
Open Access, Volume 9
Sustained complete response to chemotherapy in a patient with advanced merkel cell carcinoma: A case report
Alejandro Noguez-Ramos1,2; Eleonora Pisa3; Laura Gilardi4; Nicola Fazio1*
1Division of Gastrointestinal Medical Oncology and Neuroendocrine Tumors, European Institute of Oncology, IEO, IRCCS, Via Giuseppe Ripamonti, 435, 20141 Milan, Italy.
2 Division of Medical Oncology, ABC Medical Center. Sur 136, 116, 01120 Mexico City, Mexico.
3Division of Pathology, European Institute of Oncology, IEO, IRCCS, Via Giuseppe Ripamonti, 435, 20141 Milan, Italy.
4Division of Nuclear Medicine, European Institute of Oncology, IEO, IRCCS, Via Giuseppe Ripamonti, 435, 20141 Milan, Italy.
Nicola Fazio
Division of Gastrointestinal Medical Oncology and Neuroendocrine Tumors, European Institute of Oncology, IEO, IRCCS, Via Ripamonti 435, Milan 20141, Italy
Email: nicola.fazio@ieo.it
Received : July 27, 2023,
Accepted : Sep 18, 2023
Published : Sep 22, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Merkel cell carcinoma (MCC) is a rare neuroendocrine skin cancer. Over the last decade immune checkpoint inhibitors (ICIs) replaced chemotherapy as the recommended first-line therapy option. Across nonrandomized studies chemotherapy showed an overall response rate (ORR) ranged from 50% to 60%, a complete response (CR) rate from 3% to 30% and a progression free survival (PFS) of 3-4 months.
We report a clinical case regarding a 72-year-old woman with MCC with right gluteus cutaneous lesion and inguinal and iliac lymph-adenopathies at diagnosis. The initial treatment was based on systemic chemotherapy with carboplatin + etoposide followed by lymphadenectomy. A pancreatic recurrence occurred after thirteen months, histologically confirmed. Systemic chemotherapy with the same regimen yielded a CR without a further progression for the subsequent eight years. The patient died due to nononcological causes, MCC-free, 11 years after the diagnosis.
This case is reported to highlight the chemotherapy efficacy in MCC in the immunotherapy era.
Keywords: Merkel cell carcinoma; Neuroendocrine tumor; Complete response; Chemotherapy.
Abbreviations: CR: complete response, CT-scan: computerized tomography scan, DoR: duration of response, ICIs: immune checkpoint inhibitors, MCC: Merkel cell carcinoma, ORR: overall response rate, OS: overall survival, PR: partial response, PFS: progression free survival, SRS: somatostatin receptor scintigraphy, 18F-FDG-PET/CT: Positron emission tomography with 2-deoxy-2-[fluorine-18] fluoro- D-glucose integrated with computed tomography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Fazio N (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Noguez-Ramos A, Pisa E, Gilardi L, Fazio N. Sustained complete response to chemotherapy in a patient with advanced Merkel cell carcinoma: A case report. Open J Clin Med Case Rep. 2023; 2116.
Background
Merkel Cell Carcinoma (MCC) is a rare and aggressive neuroendocrine skin cancer characterized by high risk of recurrence and poor prognosis at an advanced stage [1].
The incidence ranges from 0.1 to 1.6 new cases/100,000 people per year worldwide, the average age at diagnosis is 69 years, and male/female ratio is 2:1 [1,2]. At the time of diagnosis about 65% of patients have localized disease, 26% regional nodal involvement and 8% distant metastasis [3]. The rate of overall survival (OS) at 5 years ranges from 62% in stage I to 13% in stage IV [2,3].
The etiology of MCC is debated, with some theories proposed, including Merkel cell polyomavirus (MCPyV) infection, exposure to UV radiation and immunosuppression [4-6].
The diagnosis is made with histopathology, showing cells with neuroendocrine but also epithelial markers such as synaptophysin, chromogranin-A (CgA), cytokeratin 20 (CK-20) and neurofilaments (NF); MCpyV can be present [7,8].
For localized MCC surgical resection with 1-2 cm margin is the mainstream treatment and usually is followed by adjuvant radiotherapy if there is a positive margin or if there are risk factors for recurrence. In borderline resectable or unresectable locoregional disease it could be possible to consider preoperative systemic treatment; and in metastatic setting the recommended treatment is immunotherapy, with chemotherapy as second option [9].
We report a clinical case regarding a patient successfully treated with chemotherapy years ago, before the advent of immunotherapy.
Case Presentation
We present a 72-year-old woman, without comorbidities, and metastatic MCC. In July 2008 she came to the European Institute of Oncology after having undergone an excisional biopsy of a cutaneous lesion in the right gluteus. The patient reported that this lesion had appeared two years earlier and spontaneously regressed after some time. The pathology report concluded for MCC. the Immunohistochemical analysis was positive for CgA, CK-20, NF and synaptophysin, and negative for TTF-1 and desmin; Ki-67 was 90%, MCPyV was detected without any point mutation (Figure 1).
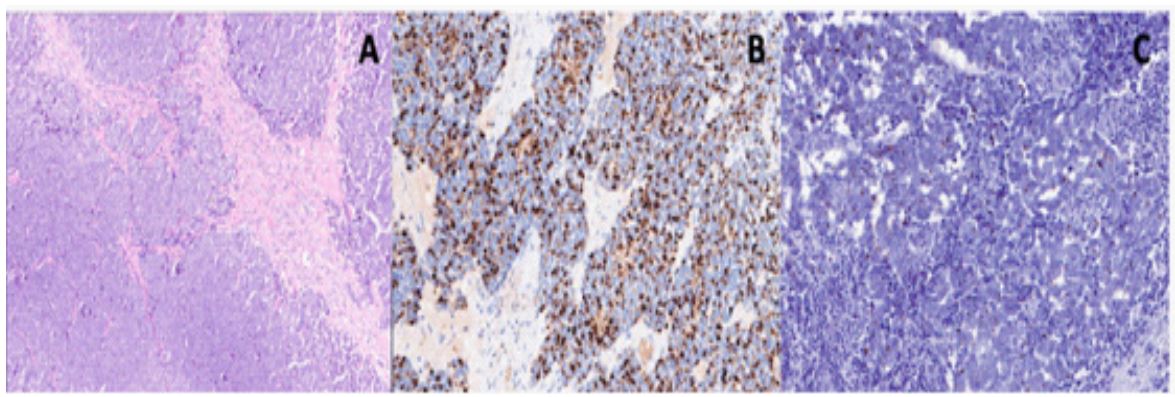
Figure 1: A: Hematoxylin and Eosin Stain of a skin biopsy. B: Dot-like cytokeratin 20 positivity by immunohistochemistry.
C: Dot-like neurofilament positivity by immunohistochemistry.
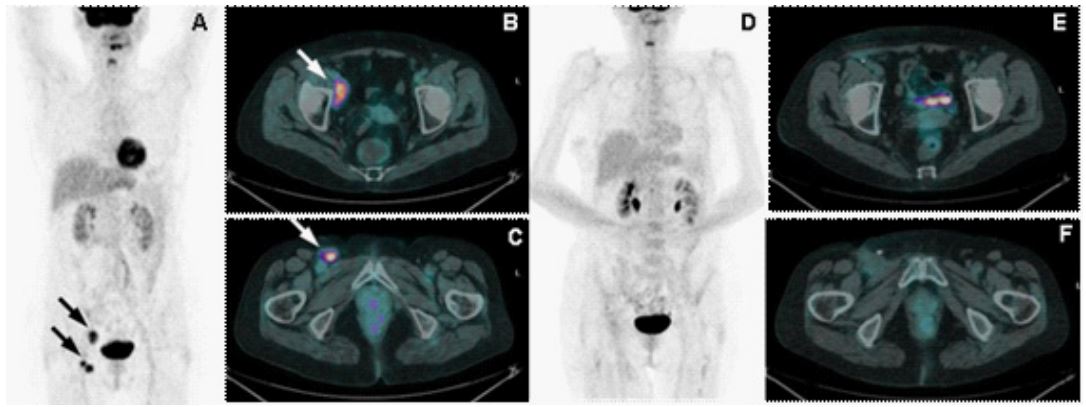
Figure 2: A: Maximum intensity projection image at diagnosis. B: high 8FDG uptake and enlargement of a right external iliac
adenopathy. C: high 18FDG uptake and enlargement of a right inguinal adenopathy. D: Maximum intensity projection image
after 3 cycles of chemotherapy. E: Non-uptake and non-enlargement of the previous right external iliac adenopathy. F: Nonuptake and non-enlargement of the previous right inguinal adenopathy
At our visit she was asymptomatic, presenting at the clinical examination palpable nodules in the right inguinal region. The Chest-Abdomen computerized tomography scan (CT-scan) showed a right external iliac (43 mm) and two inguinal lymph-nodes (20 mm). The somatostatin receptor scintigraphy (SRS) was negative, and the positron emission tomography with 2-deoxy-2-[fluorine-18] fluoro-D-glucose integrated with computed tomography (18F-FDG-PET/CT) showed high uptake in these lymph-adenopathies. (Figure 2. A, B and C).
Due to the quite extensive regional disease the European Institute of Oncology multidisciplinary team proposed systemic chemotherapy with carboplatin AUC 5 day 1 + etoposide 100 mg/m2 days 1-3 every 3 weeks. After three chemotherapy cycles, a radiological tumor response was observed (Figure 2. D, E and F). Therefore, in December 2009 a right iliac-inguinal lymphadenectomy was performed. The pathologist reported one out of seven adenopathies positive for MCC. An adjuvant radiotherapy was evaluated but excluded due to high risk of toxicity considering the severe post-surgical right lower limb oedema. Therefore, the multidisciplinary decision was to go ahead with chemotherapy completing six total cycles.
In April 2009, after five cycles of chemotherapy, a retropancreatic area of uptake appeared at the 18F-FDG-PET/CT, without clear morphological alteration at the CT-scan. Due to the not sure relapse the multidisciplinary team decided to complete chemotherapy performing the sixth cycle and subsequently perform an active surveillance with CT-scan and clinical examination.
After thirteen months and four negative CT-scans, on May 2010 a new pancreatic lesion was observed (3.9 x 2.9 cm) at the CT-Scan, with a related uptake at the 18F-FDG-PET/CT (Figure 3. A, B and C). The patient was asymptomatic. To confirm the high suspicion of recurrence a pancreatic ultrasound-guided percutaneous biopsy was performed, which concluded for MCC. The pathologist reported positivity for cytocheratin-20, synaptophysin and focally chromogranin A; Ki-67 was 80%, pathological material was inadequate to detect MCpyV
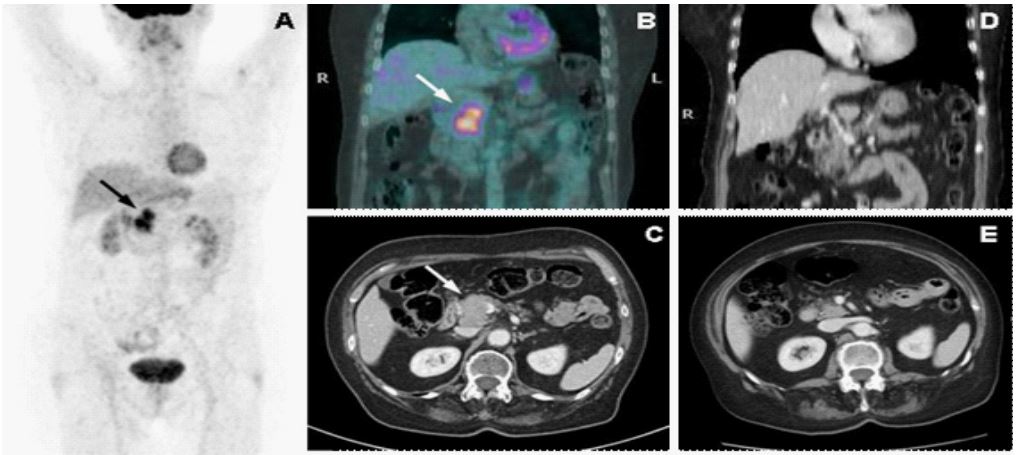
Figure 3: A: Maximum intensity projection image at diagnosis. B: high uptake pancreatic lesion in 18F-FDG-PET/CT. C: pancreatic lesion in CT-Scan. D and E: pancreatic lesion complete response in CT-Scan after chemotherapy.
Table 1: Systemic treatment options for metastatic Merkel Cell Carcinoma.
| Treatment | Reference | Design | Line | N | OS | PFS | ORR | CR |
|---|---|---|---|---|---|---|---|---|
| Immunotherapy | ||||||||
| Avelumab | JAVELIN Merkel 200 trial [11, 12] | Phase II | First | 116 | 20.3 m | 4.1 m | 39% | 16% |
| Pembrolizumab | KEYNOTE-017 [13] | Phase II | First | 50 | NR | 16.8 m | 56% | 24% |
| Nivolumab | CheckMate 358 [14] | Phase I/II | ≥ First | 25 | - | NR | 68% | 14% |
| Avelumab | JAVELIN Merkel 200 trial [15, 16] | Phase II | ≥ second | 88 | 12.6 m | 2.7 m | 33% | 11% |
| Retifanlimab | POD1UM-201 [17] | Phase II | First | 65 | - | - | 46% | 12% |
| Chemotherapy | ||||||||
| CAV P+E D+C |
Voog E. Cancer. 1999 [22] | Case series and Review | ≥ First | 72* | 9 m | - DoR = 8 m |
57% | - |
| P+E AC |
Tai PT. J Clin Oncol. 2000 [23] | Case series and Review | Unclear | 204 | - | - | 60 - 75% | 35 - 36% |
| P+E and others. | Iyer JG. Cancer Med. 2016 [24] | Retrospective | First and second | 62 | 13 m | 3.1 m | 23 - 55% | 3 - 13% |
| P+E | Satpute S. J Clin Oncol. 2014 [25] | Retrospective | Unclear | 12** | - | 4 m | 83% | - |
AC: Cyclophosphamide + doxorubicin, CAV: Cyclophosphamide + doxorubicin + vincristine, CR: Complete Response, D+C: Doxorubicin + cisplatin, DoR: Duration of Response, NR: Not reached, ORR: Objective Response Rate, OS: Overall Survival, P+E: Platinum
+ etoposide, PFS: Progression Free Survival,
*101 patients were included, 72 in metastatic setting.
**41 patients were included, 12 in metastatic setting.
After a multidisciplinary discussion, due to the long disease-free survival and good tolerance, systemic chemotherapy with the same regimen was proposed and three cycles were administered. The subsequent CT-scan showed a RECIST-based complete response (Figure 3. D and E).
Since then, the patient periodically underwent clinical and radiological controls. The last CT-scan was done in September 2018 (eight years after diagnosis) and showed sustained CR. After a hip fracture in august 2020 the patient died without evidence of MCC (11 years after diagnosis).
Discussion
We have described the clinical case of a patient with advanced MCC, treated at a MCC-referral center prior to immunotherapy approval. This case shows a complete and sustained response to chemotherapy.
In accordance with international guidelines [9,10]. ICIs are the first line treatment for patients with advanced MCC, and chemotherapy is recommended when patients fail to respond or are intolerant to ICIs.
Currently ICIs available options include avelumab, pembrolizumab, nivolumab and retifanlimab. With this therapy the OS ranges from 12 to 20 months, PFS from 4 to 16 months, ORR from 33 to 68% and CR rates from 11 to 24% [11-17].
Immune checkpoint inhibitors have revolutionized the treatment of solid cancers. Nevertheless, is not available all around the world, the cost is high, and the cost-effective rates is variable among the tumors [18,19]. Besides, some patients are not eligible for therapy with ICIs such as those with severe autoimmune diseases, and there is limited retrospective evidence supporting their use in this scenario [20].
When ICIs is not available, fail or the patient is not eligible, then chemotherapy is the further option. International guidelines [9,10] recommend chemotherapy with platinum plus etoposide, CAV (Cyclophosphamide, doxorubicin, and vincristine) or Topotecan mainly based on case-reports, case series, retrospective studies, or reviews.
A Systematic review of chemotherapy regimens in patients with metastatic MCC [21] found 35 reports, 5 retrospective studies or literature reviews in patients with distant metastases, and showed OS from 9 to 9.5 months, PFS from 2 to 3 months, ORR of 52 - 61% in first line and 23% in second line, CR rates from 3-37%, with a median duration of response (DoR) of only 6 months [21-25] (Table 1).
The patient of our case report was treated prior to the approval of ICIs in MCC and she got not only a CR, but overall a definitive CR, benefiting in absolute from this. The CR has been reported in less than one third of patients with MCC. The reported DoR with chemotherapy is only 6 months, whereas reports of sustained responses (1 to 2.5 years) have been published with ICIs [26,27]. Our patient had a surprising DoR of more than 8 years. Merkel cell carcinoma is historically known to be an aggressive, highly relapsing, usually rapidly evolving and therefore poor-prognosis neuroendocrine skin cancer, however it is considered a chemo-sensitive cancer. Therefore, partial response (PR) or even CR were not so surprising with chemotherapy, although the DoR is usually short. In our clinical case the DoR is more surprising and unexpected than the CR. The mechanism of this is unknown but we think that a similar mechanism like that of ICIs cannot be excluded. Our case indicates that chemotherapy can sometime be successful in MCC, and therefore it should be considered even in the current era of ICIs.
References
- Spada F, Bossi P, Caracò C, Sileni VC, Dei Tos AP, et al. Nationwide multidisciplinary consensus on the clinical management of Merkel cell carcinoma: a Delphi panel. J Immunother Cancer. 2022 Jun; 10: e004742.
- Schadendorf D, Lebbé C, Zur Hausen A, Avril MF, Hariharan S, et al. Merkel cell carcinoma: Epidemiology, prognosis, therapy and unmet medical needs. Eur J Cancer. 2017; 71: 53-69.
- Harms KL, Healy MA, Nghiem P, Sober AJ, Johnson TM, et al. Analysis of Prognostic Factors from 9387 Merkel Cell Carcinoma Cases Forms the Basis for the New 8th Edition AJCC Staging System. Ann Surg Oncol. 2016; 23: 3564-3571.
- Leroux-Kozal V, Lévêque N, Brodard V, Lesage C, Dudez O, et al. Merkel cell carcinoma: histopathologic and prognostic features according to the immunohistochemical expression of Merkel cell polyomavirus large T antigen correlated with viral load. Hum Pathol. 2015; 46: 443-53
- Heath M, Jaimes N, Lemos B, Mostaghimi A, Wang LC, et al. Clinical characteristics of Merkel cell carcinoma at diagnosis in 195 patients: the AEIOU features. J Am Acad Dermatol. 2008; 58: 375-81.
- Clarke CA, Robbins HA, Tatalovich Z, Lynch CF, Pawlish KS, et al. Risk of merkel cell carcinoma after solid organ transplantation. J Natl Cancer Inst. 2015; 107: dju382.
- Wong HH, Wang J. Merkel cell carcinoma. Arch Pathol Lab Med. 2010; 134: 1711-6.
- Fried I, Cerroni L. Merkel-Zell-Karzinom [Merkel cell carcinoma]. Pathologe. German. 2014; 35: 467-75.
- NCCN guidelines version 1. Merkel cell carcinoma. 2023.
- Gauci ML, Aristei C, Becker JC, Blom A, Bataille V, et al, Diagnosis and treatment of Merkel cell carcinoma: European consensus-based interdisciplinary guideline - Update 2022. Eur J Cancer. 2022; 171: 203-231.
- D’Angelo SP, Russell J, Lebbé C, Chmielowski B, Gambichler T, et al. Efficacy and Safety of First-line Avelumab Treatment in Patients With Stage IV Metastatic Merkel Cell Carcinoma: A Preplanned Interim Analysis of a Clinical Trial. JAMA Oncol. 2018; 4: e180077.
- D’Angelo SP, Lebbé C, Mortier L, Brohl AS, Fazio N, et al. First-line avelumab in a cohort of 116 patients with metastatic Merkel cell carcinoma (JAVELIN Merkel 200): Primary and biomarker analyses of a phase II study. J Immunother Cancer. 2021; 9: e002646.
- Nghiem P, Bhatia S, Lipson EJ, Sharfman WH, Kudchadkar RR, et al. Durable Tumor Regression and Overall Survival in Patients With Advanced Merkel Cell Carcinoma Receiving Pembrolizumab as First-Line Therapy. J Clin Oncol. 2019; 37: 693-702.
- Topalian SL, Bhatia S, Hollebecque A, Awada A, De Boer JP, et al. Non-comparative, open-label, multiple cohort, phase 1/2 study to evaluate nivolumab (NIVO) in patients with virus-associated tumors (CheckMate 358): Efficacy and safety in Merkel cell carcinoma (MCC). Cancer Res. 2017; 77S: AACR #CT074.
- D’Angelo SP, Bhatia S, Brohl AS, Hamid O, Mehnert JM, et al. Avelumab in patients with previously treated metastatic Merkel cell carcinoma: long-term data and biomarker analyses from the single-arm phase 2 JAVELIN Merkel 200 trial. J Immunother Cancer. 2020; 8: e000674.
- D’Angelo SP, Bhatia S, Brohl AS, Hamid O, Mehnert JM, et al. Avelumab in patients with previously treated metastatic Merkel cell carcinoma (JAVELIN Merkel 200): Updated overall survival data after >5 years of follow-up. ESMO Open. 2021; 6: 100290.
- Grignani G, Rutkowski P, Lebbe C. 545 a phase 2 study of retifanlimab in patients with advanced or metastatic merkel cell carcinoma (MCC) (POD1UM-201). J Immunother Cancer 2021; 9: 2S.
- Pichler M, Steyrer J. Cost-effectiveness analysis of the use of immunotherapy in metastatic solid tumours in Austria by applying the ESMO-Magnitude of Clinical Benefit Scale (ESMO-MCBS) version 1.1. ESMO Open. 2021; 6: 100198.
- Everest L, Shah M, Chan KKW. Comparison of Long-term Survival Benefits in Trials of Immune Checkpoint Inhibitor vs NonImmune Checkpoint Inhibitor Anticancer Agents Using ASCO Value Framework and ESMO Magnitude of Clinical Benefit Scale. JAMA Netw Open. 2019; 2: e196803.
- Rakshit S, Molina JR. Immunotherapy in patients with autoimmune disease. J Thorac Dis. 2020; 12: 7032-7038.
- Nghiem P, Kaufman HL, Bharmal M, Mahnke L, Phatak H, et al. Systematic literature review of efficacy, safety and tolerability outcomes of chemotherapy regimens in patients with metastatic Merkel cell carcinoma. Future Oncol. 2017; 13: 1263-1279.
- Voog E, Biron P, Martin JP, Blay JY. Chemotherapy for patients with locally advanced or metastatic Merkel cell carcinoma. Cancer. 1999; 85: 2589-95.
- Tai PT, Yu E, Winquist E, Hammond A, Stitt L, et al. Chemotherapy in neuroendocrine/Merkel cell carcinoma of the skin: case series and review of 204 cases. J Clin Oncol. 2000; 18: 2493-9.
- Iyer JG, Blom A, Doumani R, Lewis C, Tarabadkar ES, et al. Response rates and durability of chemotherapy among 62 patients with metastatic Merkel cell carcinoma. Cancer Med. 2016; 5: 2294-301.
- Satpute S, Ammakkanavar NR, Einhorn LH. Role of platinum-based chemotherapy for Merkel cell tumor in adjuvant and metastatic settings. J Clin Oncol. 2014; 32: 9049-9049.
- Leão I, Marinho J, Costa T. Long-term response to avelumab and management of oligoprogression in Merkel cell carcinoma: A case report. World J Clin Cases. 2021; 9: 4829-4836.
- Torchio M, Cattaneo L, Milione M, Prinzi N, Corti F, et al. Case Report: Exceptional Response to Avelumab After Failure of Electrochemotherapy in a Patient With Rapidly Progressive, PD-L1-Negative Merkel Cell Carcinoma. Front Oncol. 2021; 11: 628324
