
Open Access, Volume 9
False positive PET-CT imaging after application of fibrin-based sponge at the site of previous hepatic resection for colo-rectal metastasis: A short series
Steven Grandjean1; Claude Bertrand1; Bruno Krug2; Alexandra Dili1*
1Department of General, Digestive and Endocrine Surgery, Pole of hepato-bilio-pancreatic surgery, CHU UCL Namur, Site of Godinne, Belgium.
2Department of Nuclear Medicine, CHU UCL Namur, Site of Godinne, Belgium.
Alexandra Dili
Department of General, Digestive and Endocrine Surgery Avenue du Dr Gaston Thérasse, 15530 YVOIR
Belgium.
Phone: (+32)81/423085 & (+32)479849517; Email: alexandra.dili@chuuclnamur.uclouvain.be
Received : July 22, 2023,
Accepted : Sep 11, 2023
Published : Sep 15, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Surgical resection is the treatment of choice with curative intent for colorectal liver metastasis. Preoperative accurate radiological staging is key for optimal treatment. Fluorine-18 fluorodeoxyglucose PET-CT (PETCT) is effective for this purpose.
We present 4 cases of patients with history of hepatectomy for colorectal liver metastasis. In all patients, during the procedure, we used fibrin-based sponge to achieve optimal haemostasis of the parenchymal transection surface. During the oncologic follow-up, a suspicion of disease recurrence justified a staging PET-CT that revealed pathologic metabolic activity on sites of previous liver resection, highly suspicious of tumour recurrence. The delay between hepatectomy and PET-CT for recurrence ranged from 5 to 12 months. In all cases, a new surgical exploration was performed after neoadjuvant chemotherapy, and PET-CT positive sites of previous liver resection were removed. Definitive histological diagnosis showed inflammatory granuloma or fibrous tissue.
Based on this experience, we suggest that PET-CT abnormal metabolic activity at previous hepatectomy sites should be treated with caution to avoid futile liver resection. Chronic inflammatory response after application of fibrin-based-sponge could explain false-positive PET-CT imaging.
Keywords: Liver metastasis; PET-CT; Granuloma; Haemostatic sponge.
Abbreviations: ET-CT: Fluorine-18 fluorodeoxyglucose positron emission tomography and computed tomography; CRLM: Colorectal liver metastases; CT: Computed tomography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Dili A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Grandjean S, Bertrand C, Krug B, Dili A. False positive PET-CT imaging after application of fibrin-based sponge at the site of previous hepatic resection for colo-rectal metastasis: A short series. Open J Clin Med Case Rep. 2023; 2112.
Introduction
Colorectal cancer is the third most common cancer in the world [1]. Approximatively, 15-30% of patients present synchronous liver metastasis, while 20-50% of patients will develop metachronous disease, with a most common location in the liver [2]. Considering that the R0 resection of colorectal liver metastases (CRLM) is a potentially curative treatment with reported 5-year-survival rates of 20-45%, an accurate pre-operative staging is of paramount importance.
Among the different staging modalities of hepatic and extra-hepatic disease, 18F-fluorodeoxyglucose positron emitted tomography and computed tomography (PET-CT) has emerged as an additional tool alongside ultrasonography, computed-tomography (CT) and magnetic resonance to detect intra- or extrahepatic metastasis.
For the liver, PET-CT identifies abnormal tissue metabolic activity, which may precede imaging alterations [3]. Most importantly, PET-CT may have an advantage over standard imaging to detect recurrent liver disease after liver resection, local ablation, or radioembolization. Indeed, in this context, parenchymal lesions observed in CT or US may correspond in sequelae of the treatment and not recurrent tumour. A recent systematic review on PET-CT in treatment evaluation of CRLM concluded that PET-CT is superior to other modalities after thermal ablation, in case of palliative chemotherapy and after radioembolization [4]. After surgery, a systematic review underlines the benefit of PET-CT in the detection of extrahepatic lesions in patients operated for CRLM. As such, the recent European guidelines consider this modality to be useful in case of increased tumour markers without evidence of metastatic disease and to evaluate the metastatic extension of the disease on potentially resectable metastases [2].
Liver surgery is key for the treatment of CRLM, but still carries some risk of morbidity mostly linked to bleeding, bile leakage and abscess formation [5]. Advances in pre-operative management, extensive knowledge of liver anatomy, more dedicated surgical techniques and postoperative care have made liver resection safer over the years, expanding the resection criteria and the extent of hepatectomy. Actually, numerous topical agents have been proposed in the past decades to treat the parenchymal sections [6]. These products include fibrin-based glue or patches, gelatin- or collagen-based products and oxidised cellulose. These tools may be effective in reducing time to haemostasis but do not to reduce transfusion, post-operative collection and bile leak [7-9].
In our institution, in addition of surgical clips we often use Tachosil®, a dry collagen sponge coated with fibrinogen and thrombin to achieve haemostasis, when needed, on liver sections. Here, we report a short series of PET-CT false-positive metabolic activity at liver transection sites after application of haemostatic sponges.
Case Series
All the following patients have undergone at least one radical liver resection (R0) for colorectal metastasis, with haemostasis achieved using fibrinogen sponge material and surgical clips
Patient 1
A 70-year-old male patient was diagnosed with rectal cancer with two synchronous liver metastasis in segments III and VIII measuring 12 and 35 mm, respectively.
After neoadjuvant treatment, a wedge resection of the tumour in segment III and a large wedge resection in segment VIII were performed laparoscopically, followed by adjuvant chemotherapy
Eleven months later, a metachronous metastasis was detected on CT-scan (segment VI), while stigmata of resection around segment VIII persisted. The subsequent PET-CT excluded extra-hepatic disease and revealed not only a pathologic metabolic activity in segment VI (SUV 7,5) but also in segment VIII at the site of previous liver resection (SUV 8,3) (Figure 1A).
After second line neoadjuvant chemotherapy, a control PET-CT identified a complete metabolic response of the tumour in segment VI, and partial response (SUV 3,9) in segment VIII (Figure 1B)
A redo hepatectomy was performed with a wedge resection of segment VI and segmentectomy of segment VIII with skeletisation of the right hepatic vein.
Analysis of the specimens revealed a metastasis of colorectal origin in the specimen of segment VI, however showed signs of inflammatory granuloma at the site of resection of segment VIII.
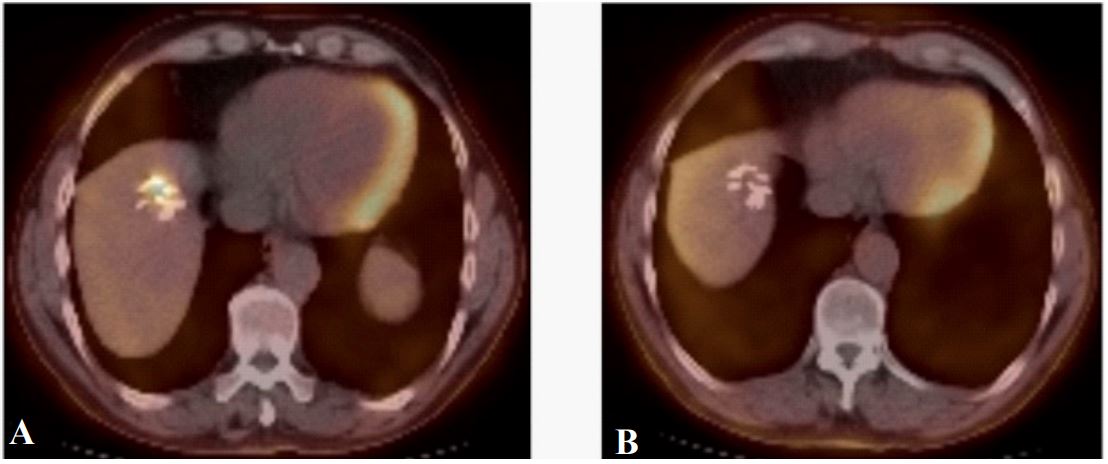
Figure 1: Representative images of PET-CT metabolic activity in the site of previous wedge resection on segment
VIII (A) at diagnosis (SUV 8,3) (B) after neoadjuvant therapy (SUV 3,9)
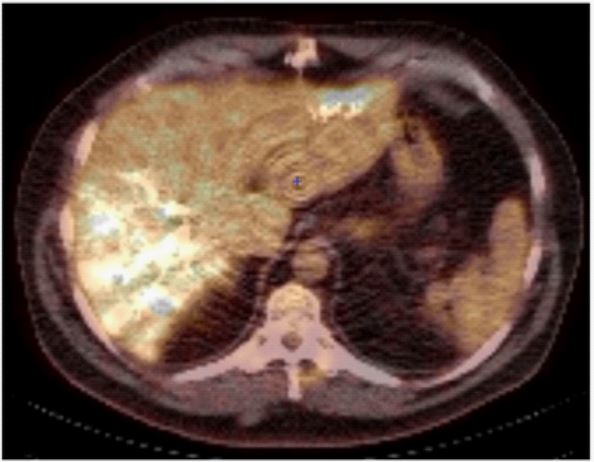
Figure 2: Representative images of PET-CT metabolic
activity in the site of previous wedge resection on segment II (SUV 4,8)
Patient 2
A 53-year-old male patient was diagnosed with an occlusive sigmoid colic cancer with synchronous multiple bilobar liver metastasis. Firstly, an anterior rectal resection was performed combined to a complete tumour clearance of the left hemiliver, by resection of five metastasis. He received systemic chemotherapy, and right portal embolization before second step right hepatectomy. PET-CT performed five months after the first step resection and prior to the second stage hepatectomy showed abnormal metabolic activity in segments V and VI, as long as in the resection site of segment II (SUV 4,8) (Figure 2). During the right hepatectomy, the former section site of segment II was removed, and histopathology showed features of fibrous scar tissue with no evidence of malignancy.
Patient 3
A 56-year-old man was diagnosed with sigmoid colon cancer with initially borderline resectable synchronous liver metastasis. After neoadjuvant chemotherapy with partial response, he underwent an emergency left colectomy for colic occlusion, followed one month later by liver tumour clearance through multiple wedge resections of segments IV, VIII and VII. Eighteen months later, a repeat hepatectomy for recurrence was performed on segment IV combined to lung metastasectomy
CT-imaging eleven months later detected lymph node disease in the hepatic hilum, while PET confirmed an abnormal metabolism in the hilar lymph node and in the liver parenchymal section of previous segment IV resection (SUV 6,9) (Figure 3). After second line chemotherapy, a new surgical exploration was performed with lymph node clearance. Intraoperative liver ultrasound detected no lesions in the segment IV section and the biopsy performed at this site showed fibroadipose tissue without histological abnormalities., while lymph node disease recurrence was confirmed.
Patient 4
A 66-year-old male patient suffering of occlusive left colic adenocarcinoma with two synchronous hepatic metastases had a left colectomy, followed by chemotherapy and segment II and VII wedge resections.
Nine months after liver resection, CT-imaging revealed an increase in the size of left para-aortic lymph nodes, while PET-CT confirmed pathologic para-aortic lymph node disease and hypermetabolism at the resection site in segment VII (SUV 4,9) (Figure 4).
After a second line induction chemotherapy, surgical exploration with intraoperative liver ultrasound was performed, with resection of a segment VII, and extended lymphadenectomy. Pathology of segment VII found a necrotic lesion, containing staples, surrounded by fibro-inflammatory tissues and granulomas, while lymphadenectomy specimens confirmed metastatic disease.
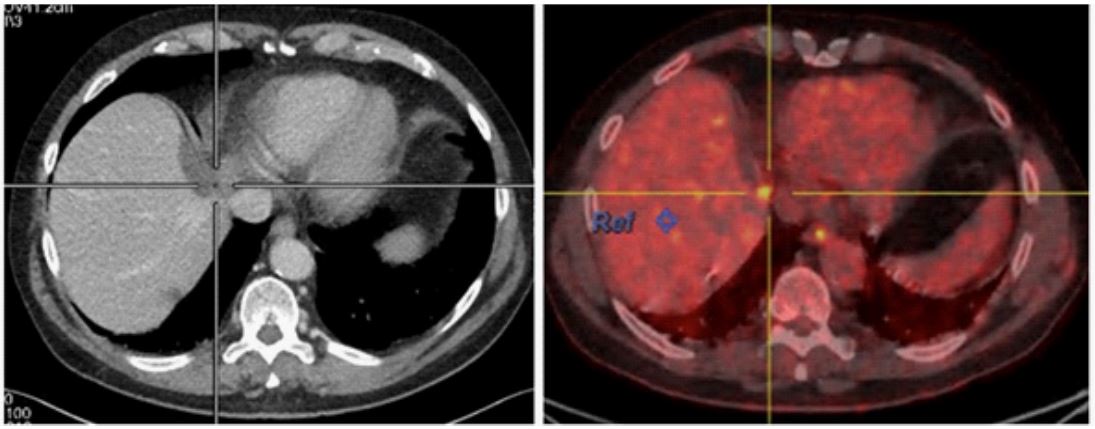
Figure 3: Representative images of PET-CT metabolic activity in the site of previous wedge resection on segment
IV (SUV 6,9)
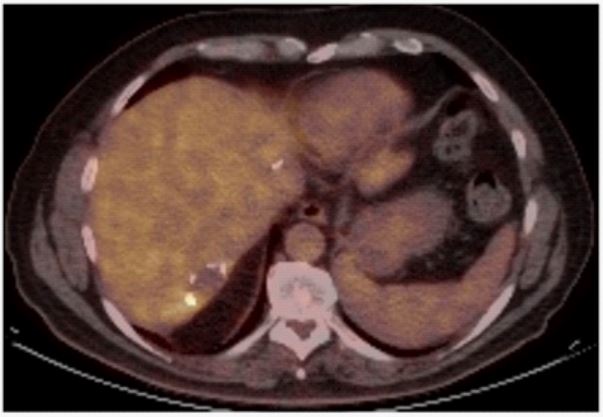
Figure 4: Representative images of PET-CT metabolic activity in the site of previous wedge resection on segment VII
(SUV 4,9)
Discussion
Despite the ability of 18F-fluorodeoxyglucose PET-CT to distinguish between malignant and benign disease, fluorodeoxyglucose (FDG) is not a cancer-specific agent and various causes of false positive benign lesions have been reported [10]. Indeed, FDG is an analogue of glucose that accumulates in cancer but also in inflammatory cells (lymphocytes, neutrophils and macrophages) present in inflammation or infections, in active granulomatous processes and active fibrotic lesions [11]. Tan et al [12] reviewed a series of 1427 PET-CT studies with metabolically active liver lesions, with definitive histology available on 214 cases. 91% of these were malignant, 5,1% remained undetermined and 3,7% were proven to be benign. They identified hepatic abscess, cryptococcal infection, hepatic adenoma and haemangioendothelioma as non-malignant conditions of PET-CT positivity in the liver. They also highlighted that extrahepatic lesions such as adrenal tumours or gallbladder carcinoma, infection or inflammation can mimic liver positive neoplasm.
Table 1: Clinical parameters of the 4 cases with false positive PETscan on previous hepatic resection’s sites.
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | |
|---|---|---|---|---|
| Age at incidence | 70 | 53 | 56 | 66 |
| Sex | M | M | M | M |
| Initial resection site | III, VIII | II, III | IV, VIII | II, VIII |
| Resection status of primary hepatic resection | R0 (7 mm) | R0 | R0 (11 mm) | R0 (3 mm) |
| Time from primary hepatic resection to pathologic PET-CT (months) | 11 | 5 | 12 | 9 |
| Time from end of adjuvant therapy to pathologic PET-CT (months) | 7 | 1 | 8 | Ongoing |
| Site of suspected section site recurrence | VIII | II | IV | VII |
| SUV of suspected recurrence | 8,3 | 4,8 | 6,9 | 4,9 |
| Resection of suspected recurrence | Yes | Yes | Yes | Yes |
| Histologic findings | Inflammatory granuloma | Fibrous scar tissue | Fibroadipose tissue | Necrosis, staples, fibro- inflammatory tissues and granulomas. |
Other authors reported cases of false-positive hepatic lesions on PET-CT with hypermetabolic multifocal steatohepatitis [13], after an iatrogenic parenchymal liver injury or with radiation-induced liver injury [14].
In the literature, two cases of false-positive hepatic lesion on PET-CT on previous resection site have been reported, with histology revealing foreign body granuloma. While in the first case silk suture was identified on analysis [15], no specific foreign body was incriminated in the second [16]. Similarly, another team reported a case of foreign body granuloma on a liver resection site, suspected of malignancy by Gadolinium-DTA MRI [17].
Involvement of nonabsorbable surgical material in false-positive lesions on PET-CT has been reported in other types of surgery such as talc pleurodesis [18,19], colic anastomosis with silk or nonabsorbable suture [20], thyroidectomy [21], pulmonary resection [22], head and neck cancer surgery [23], orchidectomy [24], abdominal debulking [25], gastrectomy [26] and total hysterectomy [27].
Absorbable material has also been incriminated in cases of granuloma mimicking recurrence on PET-CT such as polyglycolic acid sheet and suture on pulmonary segmentectomy, surgical adhesive after lung cancer resection [28] or haemostatic compresses of fibrillar cellulose (Surgicel®) in intra-cerebral [29], cardiac [30] and gynaecologic surgeries [31].
In line with other haemostatic sponges, Tachosil®, a collagen-bound fibrin sealant, activates the coagulation cascade by imitating the final steps of the natural blood clotting system. The fibrin clot is then metabolized by fibrinolysis. Animal studies document the presence of fibrovascular granulation tissue with fibroblasts, neutrophils, lymphocytes and some giant cells as a sign of foreign body reaction [32]. To date, this device has never been documented in the development of postoperative granuloma in humans. However, there was one case of a post-operative granuloma mimicking a cervical spinal mass after the use of fibrin-based haemostat [33].
To our knowledge, we describe the first case series of false positive hepatic lesions on PET-CT following the use of fibrin-based sponge during initial liver surgery (Table 1). This phenomenon was observed even 12 months after the initial hepatectomy.
In conclusion, our findings suggest that PET-positive images at sites of R0 hepatic resection should be treated with caution, particularly when surgical material is left on parenchymal transection. Clinicians treating liver metastasis should be aware of possible false-PET-CT metabolic activity to avoid futile liver resections. In addition, the use of a specific haemostatic agents should be clearly mentioned on operative reports to help the differential diagnosis when a hypermetabolic lesion is detected during the oncologic follow-up.
Declarations
Funding information: No funding was received for this study.
Conflict of interest statement: None to declare.
Ethics statement: Ethical approval has been obtained for this study, in accordance with local guidelines.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71: 209-49.
- Cervantes A, Adam R, Roselló S, Arnold D, Normanno N, et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023; 34: 10-32.
- Georgakopoulos A, Pianou N, Kelekis N, Chatziioannou S. Impact of 18F-FDG PET/CT on therapeutic decisions in patients with colorectal cancer and liver metastases. Clin Imaging. 2013; 37: 536-41.
- Bijlstra OD, Boreel MME, van Mossel S, Burgmans MC, Kapiteijn EHW, et al. The Value of 18F-FDG-PET-CT Imaging in Treatment Evaluation of Colorectal Liver Metastases: A Systematic Review. Diagnostics (Basel). 2022; 12.
- Jin S. Management of post-hepatectomy complications. World J Gastroenterol. 2013; 19: 7983.
- de Boer MT, Boonstra EA, Lisman T, Porte RJ. Role of fibrin sealants in liver surgery. Dig Surg. 2012; 29: 54-61.
- Brustia R, Granger B, Scatton O. An update on topical haemostatic agents in liver surgery: systematic review and meta analysis. J Hepatobiliary Pancreat Sci. 2016; 23: 609-21.
- Wells CI, Ratnayake CBB, Mentor K, Sen G, Hammond JS, et al. Haemostatic Efficacy of Topical Agents During Liver Resection: A Network Meta-Analysis of Randomised Trials. World J Surg. 2020; 44: 3461-9.
- Ding H, Yuan JQ, Zhou JH, Zheng XY, Ye P, et al. Systematic review and meta-analysis of application of fibrin sealant after liver resection. Curr Med Res Opin. 2013; 29: 387-94.
- Chang JM, Lee HJ, Goo JM, Lee HY, Lee JJ, et al. False positive and false negative FDG-PET scans in various thoracic diseases. Korean J Radiol. 2006; 7: 57-69.
- Luk WH, Au-Yeung AWS, Loke TKL. Imaging patterns of liver uptakes on PET scan: pearls and pitfalls. Nucl Med Rev Cent East Eur. 2013; 16: 75-81.
- Tan GJS, Berlangieri SU, Lee ST, Scott AM. FDG PET/CT in the liver: lesions mimicking malignancies. Abdom Imaging. 2014; 39: 187-95.
- Duvivier A, Goyers JF, Radermacher J, Namur G. [Hypermetabolic multifocal steatohepatitis: A rare case of [18F] FDG PET/CT false positive mimicking a metastatic carcinomatosis]. Rev Med Liege. 2022; 77: 430-4.
- Voncken FEM, Aleman BMP, van Dieren JM, Grootscholten C, Lalezari F, et al. Radiation-induced liver injury mimicking liver metastases on FDG-PET-CT after chemoradiotherapy for esophageal cancer: A retrospective study and literature review. Strahlenther Onkol. 2018; 194: 156-63.
- Matsuura S, Sasaki K, Kawasaki H, Abe H, Nagai H, et al. Silk suture granuloma with false-positive findings on PET/CT accompanied by peritoneal metastasis after colon cancer surgery. Int J Surg Case Rep. 2016; 28: 22-5.
- Pantiora E v, Kontis EA, Michalaki V, Primetis E, Vezakis A, et al. Granuloma Mimicking Local Recurrence on PET/CT after Liver Resection of Colorectal Liver Metastasis: A Case Report. Cureus. 2016; 8: e717.
- Poyanli A, Bilge O, Kapran Y, Güven K. Case report: Foreign body granuloma mimicking liver metastasis. Br J Radiol. 2005; 78: 752-4.
- Ahmadzadehfar H, Palmedo H, Strunk H, Biersack HJ, Habibi E, et al. False positive 18F-FDG-PET/CT in a patient after talc pleurodesis. Lung Cancer. 2007; 58: 418–21.
- Fanggiday JC, Rouse RW, Collard SM, de Haas MJ, de Klerk JMH. Persistent Inflammation in Pulmonary Granuloma 48 Years after Talcage Pleurodesis, Detected by FDG-PET/CT. Case Rep Med. 2012; 2012: 686153.
- Lim JWM, Tang CL, Keng GHW. False positive F-18 fluorodeoxyglucose combined PET/CT scans from suture granuloma and chronic inflammation: report of two cases and review of literature. Ann Acad Med Singap. 2005; 34: 457-60.
- Chung YE, Kim EK, Kim MJ, Yun M, Hong SW. Suture granuloma mimicking recurrent thyroid carcinoma on ultrasonography. Yonsei Med J. 2006; 47: 748-51.
- Yüksel M, Akgül AG, Evman S, Batirel HF. Suture and stapler granulomas: a word of caution. Eur J Cardiothorac Surg. 2007; 31: 563-5.
- Kikuchi M, Nakamoto Y, Shinohara S, Fujiwara K, Tona Y, et al. Suture granuloma showing false-positive finding on PET/CT after head and neck cancer surgery. Auris Nasus Larynx. 2012; 39: 94-7.
- Takahara K, Kakinoki H, Ikoma S, Udo K, Tobu S, et al. Suture Granuloma Showing False-Positive Findings on FDG-PET. Case Rep Urol. 2013; 2013: 472642.
- Imperiale L, Marchetti C, Salerno L, Iadarola R, Bracchi C, et al. Nonabsorbable suture granuloma mimicking ovarian cancer recurrence at combined positron emission tomography/computed tomography evaluation: A case report. J Med Case Rep. 2014; 8: 202.
- Tsujita E, Ikeda Y, Kinjo N, Yamashita YI, Kumagai R, et al. Suture granuloma with false-positive finding on PET/CT after gastrectomy for gastric cancer. Asian J Endosc Surg. 2015; 8: 457-60.
- Takeshita N, Tohma T, Miyauchi H, Suzuki K, Nishimori T, et al. Suture Granuloma With False-Positive Findings on FDG-PET/CT Resected via Laparoscopic Surgery. Int Surg. 2015; 100: 604-7.
- Ruiz-Zafra J, Rodríguez-Fernández A, Sánchez-Palencia A, Cueto A. Surgical adhesive may cause false positives in integrated positron emission tomography and computed tomography after lung cancer resection. European Journal of Cardio-Thoracic Surgery. 2013; 43: 1251-3.
- Ito H, Onishi H, Shoin K, Nagatani H. Granuloma caused by oxidized cellulose following craniotomy. Acta Neurochir (Wien). 1989; 100: 70-3.
- Ibrahim MF, Aps C, Young CP. A foreign body reaction to Surgicel mimicking an abscess following cardiac surgery. Eur J Cardiothorac Surg. 2002; 22: 489-90.
- Fournet S, Giacalone PL, Rathat G, Rouleau C. False positive lymph node activity on positron emission tomography (PET/CT) due to hemostatic compresses. J Visc Surg. 2011; 148: e153-5.
- Rickenbacher A, Breitenstein S, Lesurtel M, Frilling A. Efficacy of TachoSil a fibrin-based haemostat in different fields of surgery- a systematic review. Expert Opin Biol Ther. 2009; 9: 897-907.
- Ekici MA, Ekici A, Per H, Tucer B, Kurtsoy A. Foreign body granuloma mimicking upper cervical spinal mass after dural repair with Tachocomb [correction of Tachocomp]: A case report. Pediatr Neurosurg. 2010; 46: 133-7.
