
Open Access, Volume 9
Safety and efficacy of photodynamic therapy for the treatment of malaria in adults in Nigeria: Phase 2 trial
Hans Michael Weber, MD; Robert Weber, MSc; Martin Junggebauer, MSc; Habeeb Ali, MD; Taiwo SS, PhD; Matthias Wojcik, PhD*
Department of Pharmaceutics and Biopharmaceutics, University of Marburg, Germany.
Matthias Wojcik
Department of Pharmaceutics and Biopharmaceutics, University of Marburg, Germany.
Email: matthias.wojcik@pharmazie.uni-marburg.de
Received : July 18, 2023,
Accepted : Sep 08, 2023
Published : Sep 15, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: This is the first randomized controlled trial assessing the efficacy and safety of photodynamic therapy in the treatment of uncomplicated falciparum Malaria in adults. The aim of the current study is to evaluate the use of photodynamic therapy as a possible novel treatment option.
Method: This phase 2 trial of photodynamic therapy for the treatment of Malaria was done in a single centre in Ibadan, Nigeria. Nigerian adults aged 18 years or older, who were diagnosed with malaria caused by Plasmodium falciparum were eligible to participate. Participants were randomly assigned to receive photodynamic therapy or standard Artemisinin-based Combination Therapy (ACT).
Investigators divided the participants into two groups. The intervention group received an intravenous photosensitizer injection of 200 mg Riboflavin followed by intravenous blue (447 nm) and ultraviolet (370 nm) light application. Participants, investigators, and staff undertaking laboratory analyses were masked to group allocation. Photodynamic therapy was applied 5 times within nine days (every second day)
Objectives and endpoints: The primary objective was to evaluate the safety of photodynamic therapy in adults (18+) with uncomplicated malaria (falciparum). Participants were local to an area of high malaria transmission, where the standard treatment is with ACT. Photodynamic therapy was administered 5 times over 9 days and assessed for safety compared to the current standard of care, ACT. The second objective was to evaluate the effectiveness of photodynamic therapy compared to the efficacy of standard ACT malaria therapy.
The efficacy of photodynamic therapy for uncomplicated malaria was measured by clinical and parasitological response (ACPR) twice, once on day 4 (after 2 PDT treatments) and on day 9 (upon completion of 5 PDT treatments). The primary endpoints for safety evaluation were the incidence of serious adverse events (SAE), changes in white blood cell counts (WBC) and haemoglobin/haematocrit within 14 days after first treatment with PDT. All recruited participants who received at least one of both treatments were included in the primary and safety analyses.
Registration of study: ISRCTN registry with trial registration number ISRCTN80135736.
Findings: 200 volunteers were recruited and screened for eligibility with an outcome of 125 eligible participants (35.2% male, 64.8% female) with a mean age of 38.33 years finishing the study successfully. 72 patients (mean age 36.26 years, Std. deviation 13.38) were randomly assigned to receive photodynamic treatment (PDT) and 53 patients (mean age 41.15 years, Std. deviation 13.10) were randomly assigned to receive standard ACT therapy (control group).
In the PDT group the parasite count was significantly decreased from day four onwards with 70.8% of the patients parasite free compared to 53,7% in the ACT group. Mean parasite count on day 4 was reduced from 3552 at baseline to 142,14 (Std Deviation 727,09) compared to a drop from 1881 at baseline to 251,66 (STD deviation 1237,30) at day 4 in the ACT group.
Parasite count was further decreased with PDT showing the following results on day 9 (after the last PDT treatment): 83,3% of the patients in the PDT group tested parasite free compared to 73,3% in the ACT group. Mean parasite count on day 9 was reduced to 11,82 (Std Deviation 34,15) compared to 13,00 (Std deviation 27,57) in the ACT group. White blood cell counts in the PDT group did not change significantly when checked on days 7 and 14 (from 5146,43 (Std 1578,99) at day 0 to 4623,57 (Std 1390,78) at day 7 and 4601,52 (Std 1596,87) on day 14. For the ACT therapy similar results from day 0 to day 14 were observed: 5150,00 (Std 1752,53); 5156,82 (Std 13 77,12); 4778,33 (Std 1293,82). PCV counts in the PDT group did not change significantly when checked on days 7 and 14 (from 5146,43 (Std 1578,99) at day 0 to 4623,57 (Std 1390,78) at day 7 and 4601,52 (Std 1596,87) on day 14. For the ACT therapy similar results from day 0 to day 14 were observed: 5150,00 (Std 1752,53); 5156,82 (Std 1377,12); 4778,33 (Std 1293,82). Severe adverse reactions were reported by no participants in the PDT and ACT groups.
Interpretation: Photodynamic therapy for malaria is safe and induced significant reduction of parasite counts in all recipients after five cycles of treatment.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Wojcik M (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Weber HM, Weber R, Junggebauer M, Ali H, Taiwo SS, Wojcik M. Safety and efficacy of photodynamic therapy for the treatment of malaria in adults in Nigeria: phase 2 trial. Open J Clin Med Case Rep. 2023; 2111.
Introduction
Malaria is a significant public health issue and a leading cause of death in developing countries and tropical regions [1]. According to the World Health Organisation (WHO), an estimated 3.2 billion people in 95 countries and territories are at risk of contracting malaria and developing the disease, with 1.2 billion at a high risk of infection (>1 in 1000 chance per year). In 2015, the global incidence of malaria was estimated to be 214 million cases, with 438,000 deaths, according to the 2015 World Malaria Report [2]. The WHO African Region had the heaviest burden, with approximately 90% of all malaria deaths occurring there, and children under 5 years accounting for over two thirds of all deaths.
The rapid development and spread of antimalarial drug resistance is posing a threat to the progress made in malaria control globally [3]. Currently, parasite resistance to artemisinin [4], which is the primary compound in the most effective and widely administered antimalarial drugs, has been identified in five countries within the Greater Mekong subregion.
The emergence of mosquito resistance to insecticides is a growing concern [5,6], with 60 out of 78 countries that monitor insecticide resistance reporting such resistance in mosquitoes since 2010 [7]. Of these, 49 countries have reported resistance to two or more insecticide classes, according to the World Health Organization (WHO) in 2015 [8]. Given the insecticide and parasite resistance, new treatment options are needed to achieve global eradication of malaria [9]. Photodynamic therapy (PDT), and more specifically, antimicrobial photodynamic therapy (aPDT), could potentially contribute to this goal as it has proven to be effective against multiple pathogens [10,11]. While aPDT is typically used in dentistry to treat periodontitis [12], it involves the application of a substance called a photosensitizer, which is then activated by light of a specific wavelength [13]. This activation leads to the production of reactive oxygen species, causing damage to surrounding cells and resulting in cell death.
Riboflavin, better known as vitamin B2, is a naturally occurring vitamin found in many foods and, based on a wide range of studies, is considered safe even in high doses [14] and has been qualified by the US FDA as GRAS (Generally Recognized as Safe). Riboflavin is free of side effects, inexpensive and at the same time a very potent photosensitizer, as it acts effectively against multiple pathogens in combination with ultraviolet and blue light. The potential role of Riboflavin in the photoinactivation of microorganisms and viruses has been demonstrated in numerous studies under laboratory conditions [15,16]. It is still an intensely investigated field, especially in the decontamination of blood products [17-23] and in the field of transfusion medicine. The aim of this study is to evaluate the safety and efficacy of aPDT as a potential treatment option for eradicating malaria parasites in vivo.
Methods
Study design
The purpose of this randomized controlled trial is to study the efficacy and safety of aPDT for the treatment of uncomplicated falciparum malaria in an adult Nigerian population with the use of Riboflavin as Photosensitizer (PS). During a period of 256 days, 125 patients were recruited and assigned either to a five-treatment cycle of aPDT with Riboflavin within 9 days or standard ACT Therapy. Subjects were randomly assigned to two groups. The following protocol for a single cycle of aPDT was applied: 200 ml Riboflavin-5-Phosphapte-Solution was administered intravenously over a period of 30 mins. 30 mins later, the aPDT treatment followed. For the aPDT treatment, a special fiber optic system (Weber Medical Endolaser) was inserted into the bloodstream. Blue laser (447 nm) was applied for 40 min followed by UVA light (370 nm) for 20 min according to the absorption spectrum of Riboflavin. Patients assigned to the Standard ACT Therapy group received a combination of artesunate and amodiaquine over three days orally (4 mg/kg/day of artesunate and 10 mg/kg/day of amodiaquine).
Study patients
Patients who presented with symptoms of uncomplicated malaria at the clinic were considered eligible for this study. The inclusion criteria included a minimum age of 18 years, a positive result to the malaria test, and a signed informed consent form. The exclusion criteria comprised complicated malaria, multiinfection states, a negative reaction to the malaria test, pregnancy and lactation, disability, and informed dissent.
Study assessment
The primary objective of this study is to determine the incidence of adverse events (AE) that occur up to 14 days post treatment. The study also aims to achieve several secondary endpoints, including the rate of satisfactory clinical and parasitological response (ACPR) on day 4 and 9, changes in haemoglobin/ haematocrit levels until day 14 post intervention, the time frame for fever and parasites to clear, and the occurrence of serious adverse events (SAE).
Datasheet and data collection
Prior to enrolment, participants will be provided with education about the study and given all necessary information. Written consent will be obtained from those who choose to participate. Participants will be randomly assigned to either the control or study group, and it is important to establish a good rapport between investigators and participants during this phase to ensure accurate data collection, particularly with regard to subjective data, such as symptoms.
Both qualitative and quantitative data will be collected during the study. Symptoms reported by study participants will be recorded quantitatively, and participants may be asked to rate the severity of their symptoms on a scale of 1 to 10. Biomedical test results, including PCV, white blood cell counts, and parasite load will be collected as quantitative data. Blood samples for biomedical tests will be taken at specified intervals as outlined in Appendix III. Participation in the study is entirely voluntary, and participants have the right to withdraw at any time.
Statistical analysis
In this study, we will assign sequential numbers to all questionnaires and result sheets, including an identifier for the participant group (control or intervention). Data collection clerks who are trained in the field will carefully review and double-check the accuracy of the collected information, addressing any identified errors or inconsistencies immediately while still in the field.
The data collected will be analysed using the Statistical Package for the Social Sciences (SPSS) software and presented in appropriate tables and charts.
Once the study is complete, the questionnaires and result sheets will be securely stored for a period of five (5) years, after which they will be disposed of in a manner that protects participant confidentiality.
Malaria parasite test: This is a biomedical test to confirm the presence or absence of malaria parasites in a study participant. This will also be used to quantify the parasite load in the participants.
Packed cell volume test (haematocrit): This test determines percentage of red cells in whole blood. This test is an indicator of the severity of malaria as malaria parasites destroy red blood cells in the body.
White blood cell count: This test will only be done on participants in the intervention group to make sure there is no damaging effect on white blood cells.
Results
Patients
Between 01.01.2021 and 13.09.2021, 200 volunteers were recruited and screened for eligibility with an outcome of 125 participants (35.2% male, 64.8% female) finishing the study successfully. 47 Individuals were excluded and 28 could not finish the study.
The mean age of all participants was 38.33 years (range 18-65) with 44 patients aged between 18-35, 43 patients between 36-50 and 38 aged 51 or older. Baseline characteristics were highly similar between both treatment groups (PDT and ACT) and across all ages and sexes.
72 patients (mean age 36.26 years, Std. deviation 13.38) were randomly assigned to receive the photodynamic treatment (PDT) and 53 patients (mean age 41.15 years, Std. deviation 13.10) were randomly assigned to receive standard ACT therapy (control group).
Efficacy
Both treatments resulted in a reduction in measured parasite counts. In the PDT group the parasite count was significantly decreased from day four onwards, with 70.8% of the patients parasite free compared to 53,7% in the ACT group. Mean parasite count on day 4 could be reduced from 3552 at baseline to 142,14 (Std Deviation 727,09) compared to a drop from 1881 at baseline to 251,66 (STD deviation 1237,30) at day 4 in the ACT group.
Parasite count was further decreased with PDT showing the following results on day 9 (after the last PDT treatment): 83,3% of the patients in the PDT group tested parasite free compared to 73,3% in the ACT group. Mean parasite count on day 9 could be reduced to 11,82 (Std Deviation 34,15) compared to 13,00 (Std deviation 27,57) in the ACT group.
Table 1: Parasite count in treatment group before 1sth therapy, after 2nd therapy (day 4) and after 5th therapy (day 9)
| Parasite Count before 1st therapy (day 0) (parasites/microlitre of blood) | Parasite Count after 2nd therapy (day 4) (parasites/microlitre of blood) | Parasite Count after 5th therapy (day 9) (parasites/microlitre of blood) | |
|---|---|---|---|
| Mean | 3552 | 142 | 11.8 |
| Minimum | 29 | 0 | 0 |
| Maximum | 65748 | 4520 | 192 |
Table 2: Parasite count in control group before 1st therapy, after 2nd therapy (day 4) and after 5th therapy (day 9)
| Parasite Count before 1st therapy (day 0) (parasites/microlitre of blood) | Parasite Count after 2nd therapy (day 4) (parasites/microlitre of blood) | Parasite Count after 5th therapy (day 9) (parasites/microlitre of blood) | |
|---|---|---|---|
| Mean | 1881.40 | 251.66 | 13.00 |
| Minimum | 15 | 0 | 0 |
| Maximum | 20000 | 7000 | 128 |
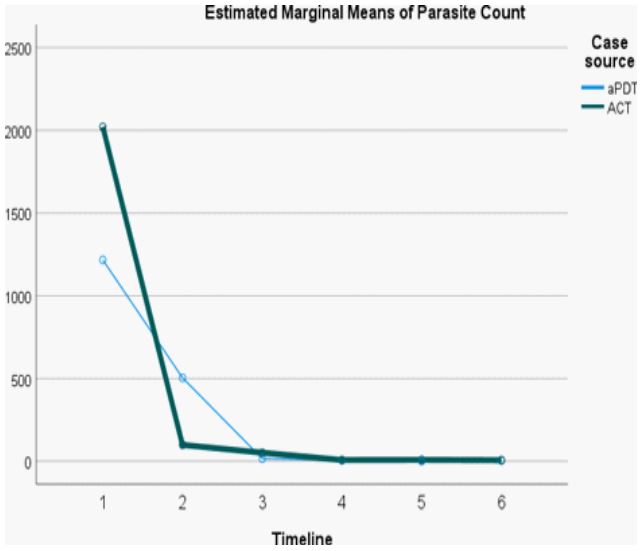
Figure 1: Comparison for estimated marginal means of
parasite count of treatment group and control group.
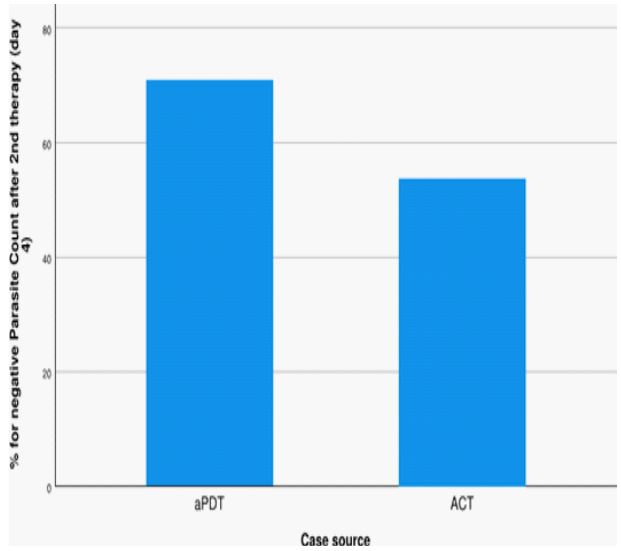
Figure 2: Percentage of negative parasite counts in treatment group vs. control group after 4 days / 2 PDT treatments: 70,8 % patients tested negative in treatment group
compared to 53,7 % in control group.
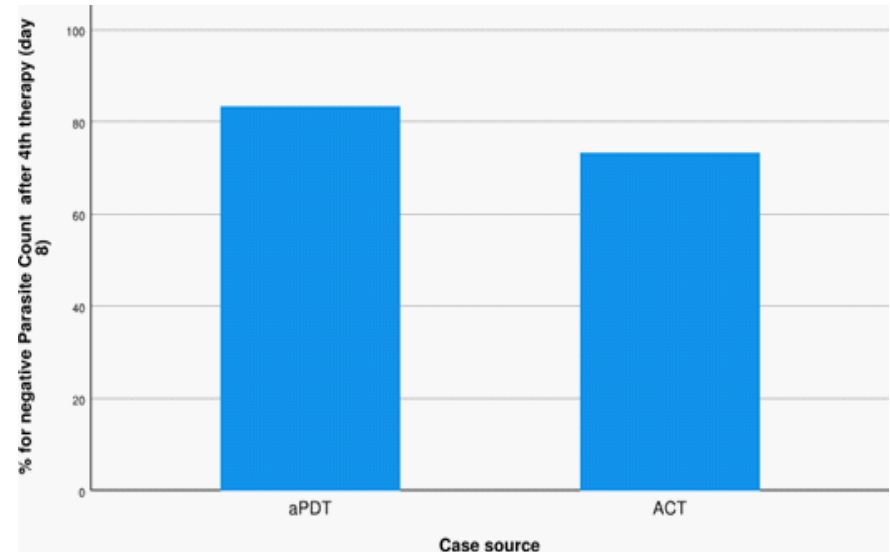
Figure 3: Percentage of negative parasite counts in treatment group vs. control group
after 9 days / 5 PDT treatments: 83,3% patients tested negative in treatment group
compared to 73,3% in control group.
Safety
White blood cell count (WBC) and the packed cell volume indicated as safety markers for both treatment approaches (PDT and ACT).
White blood cell counts in the PDT group did not change significantly when checked on days 7 and 14 (from 5146,43 (Std 1578,99) at day 0 to 4623,57 (Std 1390,78) at day 7 and 4601,52 (Std 1596,87) on day 14. For the ACT therapy similar results from day 0 to day 14 were observed: 5150,00 (Std 1752,53); 5156,82 (Std 1377,12); 4778,33 (Std 1293,82). Severe adverse reactions were reported by no participants in the PDT and ACT groups.
Table 3: WBC counts for treatment and control group measured on day 0, day 7 and day 14
| Group Case source | N | Mean | Std. Deviation | Std. Error Mean | |
|---|---|---|---|---|---|
|
Total wbc day 0 Total WBC on day 0 |
0 aPDT | 70 | 5146,43 | 1578,991 | 188,725 |
| 1 ACT | 53 | 5150,00 | 1752,526 | 240,728 | |
|
Total wbc day 7 Total WBC on day 7 |
0 aPDT | 70 | 4623,57 | 1390,775 | 166,229 |
| 1 ACT | 44 | 5156,82 | 1377,122 | 207,609 | |
|
Total wbc day 14 Total WBC on day 14 |
0 aPDT | 66 | 4601,52 | 1596,871 | 196,561 |
| 1 ACT | 45 | 4778,33 | 1293,818 | 192,871 |
Table 4: PCV counts for treatment and control group measured on day 0, day 7 and day 14
| Group Case source | N | Mean | Std. Deviation | Std. Error Mean | |
|---|---|---|---|---|---|
| PCV day 0 PCV on day 0% | 0 aPDT | 71 | 36,76 | 4,664 | ,554 |
| 1 ACT | 53 | 37,60 | 4,609 | ,633 | |
| PCV day 7 PCV on day 7% | 0 aPDT | 71 | 35,23 | 4,444 | ,527 |
| 1 ACT | 45 | 34,82 | 4,190 | ,625 | |
| PCV day14 PCV on day 14% | 0 aPDT | 66 | 35,52 | 4,459 | ,549 |
| 1 ACT | 45 | 35,84 | 3,289 | ,490 |
PCV counts in the PDT group did not change significantly when checked on days 7 and 14 (from 5146,43 (Std 1578,99) at day 0 to 4623,57 (Std 1390,78) at day 7 and 4601,52 (Std 1596,87) on day 14. For the ACT therapy similar results from day 0 to day 14 were observed: 5150,00 (Std 1752,53); 5156,82 (Std 1377,12); 4778,33 (Std 1293,82). Severe adverse reactions were reported by no participants in the PDT and ACT groups.
Inclusion and Exclusion criteria:
I. Inclusion criteria
i. Adults aged 18 and above
ii. Positive reaction to malaria test (RDT or microscopic test)
iii. Signed informed consent form
II. Exclusion criteria
i. Patients under 18 years
ii. Patients suffering from complicated malaria
iii. Negative reaction to malaria test
iv. Pregnant and lactating women
v. People with disability
vi. Informed dissent
vii. Patients suffering from multiple infections (ie. not malaria alone)
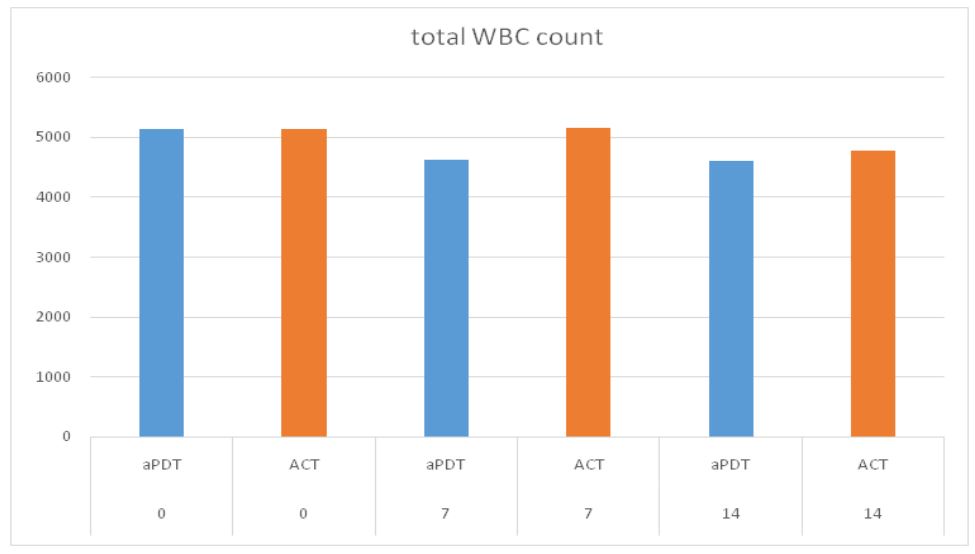
Figure 4: WBC counts during the first 14 days of treatment. Both therapies showed no dangerous
or harmful decrease. A small decrease could be measured during day 0 and 7 aPDT (5146,43 - >
4623,57) and between day 7 and 14 for ACT (5156,82 -> 4778,23).
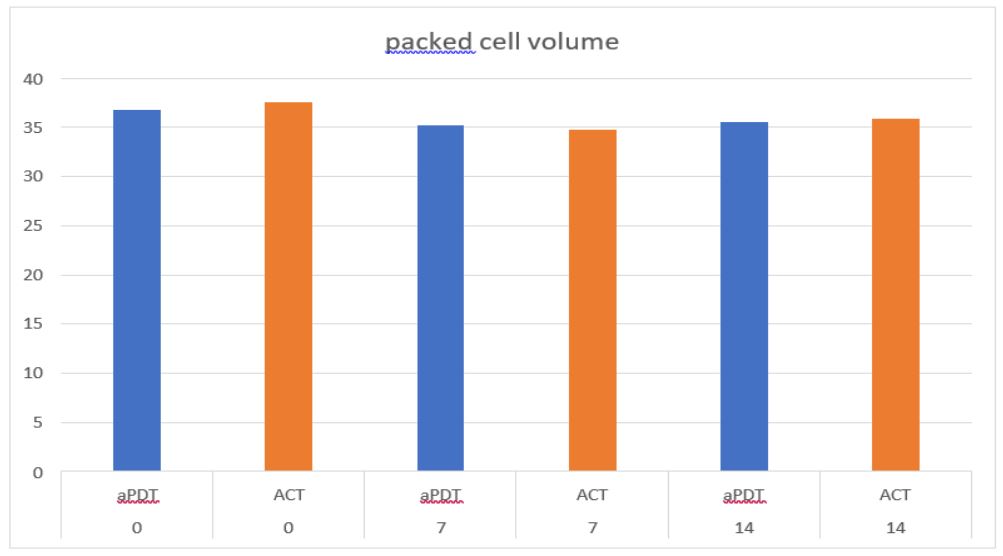
Figure 5: PCV during the first 14 days of treatment. Both therapies showed no dangerous or harmful decrease. No change could be detected for aPDT (36,76; 35,23; 35,52) or during ACT (37,6;
34,82; 35,84).
Discussion
The efficacy of Photodynamic Therapy (PDT) against several microorganisms including p. falciparum could be shown in several in- vitro experiments over the last couple of years [11,16-23]. This in-vitro data could now be confirmed by the first in vivo study in this field on acute Malaria caused by p. falciparum. The results even indicate advantages in the effectiveness and treatment duration of the malaria patients. Furthermore, the obtained data indicate a good tolerability and overall safety of the therapy.
A significant improvement with conventional care, as well as with PDT could be observed. In the aPDT Group with the use of Riboflavin (Vitamin B2) as a photosensitizer the clearance of parasites out of the bloodstream compared to standard ACT therapy after 9 days was 83,3% respectively 73,3%. No dangerous decrease in WBC count could be measured throughout the study in both groups. During both treatments there was no change in packed cell volume detectable. No further side-effects or adverse reactions were reported during the treatment and according to data nor age or gender affected the efficacy or safety. This is consistent with the previous in vitro investigations on aPDT using Riboflavin as an photosensitizing agent [17,21].
A major downfall with conventional therapeutic approaches against microorganisms such as bacteria and parasites is the development of resistance to the effective substances [30-32]. In photodynamic therapy, there is low risk for resistance against the therapeutic approach.
Special mechanisms are required to protect against photodynamic therapy, which have not yet been described for p. falciparum [33]. This might represent a significant advantage in the treatment of Malaria in future disease management strategies.
However, it is important to conduct further investigations in this field to identify and understand possible rapid resistance development. It would also be important to investigate the specificity of riboflavin [34]. The study demonstrates very good tolerability and safety of the therapy, but in the initial experiments, only the influence on blood components, specifically the white blood cell count, was examined. The potential selectivity of riboflavin for specific cell types needs further investigation. Additionally, further studies should examine the effects of PDT in the bloodstream more precisely. It would also be useful to undertake a better evaluation of the dose-response relationship of the activated riboflavin.
Conclusions
The presented study shows first evidence for a successful treatment of Malaria in adults caused by p. falciparum by antimicrobial photodynamic therapy
The applied protocol with Riboflavin as a photosensitizer treated with UVA and blue light systemically proved to be effective in reducing parasite counts significantly without any side-effects or safety concerns.
The results are very encouraging and further research should explore PDT as a potential tool in future disease management strategies for Malaria and other infectious diseases that are affected by rising drug resistances.
Funding: Future Minds Development Initiative, Ibadan Nigeria ISLA Research Group e.V., Germany. Stiftung «Hürzeler», Schweiz (Dr. med. Olaf Kuhnke, Roveredo).
References
- Lopez A, Murray C. The global burden of disease, 1990-2020. 1998; 4: 1241-1243.
- World Health Organization. World malaria report 2022. World Health Organization, 2022.
- White, Nicholas J. «Antimalarial drug resistance.» The Journal of clinical investigation. 2004; 113: 1084-1092.
- Ouji, Manel, et al. «Plasmodium falciparum resistance to artemisinin-based combination therapies: A sword of Damocles in the path toward malaria elimination.» Parasite 25. 2018.
- Metcalf, Robert L. «Insect resistance to insecticides.» Pesticide science. 1989; 26: 333- 358.
- Ranson, Hilary, Janet Hemingway. «Mosquito glutathione transferases.» Methods in enzymology. 2005; 401: 226-241.
- Lee, Sung Eun, Jang Eok Kim, Hol Seon Lee. «Insecticide resistance in increasing interest.» Journal of Applied Biological Chemistry. 2001; 44: 105-112.
- Sparks, Thomas C, Ralf Nauen. «IRAC: Mode of action classification and insecticide resistance management.» Pesticide biochemistry and physiology. 2015; 121: 122-128.
- Greenwood, Brian M, et al. «Malaria: Progress, perils, and prospects for eradication.» The Journal of clinical investigation. 2008; 118: 1266-1276.
- Huang, Liyi, et al. «Type I and Type II mechanisms of antimicrobial photodynamic therapy: An in vitro study on gram‐negative and gram‐positive bacteria.» Lasers in surgery and medicine. 2012; 44: 490-499.
- Cieplik, Fabian, et al. «Antimicrobial photodynamic therapy-what we know and what we don’t.» Critical Reviews in Microbiology. 2018; 44: 571-589.
- Cieplik, Fabian, et al. «Antimicrobial photodynamic therapy for inactivation of biofilms formed by oral key pathogens.» Frontiers in microbiology. 2014; 5: 405.
- Ghorbani, Jaber, et al. «Photosensitizers in antibacterial photodynamic therapy: An overview.» Laser therapy. 2018; 27: 293-302.
- Unna K, Greslin JG. Studies on the toxicity and pharmacology of riboflavin. J Pharmacol Exp Ther. 1942; 76: 75-78.
- Arno Wiehe, Jessica M O’Brien, Mathias O Senge. Trends and targets in antiviral phototherapy. Photochem. Photobiol Sci. 2019; 18: 2565-2612.
- M Wainwright. Photoinactivation of viruses. Photochem. Photobiol Sci. 2004; 3: 406-411.
- E Ben-Hur, RP Goodrich (2011): Pathogen Reduction in Blood for Transfusion Using Photodynamic Treatments. In: M.R. Hamblin and G. Jori (Eds.): Photodynamic Inactivation of Microbial Pathogens. Medical and Environmental Applications, RSC Publishing, Cambridge, UK 2011: 235- 263.
- P Schlenke. Pathogen Inactivation Technologies for Cellular Blood Components: An Update, Transfus. Med Hemother. 2014; 41: 309-325.
- Shawn D Keil, Richard Bowen, Susanne Marschner. MERS-CoV in plasma products using a riboflavin-based and ultraviolet light-based photochemical treatment, Transfusion. 2016; 56: 2948-2952.
- R Schuyler. Use of riboflavin for photoinactivation of pathogens in blood components, Transfus. Apher Sci. 2001; 25: 189- 190.
- Goodrich Raymond. Pathogen Reduction Technology Treatment of Platelets, Plasma and Whole Blood Using Riboflavin and UV Light. Transfusion medicine and Hemotherapy. 2011; 38: 8-18.
- Corbin, Frank. «Pathogen inactivation of blood components: current status and introduction of an approach using riboflavin as a photosensitizer.» International journal of hematology. 2002; 76: 253-257.
- Cardoso, Daniel R, Silvia H. Libardi, and Leif H. Skibsted. «Riboflavin as a photosensitizer. Effects on human health and food quality.» Food & Function. 2012; 3: 487-502.
- Carrera ET, et al. «The application of antimicrobial photodynamic therapy (aPDT) in dentistry: a critical review.» Laser physics. 2016; 26: 123001.
- Mahmoudi, Hassan, et al. «Antimicrobial photodynamic therapy: An effective alternative approach to control bacterial infections.» Journal of lasers in medical sciences. 2018; 9: 154.
- Hu, Xiaoqing, et al. «Antimicrobial photodynamic therapy to control clinically relevant biofilm infections.» Frontiers in microbiology. 2018; 9: 1299.
- Akilov, Oleg E, et al. «Photodynamic therapy for cutaneous leishmaniasis: the effectiveness of topical phenothiaziniums in parasite eradication and Th1 immune response stimulation.» Photochemical & Photobiological Sciences. 2007; 6: 1067- 1075.
- Baptista, Maurício da Silva, and M. Wainwright. «Photodynamic antimicrobial chemotherapy (PACT) for the treatment of malaria, leishmaniasis and trypanosomiasis.» Brazilian Journal of Medical and Biological Research. 2011; 44: 1-10.
- Abdel-Kader, Mahmoud H. Photodynamic therapy. Springer-Verlag Berlin An. 2016.
- Wongsrichanalai, Chansuda, et al. «Epidemiology of drug-resistant malaria.» The Lancet infectious diseases. 2002; 2: 209-218.
- Hedrick, Philip W. «Population genetics of malaria resistance in humans.» Heredity. 2011; 107: 283-304.
- Menard, Didier, Arjen Dondorp. «Antimalarial drug resistance: A threat to malaria elimination.» Cold Spring Harbor perspectives in medicine. 2017; 7: a025619.
- Casas, Adriana, et al. «Mechanisms of resistance to photodynamic therapy.» Current medicinal chemistry. 2011; 18: 2486-2515.
- Walsh, Christopher, et al. «Chemical and enzymic properties of riboflavin analogs.» Biochemistry. 1978; 17: 1942-195.
