did not provide a reasonable aetiology for his symptoms. IDA was identified as the cause of ischaemic stroke in this patient. This case report suggests that severe IDA should be viewed as a risk factor for ischaemic stroke, especially in young adults.
Table 1: Characteristics of the included studies
| Author & year |
Demographics & Country |
Method of stroke diagnosis |
Type of study |
Haemoglobin level on admission |
Past medical History |
Diagnosis | Treatment given |
Duration of follow up |
Outcome of the study |
|---|---|---|---|---|---|---|---|---|---|
|
Yakushiji et al (2005) |
52 yr/F Japan 41 yr /F Japan |
Brain diffusion weighted imaging Brain diffusion weighted imaging |
Case Report Case Report |
5.5 gm/dl 7.9 gm/dl |
Haematochezia, anorexia, internal haemorrhoids, smoking Epi -menorrhagia since the age of 20 |
Left MCA infarct. Acute infarctions in the bilateral cerebellum and the territories of the left middle cerebral artery and the left anterior cerebral artery |
Blood transfusion and heparin infusion. Heparin Infusion, Ferro therapy |
2 years 6 months |
Discharged from hospital on warfarin therapy. Patient was discharged from hospital with mild right sided hemiplegia on warfarin and ferro therapy. |
|
Dubyk et al. (2012) |
Elderly patients ≥ 65 years of age (n=94) USA |
Not mentioned |
Case control Prospective study |
Mean (SD) F 132 (15) M 147 (14) |
Not mentioned | Not mentioned | Not mentioned | 6 years |
84% (n=79) of subjects presented with stroke. The overall prevalence of IDA in the sample of stroke and TIA patients was 6.4% accounting for 40% of all the cases. Bivariate analysis was used to examine the association between single predictor variables and outcome measures of iron status. |
| Mehta et al (2012) |
47 yr./F USA |
MRI Brain | Case Report | 7.6 gm/dl |
IDA and menorrhagia due to uterine fibroid. |
Acute infarction in the right middle cerebral artery. |
2 units of packed red blood cells |
15 days |
Discharged on day 15 with residual left arm upper weakness. |
|
Bukharovich et al. (2012) |
49 yr/F USA |
MRI Brain | Case Report | 8.4 gm/dl | Severe Menorrhagia |
Multiple small infarcts with restricted diffusion throughout the right cerebral white matter and cortex |
Heparin, iron | 10 days |
The patient’s neurological status improved rapidly, and she was transferred to the inpatient rehabilitation unit. Ten days after admission she was discharged on warfarin anticoagulation and oral iron therapy and was able to ambulate independently |
|
Naito et al. (2014) |
Case 1 42 yr/F Japan Case 2 42yr/F Japan |
MRI Brain MRI brain |
Case Report Case Report |
5.3 gm/dl 9.1 mg/dl |
3-year history of menorrhagia and one year history of IDA. Two-year history of menorrhagia |
Acute ischemic stroke Sub-acute cerebral infarction |
Refused bloodtransfusion but received intravenous iron therapy, Uterine fibroid was surgically removed. Refused oral iron therapy Uterine fibroid was surgically removed |
15 months Not mentioned |
Discharged home. There was no evidence of ischemic stroke at her 15 months follow up. Discharged with no recurrence of ischemic stroke. |
| Roshal D (2016) |
41 yr./M USA |
MRI Brain | Case Report | 8.9 gm/dl |
Rectal bleeding. On no medications |
Acute and subacute ischemic infarcts in the left middle cerebral arterial territory |
Intravenous iron replacement, and warfarin. |
3 months |
Discharged home on oral anti thrombotic agents and aggressive iron replacement therapy with a plan for repeat vascular imaging in 3 months and a colonoscopy. |
|
Gopalratnam et al. (2017) |
20 yr/F USA |
MRI Brain | Case Report | 5.8 mg/dl |
Menorrhagia with multiple evaluations for near syncope and dizziness. |
Bilateral cerebellar and left occipital lobe ischemic infarction |
Multiple blood transfusion, intravenous iron infusion, and ferrous sulphate 325 mg TID. She was enrolled into physical and speech therapy. |
Two weeks |
Discharged home on the fifteenth day with residual left arm upper weakness with follow up in resident’s continuity clinic. |
|
Fluss et al. (2019) |
28 yr. /M USA |
MRI Brain | Case Report | 1.12g/dl |
Heavy marijuana and alcohol consumption |
Stroke in the periaqueductal gray |
Six units of packed red blood cells (pRBC)and one unit platelet over next three days. |
Not mentioned |
After three units of pRBC, his presenting clinical symptoms including his focal neurologic deficit of esotropia began resolving. |
|
Nisar & Hanumanthu (2019) |
48/F USA |
MRI Brain | Case Report | 6.0 g/dl | menorrhagia |
Right frontal lobe and left cerebellar hemisphere infarction |
One-unit red blood cells anticoagulation |
8 months |
Discharged on warfarin, aspirin, and iron supplementation |
|
Zhang et al. (2020) |
29/ F USA |
MRI Brain | Case Presentation | 7.8 gm/dl |
Obesity, gastric sleeve surgery, menorrhagia, IDA. She had a long history of IDA due to menorrhagia since she was 12. |
Acute left occipital lobe infarction |
Two units of red blood cells IV iron infusion x 5 days Folic acid daily |
Not mentioned |
Discharged home with outpatient haematologist follow up for iron transfusion hypercoagulable work up. |
| Awad et al. (2020) |
42/F USA |
MRI Brain | Case Report | 7.7gm/dl | menorrhagia |
Infarct of right middle cerebral artery and anterior cerebral artery territories |
Commenced on oral doses of 325 mg ferrous sulphate alternate days |
6 months |
Discharged home on aspirin, atorvastatin, and ferrous sulphate. |
|
Kandinata et al. (2021) |
34 yr/F USA |
MRI Brain | Case report | 9.1gm/dl | Menorrhagia |
Multifocal acute infarct |
Intravenous iron infusion |
Not mentioned |
No adverse outcome. |
Table 2: Demography of the participants.
| Author and year | Age of the participants in years | Number of participants (n) | Sex of the participant |
|---|---|---|---|
| Yakushiji et al. (2005) | 50 and 41 | n=2 | Females |
| Dubyk et al. (2011) | ≥ 65 |
n= 94 (Males=47 Females= 47) |
Both male and female |
| Bukharovich et al. (2012) | 49 | n=1 | Female |
| Mehta et al (2012) | 47 | n=1 | Female |
| Naito et al. (2014) | 42 42 |
n=2 | Female Female |
| Roshal (2016) | 41 | n=1 | Male |
| Gopalratnam et al. (2017) | 20 | n=1 | Female |
| Nisar & Hanumanthu (2019) | 48 | n=1 | Female |
| Fluss et al. (2019) | 28 | n=1 | Male |
| Zhang et al. (2020) | 29 | n=1 | Female |
| Awad et al. (2020) | 42 | n=1 | Female |
| Kandinata et al (2021) | 34 | n=1 | Female |
Table 3: Serum haemoglobin and iron level in the included studies
| Author and year |
Haemoglobin level (Normal 12-16 gm/dl) |
Iron level (Normal 37-170 μg /dl) |
Ferritin level (Normal 8-250 ng/ml) |
Total iron binding capacity (Normal 250- 550 μg /dl) |
Haematocrit (Normal 36- 48%) |
Iron saturation (Normal 18- 50%) |
|---|---|---|---|---|---|---|
|
Yakushiji et al. (2005) |
5.5 gm/dl 7.9 gm/dl |
16 μg /dl 9 μg /dl |
21 μg /dl 2 μg /dl |
Not mentioned | 20% 25% |
Not mentioned |
| Dubyk et al. (2011) |
Mean (SD) F 132 (15) M 147 (14) |
Not mentioned |
Mean (SD) F 90 (71) M 210 (402) |
Mean (SD) F 56 (11) M 50 (11) |
Not mentioned | Not mentioned |
|
Bukharovich et al. (2012) |
8.4 gm/dl | 20 μg /dl | 15 ng/ml | Not mentioned | Not mentioned | Not mentioned |
| Mehta et al (2012) | 7.6 gm/dl | Not mentioned | 4.6 ng/ml | Not mentioned | 23% | Not mentioned |
| Naito et al. (2014) | 5.3 g/dl 9.1 g/dl |
11 μg /dl 14 μg /dl |
4.0 ng/dl 3.6 ng/ml |
359 μg /dl 400 μg /dl |
20.4% 37.5% |
Not mentioned |
| Roshal D (2016) | 8.9 gm/dl | 14 μg /dl | 21 ng/dl | 480 μg /dl | 30.8% | 3% |
|
Gopalratnam et al. (2017) |
5.8 mg/dl | 20 μg /dl | 39 ng/dl | 481 μg /dl | Not mentioned | 6% |
|
Nisar & Hanumanthu (2019) |
6.0 gm/dl | 11 μg /dl | 4 ng/dl | 425 μg /dl | Not mentioned | Not mentioned |
| Fluss et al (2019) | 1.12 gm/dl | Not mentioned | Not mentioned | Not mentioned | Not mentioned | Not mentioned |
| Zhang et al. (2020) | 7.8 g/dl | 11 μg /dl | < 1 ng/ml | 395 μg /gl | 26.1% | 3% |
| Awad et al. (2020) | 7.7 gm/dl | 16 μg /dl | 7 ng/ml | 373 μg /dl | 27.3% | 4% |
|
Kandinata et al (2021) |
9.1 gm/dl | 10 ug/dL | 3.2 ng/mL | 338 ug/dL | 31.3% | 3% |
Table 4: Excluded studies.
| Author | Article | Reason for exclusion |
|---|---|---|
| Shar and Sadeh (1990) | Severe anaemia associated with transient neurological deficits | Does not fit the inclusion criteria. |
| Huang et al. 2008 |
The influence of anaemia on
clinical presentation and
outcome of patients with first -ever atherosclerosis- related ischaemic stroke |
Does not fit the inclusion criteria |
| Barlas et al.2016 |
Impact of haemoglobin levels
and anaemia on mortality in
acute stroke: Analysis of UK Regional Registry Data, Systematic Review, and Meta analysis |
Does not fit the inclusion criteria |
| Maguire et al.2007 | Association between iron deficiency anaemia and stroke in young children | Does not fit the inclusion criteria |
| Bruggers et al.1990 | Reversible focal neurologic deficits in severe iron deficiency anaemia | Does not fit the inclusion criteria |
| Petrova et al. | Is there a link between changes in levels of hepcidin and stroke | Does not fit the inclusion criteria |
| Dan 2005 | Thrombocytosis and iron deficiency anaemia | Does not fit the inclusion criteria |
| Franchini et al. 2007 | Iron and Thrombosis | Does not fit the inclusion criteria |
| Chang et al (2013) |
Association between Ischemic
Stroke and Iron-Deficiency
Anaemia: A Population-Based Stud |
Serum iron/haemoglobin level
not mentioned in the study. |
| Choi et al. (2013) |
Ischemic Stroke Related to
Severe Iron-Deficiency
Anaemia in Adults May Benefit from Blood Transfusion |
Full text article not available. |
In all these cases, patients presented with neurological symptoms and low haemoglobin level. Their neurological symptoms resolved as their haemoglobin level improved. Some of the patients received warfarin.
Predictors of IDA: In the included studies, nine case reports identified menorrhagia as the main cause of IDA in females [5,6,9,16,17,26,28-30]. Among males, rectal bleeding and heavy consumption of alcohol and marijuana was reported as the cause of IDA [Fluss et al. [2019] [25], Roshal [2016] [27]. Dubyk et al [2012] [12] reported gender as a highly significant predictor of haemoglobin [P = <0.01].
Methodological quality of the included studies
In all the included case reports, patient’s demographic characteristics, patient’s history, and the clinical condition of the patient on presentation are clearly described. Also, the diagnostic tests and the results, interventions/treatment procedures and post intervention clinical condition are clearly explained. Any adverse events or unanticipated events are not stated in any of the included case reports. Moreover, the case reports summarize key lessons learned from the cases in terms of the background of the condition/ disease and clinical practice guidance for clinicians when presented with similar case. JBI Critical Appraisal checklist for case control study was used to check the quality of the included case control studies. In the case control study [12]. The groups are comparable thus reducing the risk of selection bias. Case and controls are matched appropriately and has measured exposure in a standard, valid, and reliable way [12]. Moreover, the study has described the confounding factors identified, and the strategies to deal with confounding factors. Outcomes were assessed in a standard, valid, and reliable way for cases and controls [12]. Exposure time was sufficient to show an association between the exposure and the outcome in the study.
Discussion
The overall aim of this SR was to investigate the association between IDA and ischaemic stroke. The primary outcome of this SR identified a potential link between IDA and ischaemic stroke. In the included case reports patients who presented with stroke symptoms had significantly low haemoglobin level [6,9,16,17,25-30]. Their stroke symptoms resolved with iron infusion or blood transfusion. Understanding of the association between IDA and ischemic stroke is vital for the prevention and treatment of ischemic stroke and to prevent morbidities associated with stroke [45]. IDA is a manifestation of poor health [46]. Additionally, IDA frequently occurs in many chronic inflammatory conditions including congestive cardiac failure, chronic kidney disease and inflammatory bowel disease [47].
Stroke is a main cause of neurological disability, not only in the older person, but also in younger age groups [34,35]. The effect of stroke depends on the site and severity of brain injury [36]. Choi et al. [2013] [31] reported that the prevalence of IDA among patients with acute ischaemic stroke is 3.9%.
From the above included twelve studies it is evident that IDA is a risk factor for ischemic stroke and the severity of stroke increases with low haemoglobin level. A positive association between severity of anaemia and risk of stroke was identified by Chen et al [2023] [48]. Another study [37] depicts anaemia as the “fifth cardiovascular risk factor” next to smoking, diabetes mellitus (DM), hypertension, and hypercholesterolemia. Data from the Acute Stroke Registry and Analysis of Lausanne (ASTRAL) suggested that anaemia on admission predicts short- and long-term outcomes in patients with acute ischemic stroke [38]. Nationwide data base survey from Taiwan [13] disclosed that there is substantial correlation between IDA and ischemic stroke in adults. In one study [36], out of 50 cases of stroke, 37 cases (74%) were anaemic, and 21 cases (42%) had moderate degree of anaemia suggesting that anaemia is also one of the contributing factors for stroke. The Framingham study highlighted the need to further explore the pathogenetic, preventive and therapeutic implications of the interrelation of haemoglobin level and stroke [39]. The population-based cohort study [40] identified that anaemic female patients in the reproductive age group had an associated high risk of stroke. The study of Sui et al [2020] [40], reported that anaemia is a potential risk factor for stroke among females of reproductive age group.
The correlation of stroke and iron deficiency anaemia has been explained based on three physiological mechanisms [36]. A hypercoagulable state, thrombocytosis and hypoxia [36]. Hypercoagulability or thrombophilia is the increased tendency of blood to thrombose [41], thrombocytosis refers to an increased platelet count in the blood [42] and hypoxia refers to low level of oxygen in the blood [43]. A decrease in haemoglobin level in the blood compromises oxygen carrying capacity of the blood flow resulting in low oxygen delivery to brain. This leads to hypoxia and increases the risk of cerebrovascular diseases [36]. Besides this, secondary thrombocytosis may also explain the link between IDA and ischaemic stroke [36]. Carotid thrombus associated with IDA is already reported in adults [5]. Anaemic patients need more blood to flow to the brain to compensate for the lack of oxygen [36]. Hence, increase in blood flow can provoke endothelial damage, and thus thrombus formation and subsequent reactive thrombocytosis [25,36].
IDA can be caused by blood loss [e.g., menstrual loss, blood lost through gastrointestinal tract, genito urinary tract, hook worm infestation etc.], poor dietary intake, poverty, malnutrition, and poor absorption of iron (e.g., after bariatric surgery, inflammatory bowel disease, celiac disease etc) [44].In the included case studies menorrhagia was the cause of IDA in nine cases reports [5,6,9,16,17,26,28-30]. Two cases reported IDA due to rectal bleeding [25,27].
One study revealed that blood transfusion may be considered as an adjuvant therapy in the treatment of stroke patients [36]. In all the included case studies, the patients either received blood transfusion or iron replacement therapy either oral or intravenous with good outcomes. From this review and discussion, it is obvious that IDA is a preventable and treatable cause of stroke in adults, especially females. Appropriate timely management of IDA can prevent permanent neurological complications and possibly recurrence of stroke.
Limitations: The included studies are heterogenous in nature in terms of study design, sample size, type of intervention and the measured outcome. The findings from this study may not be generalizable as most of the included studies were case reports.
Recommendation: Upon admission of a stroke patient, anaemia should be ruled out. A diagnostic workup toward reversible causes should be implemented. Having iron studies as part of stroke work up may be beneficial in the prompt diagnosis and treatment of IDA in the early stage of stroke. It helps to improve prognosis and outcome in patients who had stroke secondary to IDA [25]. Considering the socio-economic burden of stroke, anaemic female patients in the reproductive age group should be informed of their high risk for stroke. These patients should be very vigilant for any stroke symptoms and should seek immediate medical attention.
Conclusion
IDA should be considered as a potential cause of ischemic strokes when other possibilities have been ruled out. It is important to identify and treat patients with severe IDA in order to reduce the risk of subsequent ischemic stroke. IDA has been overlooked as a risk factor for ischemic stroke. Even though the pieces of information from the included case reports suggest a strong association between IDA and stroke, the findings need to be substantiated by further studies.
Funding: None.
Conflict of interest: None.
Ethics approval: Not required.
References
- Engelhardt E. Apoplexy, cerebrovascular disease, and stroke: Historical evolution of terms and definitions. Dementia & Neuropsychologia. 2017; 11(4): 449-453.
- World Stroke Organisation (WSO) Global Stroke Fact Sheet 2022, Retrieved from https://www.worldstroke.org/assets/downloads/WSO_Global_Stroke_Fact_Sheet.pdf on 20/11/2022
- Campbell B, De Silva D, Macleod M, Coutts S, Schwamm L, Davis S et al. Ischaemic stroke. Nature Reviews Disease Primers. 2019; 5(1).
- Tadi P, Lui F. Acute stroke (cerebrovascular accident). StatPearls. Treasure Island, FL: StatPearls Publishing. 2020 Jan.
- Mehta P, Chapman S, Jayam-Trouth A, Kurukumbi M. Acute Ischemic Stroke Secondary to Iron Deficiency Anemia: A Case Report. Case Reports in Neurological Medicine. 2012; 2012: 1.
- Awad D, Kousa O, Essa A, Kuniyoshi J, Kousa H, Qasim A et al. Acute ischemic stroke as initial manifestation of undiagnosed iron deficiency anemia: case-report and literature review. AME Case Reports. 2020; 4: 23-23.
- Jimenez K, Kulnigg-Dabsch S, Gasche C. Management of iron deficiency anemia. Gastroenterology & hepatology. 2015; 11(4): 241-250.
- Kumar A, Sharma E, Marley A, Samaan MA, Brookes MJ. Iron deficiency anaemia: pathophysiology, assessment, practical management. BMJ open gastroenterology. 2022; 9(1): e000759.
- Gopalratnam K, Woodson K, Rangunwala J, Sena K, Gupta M. A Rare Case of Stroke Secondary to Iron Deficiency Anemia in a Young Female Patient. Case Reports in Medicine. 2017; 2017: 1-3.
- Alexander M. Iron Deficiency Anemia, Thrombocytosis, and Cerebrovascular Accident. Southern Medical Journal. 1983; 76(5): 662-663.
- Knizley H. Iron Deficiency Anemia, Papilledema, Thrombocytosis, and Transient Hemiparesis. Archives of Internal Medicine. 1972; 129(3): 483.
- Dubyk M, Card R, Whiting S, Boyle C, Zlotkin S, Paterson P. Iron Deficiency Anemia Prevalence at First Stroke or Transient Ischemic Attack. Canadian Journal of Neurological Sciences / Journal Canadien des Sciences Neurologiques. 2012; 39(2): 189-195.
- Chang Y, Hung S, Ling W, Lin H, Li H, Chung S. Association between Ischemic Stroke and Iron-Deficiency Anemia: A Population-Based Study. PLoS ONE. 2013; 8(12): e82952.
- Caglayan HB, Nazliel B, Irkec C, Dumlu A, Filiz A, Ates MP. Iron-deficiency anemia leading to transient ischemic attacks due to intraluminal carotid artery thrombus. Case reports in neurological medicine. 2013; 2013.
- Khan MF, Shamael I, Zaman Q, Mahmood A, Siddiqui M. Association of anemia with stroke severity in acute ischemic stroke patients. Cureus. 2018; 10(6).
- Zhang Q, Shan KS, O’Sullivan C, Nace, T. Iron Deficiency Anemia: An Unexpected Cause of an Acute Occipital Lobe Stroke in an Otherwise Healthy Young Woman. Cureus. 2020; 12(4).
- Naito H, Naka H, Kanaya Y, Yamazaki Y, Tokinobu H. Two Cases of Acute Ischemic Stroke Associated with Iron Deficiency Anemia due to Bleeding from Uterine Fibroids in Middle-aged Women. Internal Medicine. 2014; 53(21): 2533-2537.
- Shahar A, Sadeh M. Severe anemia associated with transient neurological deficits. Stroke. 1991; 22(9): 1201-1202.
- Keung Y, Owen J. Iron Deficiency and Thrombosis: Literature Review. Clinical and Applied Thrombosis/Hemostasis. 2004; 10(4): 387-391.
- Barlas R, Honney K, Loke Y, McCall S, Bettencourt‐Silva J, Clark A et al. Impact of Hemoglobin Levels and Anemia on Mortality in Acute Stroke: Analysis of UK Regional Registry Data, Systematic Review, and Meta‐Analysis. Journal of the American Heart Association. 2016; 5(8).
- Stolz E, Valdueza J, Grebe M, Schlachetzki F, Schmitt E, Madlener K et al. Anemia as a risk factor for cerebral venous thrombosis? An old hypothesis revisited. Journal of Neurology. 2007; 254(6): 729-734.
- Khan MF, Shamael I, Zaman Q, Mahmood A, Siddiqui M. Association of anemia with stroke severity in acute ischemic stroke patients. Cureus. 2018; 10(6).
- PRISMA [Internet]. Prisma-statement.org. 2021 [cited 7 November 2021]. Available from: http://www.prisma-statement.org/PRISMAStatement/FlowDiagram.aspx
- JBI critical appraisal tool [Internet].[cited 10 January 2021]. Available from https://jbi.global/critical-appraisal-tools
- Fluss R, Zguri L, Rahme R, Fulger I. Iron-deficiency anemia causes an ischemic stroke in a young man. Cureus. 2019; 11(3).
- Nisar T, Hanumanthu R. Cerebral Ischemia due to Aortic Arch Thrombosis Secondary to Iron Deficiency Anemia. Case reports in neurological medicine. 2019.
- Roshal D. Embolic stroke due to a common carotid artery thrombus in a young patient with severe iron-deficiency anemia without thrombocytosis. Case reports in neurological medicine. 2016.
- Yakushiji Y, Terasaki Y, Otsubo R, Yasaka M, Oe H, Yamada N, Nishigami K, Naritomi H, Minematsu K. Brain embolism caused by a mobile aortic thrombus with iron deficiency anemia. Cerebrovascular Diseases. 2005; 20(6): 475.
- Bukharovich IF, Wever-Pinzon O, Shah A, Todd G, Chaudhry FA, Sherrid MV. Arterial embolism caused by large mobile aortic thrombus in the absence of atherosclerosis, associated with iron deficiency anemia. Echocardiography (Mount Kisco, NY). 2012; 29(3): 369.
- Kandinata NN, Breehl L, Chhetri B, Paudel S, Breehl LL, Chhetri BK. Stroke secondary to iron deficiency anemia: a case report. Cureus. 2021; 13(11).
- Choi E, Sanchez-Rotunno M, Gonzales N. Ischemic Stroke Related to Severe Iron-Deficiency Anemia in Adults May Benefit from Blood Transfusion. Neurology. 2013. 80(1) (P01. 232).
- Anaemia [Internet] .World Health Organisation. [Cited 28 January 2021]. Available from https://www.who.int/health-topics/anaemia#tab=tab_1
- Johnson-Wimbley TD, Graham DY. Diagnosis and management of iron deficiency anemia in the 21st century. Therapeutic advances in Gastroenterology. 2011; 4(3): 177-84.
- Mikulik R, Wahlgren N. Treatment of acute stroke: an update. Journal of internal medicine. 2015; 278(2): 145-65.
- Maguire JL, Deveber G, Parkin PC. Association between iron-deficiency anemia and stroke in young children. Paediatrics. 2007; 120(5): 1053-7.
- Joshi A, Agrawal S. Iron Deficiency Anaemia as a Risk Factor for Stroke. OSR Journal of Dental and Medical Sciences (IOSRJDMS). 2016; 12: 42-44.
- Kaiafa G, Savopoulos C, Kanellos I, Mylonas KS, Tsikalakis G, Tegos T, Kakaletsis N, Hatzitolios AI. Anemia and stroke: Where do we stand? Acta Neurol Scand. 2017; 135(6): 596-602.
- Milionis H, Papavasileiou V, Eskandari A, D’Ambrogio-Remillard S, Ntaios G, Michel P. Anemia on admission predicts shortand long-term outcomes in patients with acute ischemic stroke. International Journal of Stroke. 2015; 10(2): 224-30.
- Kannel WB, Gordon T, Wolf PA, McNamara P. Hemolobin and the risk of cerebral infarction: The framingham study. Stroke. 1972; 3(4): 409-20.
- Sui Y, Hong CT, Chien LN, Liu HY, Chiou HY, Hsieh YC. Association between anemia and stroke in females: A nationwide, population-based cohort study in taiwan. International journal of environmental research and public health. 2020; 17(20): 7440.
- Senst B, Tadi P, Basit H, Jan A. Continuing Education Activity.
- Bleeker JS, Hogan WJ. Thrombocytosis: diagnostic evaluation, thrombotic risk stratification, and risk-based management strategies. Thrombosis. 2011.
- Bhutta BS, Alghoula F, Berim I. Hypoxia. InStatPearls [Internet] 2022. StatPearls Publishing.
- DeLoughery TG. Iron Deficiency Anemia. Med Clin North Am. 2017; 101(2): 319-332.
- Heo J, Youk TM, Seo KD. Anemia is a risk factor for the development of ischemic stroke and post-stroke mortality. Journal of Clinical Medicine. 2021; 10(12): 2556.
- Cappellini MD, Musallam KM, Taher AT. Iron deficiency anaemia revisited. Journal of internal medicine. 2020; 287(2): 153-70.
- Kumar A, Sharma E, Marley A, Samaan MA, Brookes MJ. Iron deficiency anaemia: pathophysiology, assessment, practical management. BMJ open gastroenterology. 2022; 9(1): e000759.
- Chen HF, Ho TF, Kuo YH, Chien JH. Association between Anemia Severity and Ischemic Stroke Incidence: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2023; 20(5): 3849.
