
Open Access, Volume 9
Liquid ImmunoBiopsy-based detection of early stage lung cancer in a volunteer subject recruited as a ‘healthy donor’ of a lung cancer diagnosis clinical trial study: A case report
Amit Katz1; Shafrira Shai2*; Fernando Patolsky3; Hagai Drori2; Giora Davidovits2; Eyal J Scheinman2; Eyal Davidovits2; Einat Fireman Klein4; Yaron Saiet1; Yochai Adir4
1Department of General Thoracic Surgery, Rambam Health Care Campus, 8 HaAliya HaShniya St.,PO Box 9602, Haifa 31096, Israel.
2Savicell Diagnostics Ltd., Matam Advanced Technology Park, Building #23, P.O. Box 15050, Haifa 3190501, Israel.
3School of Chemistry, Faculty of Exact Sciences, Tel Aviv University, 69978 Tel Aviv, Israel.
4Pulmonary Division, Faculty of Medicine, Lady Davis Carmel Medical Center, 7 Mikhal St. Haifa 3436212, Israel.
Shafrira Shai, DSc
Savicell Diagnostics Ltd., Matam Advanced Technology Park, Building #23, P.O. Box 15050, Haifa 3190501,
Israel.
Email: shafis@savicell.com
Received : July 18, 2023,
Accepted : Sep 07, 2023
Published : Sep 15, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Developing early detection diagnostic methods, especially non-invasive methods, is a critical component in raising the overall survival rate and prognosis for lung cancer (LC) patients. Recently, we described a novel Liquid ImmunoBiopsy™ test to detect early stage LC with high accuracy. As a part of our ongoing clinical trials for early detection of LC, a blood specimen was received from a ‘healthy’ volunteer, nonsmoker male, who was recruited as a part of the trial’s control group. The Liquid ImmunoBiopsy™ test result of this subject clearly indicated a lung-related malignant lesion. The objective of this article is to provide a detailed description of the subsequent investigation of this case, up to the surgical intervention.
Method: The test specifically quantifies the glycolysis metabolism pathway, which was demonstrated as an accurate biomarker for the activation level of immune cells. Peripheral Blood Mononuclear Cells extracted from the subject’s blood are loaded on a multiwell plate, together with lung tumor-associated antigens and a dedicated fluorescent probe that exhibits a pH-dependent absorption shift. The acidification process (related to the metabolic glycolysis pathway) of the extracellular fluid is monitored by a commercial fluorescence plate reader device.
Results: Following LDCT (low-dose CT) and PET-CT with high suspicion for early lung cancer, the patient underwent thoracoscopic right upper lobectomy. The malignant tumor was removed and identified as NSCLC adenocarcinoma stage IA.
Conclusion: The ImmunoBiopsy™ test with its high specificity (94%) and sensitivity (97%) for detecting early stage lung cancer, low material costs, fast results, and a patient-friendly liquid-biopsy–based blood test make it a promising tool to be used as a mass screening test for LC early diagnosis .
Keywords: Lung cancer; Early stage; Screening test; Liquid biopsy; Tumor associated antigens; Immune cells metabolism.
Abbreviations: LC: Lung cancer; CT: Computed tomography; PET: Positron emission tomography; CTLDCT: Low-dose CT; PBMCs: Peripheral Blood Mononuclear Cells; TAA: Tumor-associated antigen; MA: Metabolic activity; MA-LC: Metabolic activity test for lung cancer; LLOQ: Lower limit of quantification; cfDNA: Circulating cell-free tumor DNA; cfRNA: Cell-free RNA; TEP: Tumor-educated platelets; CTCs: Circulating tumor cells.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Shai S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Katz A , Shai S, Patolsky F, Drori H, Davidovits G, Scheinman EJ, DavidovitsE, et al. Liquid ImmunoBiopsy-based detection of early stage lung cancer in a volunteer subject recruited as a ‘healthy donor’ of a lung cancer diagnosis clinical trial study: A case report. Open J Clin Med Case Rep. 2023; 2110.
Background
Lung cancer (LC) remains the worldwide leading cause of death from all types of cancer. Unfortunately, approximately 75% of patients are diagnosed at an advanced stage of the disease (III, IV) [1]. Despite significant investment and advancement in LC research, only 16% of LCs are detected at the early stages [2]. Thus, even with recent advancements in treatment, survival rates remain poor. Developing early detection diagnostic methods, especially non-invasive methods, is a critical component in raising the overall survival rate and prognosis for LC [3]. Recently, we described a novel Liquid ImmunoBiopsy™ test [4] to detect early stage LC. The novel in-vitro blood test is based on the measurements of metabolic activity profiles of the subject’s immune cells. The test specifically quantifies the glycolysis metabolism pathway, which is a biomarker for the activation level of immune cells. The following describes the Liquid ImmunoBiopsy™ test procedure in brief: Peripheral Blood Mononuclear Cells (PBMCs) are loaded on a multiwell plate together with various lung tumor-associated antigens and a fluorescent probe that exhibits a pHdependent absorption shift. The acidification process (related to the glycolysis metabolic pathway) in the extracellular fluid is monitored by a commercial fluorescence plate reader device in continuous readings. The fluorescent signal is read for 3 hours at 37o C, and documented from each well. Studies show that activation of immune cells requires changes in the way metabolic energy (ATP molecules) is generated. Immune system cells alter their energy generation in order to obtain an effector function. Usually, the shift is from the oxidative phosphorylation cycle into an aerobic glycolysis cycle. This shift provides immediate energy that gives the immune system the ability to attack the foreign antigen [5-7]. Hence, it appears that the activation state of the immune system, in response to tumor development, differs from the non-cancerous state [8-13]. These important discoveries corroborate our hypothesis that changes caused by cancer are reflected in different metabolic activity profiles of immune cells, such as Peripheral Blood Mononuclear Cells (PBMCs), in response to various antigenic stimulants. In general, an effective in-vitro response of the immune cells to re-stimulation with a LC tumor-associated antigen (TAA) stimulant indicates that the immune cells were previously exposed to the specific stimulant. Importantly, it indicates that the cells are able to produce an immunological response to its presence. Recently we described an improved protocol of the Liquid ImmunoBiopsy™ assay, a Metabolic Activity (MA) blood test for LC. We reported a specificity of 94% and a sensitivity of 97% in the detection of early stage (I+II) LC4. As a part of our ongoing clinical trial for early detection of LC, a blood specimen was received from a ‘healthy’, nonsmoker male who was recruited to the ‘healthy population’ control group (healthy, age 50-90Y, and non-smoking). The MA test result of this subject clearly indicated the presence of a malignant lesion. The objective of this article is to provide a detailed description of the subsequent investigation of this case up to the surgical intervention. The Liquid ImmunoBiopsy assay is a non-invasive test, with low material costs, and fast results (within 5 hours from receiving blood at laboratory). This case demonstrates the potential of the Liquid ImmunoBiopsy Assay as a screening test for early diagnosis of LC.
Case Description
A 72-year-old man with no smoking history or any significant medical history was recruited to our clinical trial study on March 5th 2023 at Carmel Medical Center, Haifa, Israel (Ethics committee approval number of the Institutional Review Board is: 0105-13-CMC). Physical examination suggested no significant abnormalities and laboratory findings were within the normal range. The person was found to be eligible to participate in the control group.
The control group main Inclusion Criteria are:
◼ Subject is between 50 to 90 years old.
◼ 30 ≥ BMI ≥ 18.5.
◼Subject with no known malignancy.
The control group main Exclusion Criteria are:
◼ Subject has been previously treated during the last 5 years for any type malignant or benign tumor (for example: colon or uterus polyps removal).
◼ Subject has active infection or inflammation determined clinically at screening.
◼ Subject is currently treated with concomitant medication related directly or can affect the immune system.
◼ Subject is pregnant or lactating or undergoing fertility treatment.
◼ Known history of a significant medical disorder or chronic untreated diseases including HIV, hepatitis B or C, autoimmune disease.
◼ Drug or alcohol abuse.
The Liquid ImmunoBiopsy™ MA test was performed by using the improved protocol of MA test as recently published [4]. The table below shows the reading results of the multiwell plate that was loaded into a commercial fluorescence plate reader device (filter based BioTek – Synergy H1 and Gen5 software ver. 3.12). Fluorescence intensities were measured at 513 nm under sequential excitation at wavelengths of 405 and 455 nm. Acidification process in plate’s wells was monitored in continuous reading for 3 hours at 37o C to document the fluorescent signal received from each well. These reflect time -dependent changes in acid concentration of the extracellular fluid in reaction to exposure to a stimulant or a control. The raw data from the plate reader device are processed instantly using Savicell’s proprietary software.
We observed that the data results of the case report subject (Table 1) presented a profile resembling the features of a LC patient, as known from results obtained from the LC subjects group, and not a profile of a non-cancer control subject as expected. The MA data results of the case report subject are significantly different than the MA data results of a typical non-cancer control subject. We compared each stimulant-induced acidification index value between the case report subject and the typical non-cancer subjects using a t-test. The P value is 0.00714. Thus, the probability of receiving the stimulant acidification results under the assumption that both subjects (the case report subject and typical non-cancer control subject) have the same mean acidification for each stimulant is 0.00714.
The z-score of the case report subject show that eight out of the nine (8/9) stimulants are located in the LC zone.
Table 1: MA test results of the case report and a typical non-cancer subject recruited to the control group.
|
Lung Tumor associated
peptide – Stimulant |
Case report subject -
test’s result |
Typical non-cancer subject –
test’s result |
|---|---|---|
| GRP | 0.322 | 0.070 |
| HER 2 | 0.242 | 0.026 |
| MAGE-A3 sequence a | 0.477 | 0.248 |
| MAGE-A3 sequence b | 0.262 | 0.076 |
| NSE | 0.248 | -0.003 |
| NYESO-1 sequence a | 0.234 | 0.085 |
| NYESO-1 sequence b | 0.752 | 0.399 |
| Peptide 8 – sequence a | 0.045 | 0.003 |
| Peptide 8 – sequence b | 0.117 | 0.007 |
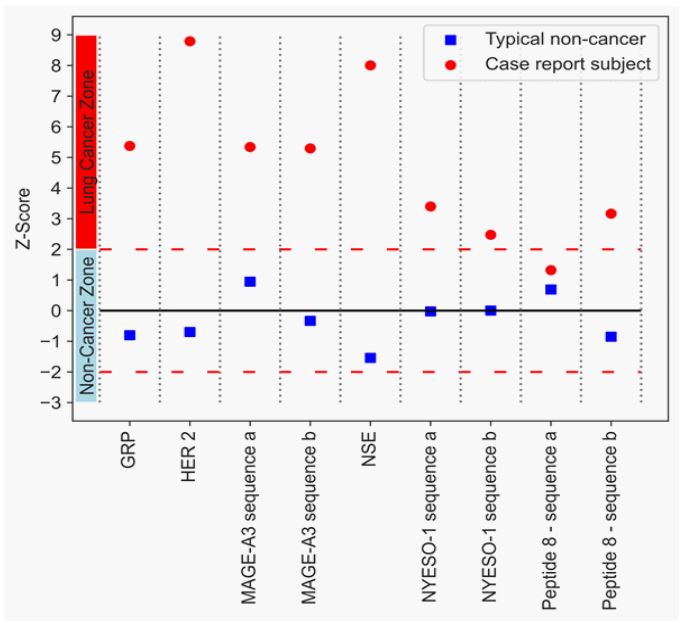
Figure 1: The z-scores of a typical non-cancer subject (blue square) and
the case study subject (red circle). The z-score was calculate using the
mean and standard deviation of non-cancer subjects for each stimulant.
Z-Score is calculated by reducing the mean and dividing by the standard
deviation.
The MA test results of the case report subject indicated a response profile to tumor-associated peptides corresponding wells with a subject with LC malignancy. As a result, the case report subject was clearly suspected to have LC. He was referred for further clinical investigation at the Rambam Medical Center Haifa, Israel. As the Liquid ImmunoBiopsy™ MA test results showed a high-risk metabolic profile for malignancy, the patient was referred to low-dose computed tomography (LDCT) that revealed a 20 x 19 x 16 mm right upper lobe mass with no hilar or mediastinal lymphadenopathies (Figure 2). He underwent a PET scan examination which showed increased 18F-fluorodeoxyglucose (FDG) uptake only in the right upper lobe mass, thus raising a high suspicion for early lung cancer (Figure 3). After a preoperative evaluation that revealed normal lung function test, the patient underwent a uniportal thoracoscopic right upper lobectomy (VATS) with mediastinal lymph node dissection. Patient had uneventful recovery from the surgery and was discharged on postoperative day 2. Pathology confirmed a diagnosis of stage IA (T1b N0 m0) well differentiated adenocarcinoma, 1.5 cm in diameter, with 9 mediastinal and hilar lymph nodes without evidence of metastasis.
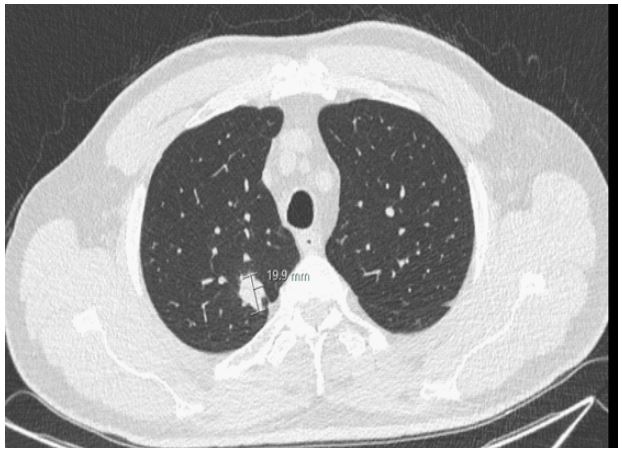
Figure 2: LDCT image Low-dose CT scan showing a solid
lesion measuring 20 x 19 x 16 mm in size, in the right upper lobe.
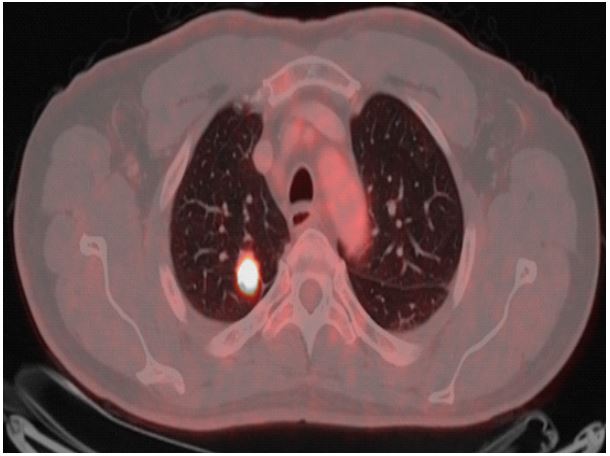
Figure 3: PET-CT image The 18F-fluourodeoxyglucose positron emission computed tomography showing increased
18F-fluorodeoxyglucose (FDG) uptake in the right upper
lobe mass.
Based on these findings the patient was subjected to a lobectomy.
Discussion
Lung cancer is the number one cause of cancer-related deaths. The malignancy is characterized by dismal prognosis and poor clinical outcome, mostly due to the advanced stage at diagnosis. At early stage, many lung cancers are asymptomatic, and can be diagnosed only if subjects participate in a lung cancer screening program. Without a lung cancer screening program, early stage can be only diagnosed by chance, such as an incidental finding in a medical examination that included lung imaging or participation in a clinical study, as with the subject of this described case. Poor clinical outcomes can be partially attributed to the scarcity of early detection strategies [14]. Current diagnostic methods (e.g., Computed Tomography - CT, Positron Emission Tomography - PET, Low-dose CT- LDCT, and radiography) have high sensitivity but low specificity. False positive rates of 96.4% for LDCT and 94% for radiography [15-18] lead to unnecessary follow-up procedures. These can be pronounced in the elderly, where para-physiological changes occur in the lungs which can lead to inappropriate interpretation of radiological findings that put patients at higher risk of over or under treatment, as per Baratella et al [19] and Nunez et al [20] reports. Invasive procedures for diagnosis of LC such as bronchoscopy and needle lung biopsy have limited ability to accurately localize pulmonary lesions that cannot be directly visualized, are expensive and can have significant complication risks [20,21]. Earlier diagnosis of cancer saves lives and significantly reduces treatment costs [22]. Yet, as we mentioned earlier, current clinical tests and diagnostic imaging approaches lack sensitivity and/or specificity in early stage lung cancers [23]. The analysis of cancer-related signals using biological fluids-e.g. a liquid biopsy-has generated great interest in the past decade. Liquid biopsies can identify a wide range of biomolecular features, such as circulating cell-free tumor DNA (cf DNA), cell-free RNA (cf RNA), exosomes, tumor-educated platelets (TEP), and circulating tumor cells (CTCs), and have the potential to give an indication of disease existence and status [1,24-30]. However, most current liquid biopsy techniques lack the detection capability required for early-stage mass screening of cancers [31,32]. We already described a novel, accurate, and non-invasive Liquid ImmunoBiopsy™ test as a tool to diagnose early-stage lung cancer [4]. It measures the function of the immune cells in response to LC antigenic stimuli based on the enhancement of the glycolysis metabolic pathway of immune cells. Glycolysis enhancement is a biomarker for the rapid activation of most immune cells [12]. We reported specificity of 94% and sensitivity of 97% in the detection of early stage (I+II) LC4 . The sensitivity and specificity obtained by the MA-LC ImmunoBiopsy™ test in detecting early-stage lung cancer is considerably higher than the results of numerous currently developed approaches reported in the literature for LC at stages I and II, by using only one method [31-35]. Other current noninvasive biomarkers tests focus on detecting circulating biomarkers, including tumor DNA, tumor antigens, tumor cells, exosomes, and extracellular vesicles. These biomarkers are released to peripheral blood primarily, when the tumor reaches a certain size at a later stage of the disease.
Recently, we recruited to the healthy control group of a clinical trial study a subject who does not have a smoking history and does not belong to any high-risk group for lung cancer. The MA-LC ImmunoBiopsy™ test’s result of his blood sample indicated a response profile to tumor associated peptides of a subject with malignancy, and this blood donor was clearly suspected to have LC. The person was referred for further clinical investigation which included LDCT and PET-CT screening. LDCT showed a suspected lesion (Figure 2). The PET-CT image showed that this lesion is highly suspected to be malignant (Figure 3). Following these findings, he underwent thoracoscopic right upper lobectomy. The malignant tumor was removed and identified as NSCLC adenocarcinoma stage IA. The early detection of lung cancer by the MA-LC ImmunoBiopsy™ test and the subsequent surgery treatment to remove the malignant tumor is expected to lead to a high probability of a full recovery from the LC. We reported4 that the MA-LC ImmunoBiopsy™ test provides results within five hours of receiving the blood sample for MA-LC. The analytical sensitivity of the test is high, with a lower limit of quantification (LLOQ) of 0.000119 (d/minute) in change of acidity over time. It specifically quantifies glycolysis, which is a biomarker for the activation level of immune cells that are re-exposed in-vitro to lung TAA stimulants. Currently, liquid biopsy is mainly utilized as an auxiliary tool in lung cancer diagnosis, when a LDCT detects an abnormality. We believe that the non-invasive MA-LC ImmunoBiopsy™ test, with its low material costs, fast results, and a patient-friendly blood test character, has a potential to be an integral part of lung cancer mass screening programs for high risk populations first and foremost, but as shown in this case, also for a broader population without high risk.
Conclusions
The high specificity (94%) and sensitivity (97%) for detecting early stage lung cancer and low costs of the non-invasive MA-LC ImmunoBiopsyTM test make it a promising tool to be used as a mass screening test for LC in the general population.
Declarations
Ethics approval and consent to participate: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committees and with the 1964 Helsinki declaration and its later amendments (subjects read and signed a dedicated consent form). Ethics committee approval numbers of the Institutional review board are: 0105-13-CMC for Carmel Medical Center, Haifa; 0274-15-RMB for Rambam Medical Center, Haifa; Israel.
Consent for publication: Yes
Availability of data and materials: Available from the corresponding author on reasonable request.
Competing interests: Shafrira Shai, Hagai Drori, Eyal J. Scheinman, Eyal Davidovits, Giora Davidovits, are employed by Savicell Diagnostics and own stock and/or options in Savicell Diagnostics’ parent company. Fernando Patolsky and Yochai Adir are consultants and own stock and/or options in Savicell Diagnostics’ parent company. Amit Katz, Yaron Saiet, Eynat Fireman Klein: none to declare.
Funding: This work was supported by Savicell Diagnostics Ltd
Authors’ contributions: Dr. Amit Katz – Writing -original draft, review & editing, Thoracic surgery medical expert. Principal investigator of clinical trial site.
Dr. Shafrira Shai – Conceptualization, investigation, writing -original draft, review & editing.
Prof. Fernando Patolsky – Biochemistry expert, methodology, review & editing.
Hagai Drori – Formal analysis, data curation, writing - original draft.
Giora Davidovits – Conceptualization, writing - review & editing.
Dr. Eyal Scheinman – Investigation, validation, review.
Eyal Davidovits - Funding acquisition, visualization.
Dr.Yaron Saiet and Dr. Eynat Fireman Klein – Sub-researchers in the clinical trial, directed the patient for medical examinations, review.
Prof. Yochai Adir- Pulmonary medical expert. Principal investigator of clinical trial site.
Acknowledgments: The authors are indebted to Dr. Eran Gilad from Department of General Thoracic Surgery, Rambam Health Care Campus, Israel and to Dr. Yana Kogan, Dr. Sonia Shneer and Dr. Raya Cohen from Pulmonary Division, Faculty of Medicine, Lady Davis Carmel Medical Center, Israel for their help in recruiting suitable subjects for the clinical study and explaining to them the research study and its risks and signing an informed consent form in accordance with the Helsinki Convention. The authors thank Gratzia Luzon, Irena Shahar for their help in coordinating the clinical studies. We greatly appreciate the assistance of the staff of the Department of Thoracic Surgery, Rambam Health Care Campus, Israel.
References
- Knight SB, Crosbie PA, Balata H, et al. Progress and prospects of early detection in lung cancer. Open Biol. 2017.
- American Cancer Society (ACS). Cancer Facts & Figures. 2019.
- Smith RA, Cokkinides V, Brooks D, et al. Cancer screening in the United States, 2011. Cancer J Clin. 2011; 618-30.
- Shai S, Patolsky F, Drori H, et al. A novel, accurate, and non‑invasive liquid biopsy test to measure cellular immune responsesas a tool to diagnose early‑stage lung cancer: A clinical trials study. Respiratory Research. 2023; 24: 52.
- O’Sullivan D, Sanin DE, Pearce EJ, et al. Metabolic interventions in the immune response to cancer. Nat Rev Immunol. 2019; 19324-335.
- Bantug GR, Galluzzi L, Kroemer G, et al. The spectrum of T cell metabolism in health and disease. Nat Rev Immunol. 2017; 1819-34.
- Pearce E, Poffenberger M, Chang C. Fueling immunity insights into metabolism and lymphocyte function. Science. 2013; 3426155.
- Pearce EL, Pearce EJ. Metabolic pathways in immune cell activation and quiescence. Immunity. 2013; 38:633-643.
- Loftus RM, Finlay DK. Immunometabolism: cellular metabolism turns immune regulator. J Biol Chem. 2016; 291: 1-10.
- Chou WC, Rampanelli E, Li X, et al. Impact of intracellular innate immune receptors on immunometabolism. Cell Mol Immunol. 2022; 19: 337-351.
- Pearce EJ, Pearce EL. Immunometabolism in 2017: Driving immunity: All roads lead to metabolism. Nat Rev Immunol. 2018; 8: 81-82.
- Chenchen H, Yuxin X, Xiyang Z, et al. Immune cell metabolism and metabolic reprogramming. Molecular Biology Reports. 2022; 49: 9783-9795.
- Michalek RD, Gerriets VA, Jacobs SR, et al. Cutting edge distinct glycolytic and Lipid oxidative metabolic programs are essential for effector and regulatory CD4+ T cell subsets. J Immunol. 2011; 1863299-3303.
- Siegel RL, Miller KD, Jemal A. Cancer statistics. American Cancer Society. CA A Cancer J Clin. 2018; 68: 7-30.
- Church TR, Aberle D, Clingan KL, et al. Results of initial low-dose computed tomographic screening for lung cancer. N Engl J Med. 2013; 23368: 1980-91.
- The National Lung Screening Trial: overview and study design. Radiol. 2011; 258: 243-53.
- Tanner NT, Aggarwal J, Gould MK, et al. Management of pulmonary nodules by community pulmonologists: a multicenter observational study. Chest. 2015; 148: 1405-14.
- Oken MM, Marcus PM, Hu P, et al. Baseline chest radiograph for lung cancer detection in the randomized Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial. J Natl Cancer Inst. 2005; 97: 1832-1839.
- Baratella E, Fiorese I, Minelli P, et al. Aging-Related Findings of the Respiratory System in Chest Imaging: Pearls and Pitfalls. Curr Radiol Rep. 2023; 11: 1-11.
- Nuñez ER, Caverly TJ, Zhang S, et al. Invasive procedures and associated complications following initial lung cancer screening in a national cohort of veterans. Chest. 2022; 162: 475-484.
- Diddams MJ, Lee HJ. Robotic Bronchoscopy: Review of Three Systems. Life. 2023; 13: 354.
- Birtwistle M. Saving lives and averting costs? The case for earlier diagnosis just got stronger. Cancer Research UK/science blog. 2014; 22.
- IJzerman MJ, de Boer J, Azad A, Degeling K, Geoghegan J, Hewitt C, et al. Towards routine implementation of liquid biopsies in cancer management: it is always too early, until suddenly it is too late. Diagnostics. 2021; 11: 103.
- Goebel C, Louden C, McKenna R Jr, et al. Diagnosis of non-small cell lung cancer for early stage, asymptomatic patients. Cancer Genomics Proteomics. 2019; 16: 229-44.
- WHO International Programme on Chemical Safety. Biomarkers in risk assessment: Validity and validation. EHC 222, 2001.
- Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin Pharmacol Ther. 2001; 69: 89-95.
- National Institute of Health. Lung cancer inheritance pattern. 2019.
- Garber J, Offit K. Hereditary cancer predisposition syndromes. J Clin Oncol. 2005; 23: 276-92.
- Wu TM, Liu JB, Liu Y, Shi Y, Li W, et al. Power and promise of next-generation sequencing in liquid biopsies and cancer control. Cancer Control. 2020; 27: 107327482093480
- Connal S, Cameron JM, Sala A et al. Liquid biopsies: The future of cancer early detection. Journal of Translational Medicine. 2023; 21: 118
- Klein EA, Richard D, Chon A, et al. Clinical validation of a targeted methylation-based multi-cancer early detection test using an independent validation set. Annals of Oncology. 2021; 32: 1167-1177.
- Geoffrey R, Oxnard MD. Multi cancer detection of early stage cancers with simultaneous tissue localization using a plasma cfDNA based targeted methylation assay. Poster, Barcelona ESMO congress. 2019.
- Xue WV, Chuen Wong CS, Shing Cho WC. Early detection and monitoring of cancer in liquid biopsy: advances and challenges. Expert Review of Molecular Diagnostics. 2019; 19: 273-276.
- Jing N, Tao G, Minlin J, et al. Early diagnosis of lung cancer: which is the optimal choice? Aging. 2021; 13: 6214-6227.
- IJzerman MJ, De Boer J, Azad A, et al. Towards routine implementation of liquid biopsies in cancer management: it is always too early, until suddenly it is too late. Diagnostics. 2021; 11: 103.
