
Open Access, Volume 9
A case report of Eagle’s syndrome: The union of the styloid process and the hyoid bone
Ewelina Beck1; Maria Tekieli-Pawłowska2; Paweł Święch2; Witold Matusiak2; Przemysław Jaźwiec2*
1Faculty of Medicine, Wroclaw Medical University, Poland.
2Specialist Medical Center in Polanica-Zdrój, Jana Pawła II 2, 57-320 Polanica Zdrój, Poland.
Przemysław Jaźwiec
Specialist Medical Center in Polanica-Zdrój, Jana Pawła II 2, 57-320 Polanica Zdrój, Poland.
Email: przemkolog@wp.pl
Received : July 20, 2023,
Accepted : Sep 12, 2023
Published : Sep 15, 2023,
Archived : www.jclinmedcasereports.com
Abstract
The Eagle’s Syndrome is a rare condition found in 4% of the general population. It is caused by elongation of the styloid process and/or calcification of the stylohyoid ligament. Clinical image depends on, which structures, including nerves, blood vessels, soft tissues, have been compressed by the styloid process. Symptoms include otopharyngeal, neurological and vascular manifestations. The diagnosis of the Eagle’s syndrome might be incidental in asymptomatic patients as well. The authors present a case of a patient with the Eagle’s Syndrome, who has suffered from undefined throat discomfort for 6 years. Computed tomography (CT) showed an excessively elongated styloid process reaching the hyoid bone to contribute to a newly formed joint. This opened the pathway for further diagnostics and treatment but, most importantly, solving patient’s health problem, bothering her for many years.
Keywords: Eagle’s syndrome; Styloid process; Stylohyoid ligament; Hyoid bone; Computed tomography; Volumetric reconstructions (3D-VR)
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Jaźwiec P (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Beck E, Tekieli-Pawłowska M, Święch P, Matusiak W, Jaźwiec P. A case report of Eagle’s syndrome: The union of the styloid process and the hyoid bone. Open J Clin Med Case Rep. 2023; 2113.
Introduction
Eagle’s syndrome is a set of clinical symptoms caused by an elongated styloid process or a calcified stylohyoid ligament, first described and named after American otolaryngologist Watt Weems Eagle (1898–1980) in 1937. Interestingly, the pathoetiology of the syndrome remains unclear in the majority of cases. In some instances, it has been associated with tonsilectomy, direct trauma, wisdom tooth removal and in some it has been an incidental finding in CT of the head and neck. Some authors suggest heterotopic calcification in patients with unbalanced calcium-phosphorus metabolism and chronic renal failure as the cause. It is a rare condition, present in 4% of the general population and symptomatic only in 4% of these. Due to it’s small prevelance, anatomical variability and versetile clinical manifestations, Eagle’s Syndrome poses a real medical treat and a diagnostic challange to for a physician [2,6].
Case Presentation
The patient was a 39-year-old female, who initially reported to an otolarygologist because of undefinied discomfort in the throat for 6 years. Other complaints included a stabbing sensation in the neck, a feeling of the congested ear as well as tinnitus, otalgia, excessive salivation.
On physical examination, head movements and opening the mouth caused pain. No neurological deficits or symptoms present except parestesia around the left check, ear and medial 1/3 of the neck. The patient denied odynophagia, dysphagia, vision disturbances, headaches or voice change. Currently, she does not report other complaints.
In the medical history, the patient was diagnosed with arterial hypertension in 2010 and since then she has been put on captopril. In the past she suffered cervical lymphadenitis. Apart from these, the patient has no history of past or chronic diseases and has never undergone any surgical procedures.
Computed tomography of the neck without contrast administration showed bilateral elongated styloid processes. On the left side the overal lenght of the styloid process was 8,3 cm. Aditionally within the left styloid process we observed two false joints, one of them in the down part, reposition the hyoid bone in caudal direction (Figure 3). Maximum width of the left styloid process was 1,3 cm and it was located at the level of upper false joint. Right styloid process was elongated insignificantly (3,65 cm) and didn’t cause pain or any other symptoms.
The patient was reffered to the University Clinical Hospital in Wroclaw for further diagnostics and treatment.
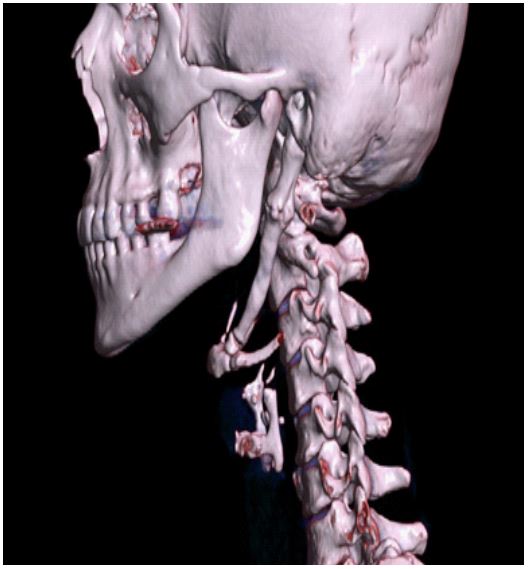
Figure 1: Multidetector computer tomography (MDTC)
with 3D volumetric reconstructions (3D-VR) - left-sided
sagittal view.

Figure 2: Multidetector computer tomography (MDTC)
with multi-planar reconstructions (MPR) - left-sided sagittal view. Measurement of the overall length of left styloid process.
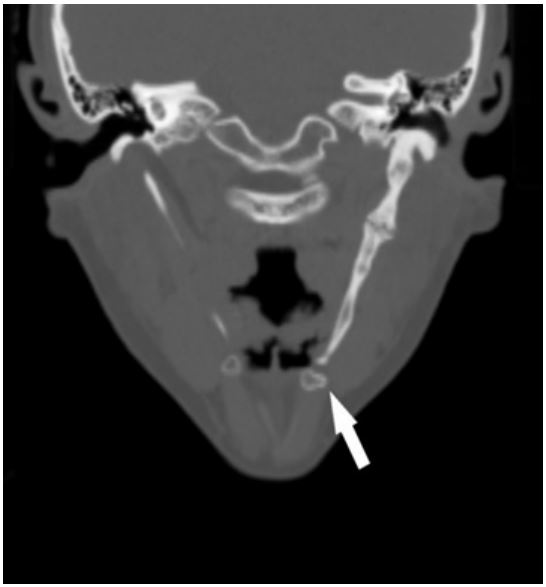
Figure 3: Multidetector computer tomography (MDTC)
with multi-planar reconstructions (MPR) - coronal view.
Reposition the hyoid bone in caudal direction.

Figure 4: Multidetector computer tomography (MDTC)
with multi-planar reconstructions (MPR) - left-sided sagittal view. Measurements of the width of left styloid process.
Discussion
The styloid process is a needle-like bony structure protruding anteroinferiorly from the inferior surface of the temporal bone and towards the hyoid bone. On average its length ranges from 2,5 cm to 3,0 cm. When it exceeds 3,0 cm, it is considered elongated. The hyoid bone is a u-shaped bone located in the anterior neck, at the base of the mandible. These two stuctures are connected by stylohyoid ligament and both contribute to the unit called the styloid apparatus, along with associated ligaments and muscles. Anatomiacally they do not make a direct connection with each other. However, the presented case shows a different situation, in which an excessively long styloid process reaches the hyoid and these two form a joint. Altered anatomical relations of the regional structures led to the symptomatic manifestation of Eagle’s syndrome in the patient [1-3,12].
Depending on the clinical presentation, there are two types of the Eagle’s syndrome: classic Eagle syndrome – due to compression of the cranial nerves V, VII, VIII, IX, or X, - and vascular Eagle syndrome – due to compression of the internal or external carotid artery. The first one is typically characterized by facial/cervical pain exacerbated by the head movement, otalgia, dysphagia, odynophagia, foreign body sensation, headache, tinnitus. On the other hand, the latter manifests as carotidynia, as a result of sympathetic plexus irritation, or ischemic symptoms such as visual disturbance, syncope, aphasia. In extreme cases, TIA, ischemic stroke or carotid dissection might occur [1,2,6-11].
Eagle’s syndrome might be challenging to diagnose beacause of its nondistinctive clinical image. While managing a patient with head and neck symptoms, physician should firstly consider other possible differential diagnoses, primarily facial neuralgia, malignancy and temporomandibular joint disorder. The diagnosis is usually suggested on the basis of patient’s medical history and physical examination, as an elongated styloid process may be palpable. The classical X-ray enables measuring the process’s length. It is accepted that the best method to visualize the styloid process, its angulation and anatomical relation with nearby structures is multiple row CT with 3D recontruction. This method appears to be sufficient enough not only to make the final diagnosis but also plan further treatment. Thus, it is considered the gold standard [1,2,5].
Treatment includes both conservative and surgical methods. To reduce pain, patients are put on analgesics, antidepressants, anticonvulsants as well as transpharyngeal injections of steroids, lidocaine, NSAID can be applied. If a patient does not respond to conservative treatment, they may be suited for a surgical styloidectomy. There are two approaches of the procedure – intraoral and external. According to some authors, the success rate of the surgery is 80% [2,4,6].
Conclusion
The Eagle’s Syndrome is a rare condition found in 4% of the general population. Its manifestation might be asymptomatic or symptomatic with various clinical image. Usually, patients seek for medical help beacause of nonspecific symptoms such as the feeling of a foreign body in the throat, dysphagia, pain localized in the temporomandibular region, neck and ear, bothering them for years before the initial diagnosis is put forward. Physicians of different specialties are often involved in the diagnostic process, especially laryngologists and neurologists. Imaging techniques are essential to second the initial diagnosis, make the final one and plan further treatment. Multiple row CT and 3D reconstruction have been accepted as the gold standard.
References
- Wolińska I, Jaźwiec P, Pawłowska M, Gać P, Poręba R, et al. Eagle’s Syndrome as aCause of Discomfort and theSubjective Presence of a Foreign Body in the Throat. Diagnostics 2021; 11: 1832.
- Bokhari MR, Graham C, Mohseni M. Eagle Syndrome. In: StatPearls. Treasure Island (FL). 2023.
- Abuhaimed AK, Alvarez R, Menezes RG. Anatomy, Head and Neck, Styloid Process. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2023.
- Jain S, Bansal A, Paul S, Prashar DV. Styloid-stylohyoid syndrome. Ann Maxillofac Surg. 2012; 2: 66-9.
- Saccomanno S, Greco F, DE Corso E, Lucidi D, Deli R, et al. Eagle’s Syndrome, from clinical presentation to diagnosis and surgical treatment: a case report. Acta Otorhinolaryngol Ital. 2018; 38: 166-169.
- Singh G, Gaillard F, Baba Y, et al. Eagle syndrome. Reference article, Radiopaedia.org. 2023.
- Ceylan A, Köybaşioğlu A, Celenk F, Yilmaz O, Uslu S. Surgical treatment of elongated styloid process: Experience of 61 cases. Skull Base. 2008; 18: 289-95.
- Murtagh RD, Caracciolo JT, Fernandez G. CT findings associated with Eagle syndrome. AJNR Am J Neuroradiol. 2001; 22: 1401-2.
- Lorman JG, Biggs JR. The Eagle syndrome. AJR Am J Roentgenol. 1983; 140: 881-2.
- Chuang WC, Short JH, McKinney AM, Anker L, Knoll B, et al. Reversible left hemispheric ischemia secondary to carotid compression in Eagle syndrome: surgical and CT angiographic correlation. AJNR Am J Neuroradiol. 2007; 28: 143-5.
- Faivre A, Abdelfettah Z, Rodriguez S, Nicoli F. Neurological picture. Bilateral internal carotid artery dissection due to elongated styloid processes and shaking dancing. J Neurol Neurosurg Psychiatry. 2009; 80: 1154-5.
- Gray’s anatomy: The anatomical basis of clinical practice. Susan Standring (Forty-second ed.). [New York]. 2021; 737.
