
Open Access, Volume 9
Spontaneous haemopneumothorax: A rare illness with unusual presentation and aetiology
Mohamed Hussein El Damasy*; Arshad Ali Khan; Ahmed Ba-Dheeb; Mootaz El Shaigi
Basildon University Hospital, Mid and South Essex NHS Foundation Trust, Nether Mayne, Basildon, Essex, United Kingdom.
Mohamed Hussein El Damasy
Basildon University Hospital, Mid and South Essex NHS Foundation Trust, Nether Mayne, Basildon, Essex,
United Kingdom.
Phone: +44 7399498696;
Email: Mohamed.hussein2@nhs.net
Received : June 22, 2023,
Accepted : Sep 15, 2023
Published : Sep 22, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: In the acute context, spontaneous haemopneumothorax is a life-threatening condition that can occur without any radiological abnormalities and may be caused by thoracic vascular aberrancy.
Case presentation: We discuss the case of a healthy 24-year-old man who visited our emergency department complaining of left sided chest pain and shortness of breath. He had previously visited a tertiary care facility’s emergency department for the same complaint the same day and had been released following a normal CXR and blood tests. His repeat x-ray chest revealed hemopneumothorax in our department. His CT scan further revealed ruptured aberrant blood vessel which was medial to the left subclavian artery.
Conclusion: This example illustrates the importance of maintaining a high index of suspicion when evaluating patients who present with chest pain and shortness of breath. There must be a repeat patient examination and x-ray chest for patients who experience prolonged chest discomfort, despite normal first investigations. If the patient’s repeat x-ray’s indicate hemopneumothorax, this should leave one to ponder the likelihood that thoracic bleeding could result from vascular aberrancy as a cause.
Keywords: Chest pain; Spontaneous haemopneumothorax; Case report; Thoracotomy and Chest X-ray.
Abbreviations: ED: Emergency department; CXR: chest x-ray; CT: Computed tomography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © El Damasy MH (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: El Damasy MH, Ali Khan A, Ba-Dheeb A, El Shaigi M. Spontaneous haemopneumothorax: A rare illness with unusual presentation and aetiology. Open J Clin Med Case Rep. 2023; 2115.
Introduction
Uncommon but possibly fatal, spontaneous haemopneumothorax needs to be identified an treated right away. It is mostly seen in 3% of patients with spontaneous pneumothorax [1] and is characterised by air and blood in the pleural space, which can lead to breathing difficulties, chest pain, and hemodynamic instability. While underlying lung illness or adhesion tears in spontaneous pneumothorax are assumed to be the causes of spontaneous haemopneumothorax, vascular aberrancy is a rather uncommon cause [2]. In this case study, we discuss a patient who, despite initially normal radiography, presented to our emergency room complaining of left sided chest pain and shortness of breath and was later found to have a spontaneous haemopneumothorax
Case Presentation
The emergency department (ED) of a tertiary care hospital received a visit from a 24-year-old man with back and left sided chest pain at around 9:00 AM. Shortness of breath and moderate to severe pain that suddenly began at rest are also present. He had undergone a CXR and blood tests to look for signs of pneumothorax. Once his x-ray and blood tests reported normal, he was discharged on oral analgesia.
Throughout the day, his suffering worsened. This led him to visit his local GP who advised him to take analgesia and was discharged. By evening, he was increasingly breathless and restless, which led to then call the emergency services. Initial examinations by the EMS personnel revealed he was found to be tachypneic, tachycardic, and was hypotensive, however, the oxygen saturation was 91%. When he was first assessed upon being led to our ED, he appeared frightened, tachypneic, and was in pain. Upon doing a chest auscultation, it was discovered that the right chest had good air entry whereas the left had none, as well as stony dullness on the left base and resonance to percussion of the left upper lung. A chest x-ray was performed following the administration of analgesia (Figure 1), and the results of a VBG showed (pH 7.29, PCO2 7.45, PO2 2.01, CHCO3 26.3, Lactate 3.2 mmol/L, and HB 127 g/L).
On the guidance of the cardiothoracic specialists, a chest tube was placed, which drained 950 ml of fresh blood using the Seldinger procedure, and then clamped. We administered IV fluids and PRBCs were given. It was decided to perform a chest CT scan with contrast (Figure 2). Following a surgical examination, the chest tube was unclamped, which immediately caused a 700 ml of blood loss. Vital signs of the patient remained stable.
A new VBG was obtained following the infusion of 2 litres of crystalloids and showed the following values: pH 7.30, PCO2 7.17, PO2 6.66, CHCO3 26.0, lactate 2.3 mmol/L, and HB 107 g/L. The chest tube was then unclamped, allowing for the retrieval of an additional 600 mls of blood, for a total drainage of 2.2 L, before the patient was transferred to our cardiothoracic ITU for preoperative evaluation and stabilisation.
The patient was transferred to the operative theatre and the left postero-lateral thoracotomy was performed in the fifth intercostal space. A small aberrant artery medial to the left subclavian wasactively bleeding, got clipped and stitched. The patient recovered well from surgery and the chest drain was removed following satisfactory chest x-ray.
Discussion
It is possible to define hemopneumothorax as the buildup of more than 400 ml of blood in the thoracic cage in the presence of spontaneous pneumothorax, where a tear in an adhesion would cause bleeding; however, there haven’t been any consistent intraoperative findings, which might call for a review study [3]. Whittaker successfully treated the illness for the first time by repeatedly aspirating pleural space in 1876, over a century after Laennec initially identified it during an autopsy [4]. Nearly 33% of individuals with the condition—who are mostly young men—present with hypovolemic shock. 87.6%, of patients require surgical intervention, with blood loss ranging from 400 to 1700 mls according to one research [3]. With good outcomes and few recurrences, surgical intervention using an open thoracotomy and video-assisted thorcoscopy was carried out. The core component of conservative management was tube thoracotomy .
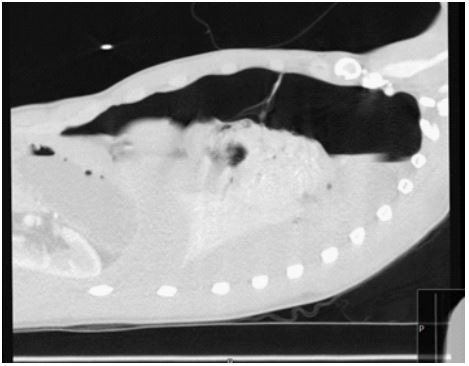
Figure 1: An expiratory view showing totally collapsed left
lung with fluid level indicating haemothorax
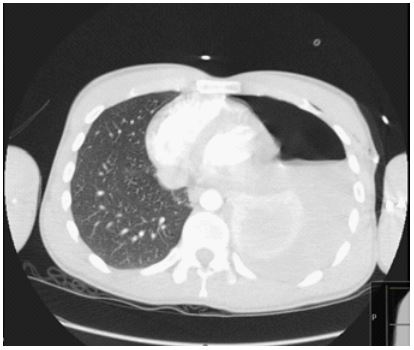
Figure 2: CT scan of the chest revealing the left sided airfluid level of the haemopneumothorax with the collapsed
left lung
A spontaneous pneumothorax that results in an abrupt start of chest discomfort and shortness of breath is the traditional course of events. However, occasionally pneumothorax can lead to the rupture of an aberrant blood vessel, resulting in hemopneumothorax. Although this was the case in our patient, proper management was delayed since his anomaly wasn’t seen on the initial chest imaging, which is rather uncommon. Looking back, a chest CT scan performed early on would have allowed for a more accurate diagnosis, especially if the patient had been experiencing prolonged, unrelieved chest pain and shortness of breath. We would strongly advise patients with persistent acute chest pain to do repeat examination and x-rays of the chest because measuring pneumothorax in the early stages does not present a diagnostic conundrum. This is because a chest x-ray interpretation in the early stages presents diagnostic challenges.
When evaluating patients with spontaneous haemopneumothorax, we must keep in mind that aberrant bleeding blood vessels is a rare etiology. In the absence of the tamponade effect of an inflated lung, a small blood vessel that is bleeding continuously would shock the patient [5]. Because of this, we would advise aggressive resuscitation as well as seeking early specialist advice and referral for definitive management from the acute setting.
Conclusion
According to the case study and discussion, hemopneumothorax is a rare condition that can cause hypovolemic shock. Although a chest X-ray is the preferred initial investigation, patients with persistent acute chest pain should be given the option of a chest CT scan to ensure proper diagnosis [6], particularly where it is not readily apparent on the initial chest imaging. The majority of patients continue to receive their care primarily through surgical intervention, with conservative management typically limited to tube thoracostomy. Rarely, aberrant bleeding blood vessels can cause haemopneumothorax; therefore, in the acute setting, it is important to seek early specialist guidance and referral for effective care. In general, haemopneumothorax patient outcomes can be considerably improved with prompt and effective care.
Declarations
Conflict of interest: The authors declare no conflict of interest regarding the publication of the article.;
Funding: Nil.
Consent for publication: A written consent for publication was taken from the patient.
Ethical approval: Is not requested in our institution to submit anonymous case report for publication.
References
- Catherine Wegner Wippel, Sasckia Duarte, Caroline Blum, Eduardo Ballister. Spontaneous haemopneumothorax resulting in shock. Chest Journal. 2021; 4: 160.
- Yoshihiko Kurimoto, Keisuke Hatamoto, Mamoru Hase, Eichi Narimatsu, Yasufumi Asai, Tomio Abe. Aberrant artery as a source of bleeding in spontaneous heamopneumothorax. The American Journal of Emergency Medicine. 2001; 19: 326- 327.
- Nan-Yung Hsu, Chih-Shiun Shih, Chung-Ping Hsu, Ping-Ru Chen. Spontaneous haemopneumothorax revisited: clinical approach and systematic review of the literature. The annals of thoracic surgery. 2005; 80: 1859-1863.
- Wen-Chu Chiang, Wen-Jone Chen, Kuang-Jui Chang, Ting-I Lai, Ang Yuan. Spontaneous hemopneumothorax: an overlooked life-threatening condition. The American Journal of Emergency Medicine. 2003; 21: 343-345.
- Davide Patrini, Nikolaos Panagiotopoulos, Jonathan Pararajasingham, Lasha Gvinianidze, Yassir Iqbal, et al. Lawrence. Journal of thoracic disease. 2015; 7: 520- 526.
- Sebastiaan Hammer, Lucia J Kroft, Alberto L Hidalgo, Ruben Leta, Albert de Roos. Chest CT examinations in patients presenting with acute chest pain: a pictorial review. Insights into Imaging. 2015; 6: 719-728.
