
Open Access, Volume 9
Simultaneous occurrence of type 3b esophageal atresia and hypertrophic pyloric stenosis: A rare coexistence
Amit Beher1*; Sabine Ortega-Lawerenz2; Matthias Herbst1; Heike Öhl1; Kay Großer1
1Clinic for Pediatric Surgery, Klinikum Kassel, Kassel, Germany.
2Institute for Pediatric Radiology, Klinikum Kassel, Kassel, Germany.
Amit Beher
Department of Pediatric Surgery, Klinikum Kassel, 34125 Kassel, Germany.
Tel: 056198019563; Email: amit.beher@gnh.net
Received : July 17, 2023,
Accepted : Sep 06, 2023
Published : Sep 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Hypertrophic pyloric stenosis (HPS) and Esophageal Atresia (EA) are two distinct congenital malformations that rarely occur simultaneously. However, there have been reported cases of the simultaneous occurrence of HPS and EA, suggesting a potential relationship between these two conditions. The clinical features of the simultaneous occurrence of HPS and EA can be modified and the diagnosis may be delayed.
Case presentation: We present a rare case of a newborn with simultaneous Type 3b esophageal atresia and hypertrophic pyloric stenosis. Following surgical correction of esophageal atresia, the patient exhibited symptoms of projectile vomiting, which were subsequently confirmed through ultrasound examination to be associated with hypertrophic pyloric stenosis. The patient was successfully managed through surgical intervention, and the outcomes were favorable.
Conclusion: This case report aims to highlight the significance of preoperative screening for hypertrophic pyloric stenosis in patients diagnosed with esophageal atresia, based on current literature.
Keywords: Esophageal atresia; Hypertrophic pyloric stenosis; Transesophageal fistula.
Abbreviation: EA: Esophageal atresia; HPS: Hypertrophic pyloric stenosis ; APGAR: Appearance, pulse, grimace, activity, and respiration - Score; CPAP: Continuous positive airway pressure.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Beher A (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Beher A, Lawerenz SO, Herbst M, Öhl H, Großer K. Simultaneous occurrence of type 3b esophageal atresia and hypertrophic pyloric stenosis: A rare coexistence. Open J Clin Med Case Rep. 2023; 2109.
Introduction
Esophageal atresia (EA) and hypertrophic pyloric stenosis (HPS) are rare congenital anomalies that individually require surgical interventions. However, the simultaneous occurrence of these conditions has only been reported in a few cases. Kate et al. [1] presented a case report describing the simultaneous occurrence of EA and HPS, emphasizing the need for further understanding of this rare occurrence. Chattopadhyay [2] also reported a case of coexistence of EA and HPS, highlighting the challenges in diagnosis and management. Despite the limited literature available, these cases underscore the importance of investigating the simultaneous occurrence of EA and HPS and the potential implications for patient care.

Figure 1: Posterior-anterior X-ray of thorax on admission. High-placed gastric tube lying in the blind sac in case
of esophageal atresia (a). Blown-up intestinal loops as an
indication of tracheoesophageal fistula.
Case Presentation
The delivery was performed at 37 completed weeks of gestation via Cesarean section due to velamentous insertion. The neonate was postnatally vital, with APGAR scores of 7/8/9 and birth weight of 3295 grams (64th percentile). Immediately after birth the infant exhibited respiratory distress and an increased oxygen requirement, necessitating the initiation of CPAP- therapy. Placement of a gastric tube was not feasible, and an X-ray revealed an esophageal blind pouch (Figure 1).
An open surgical approach was chosen to create a precise surgical access and reach the affected area of the esophagus. A type 3b esophageal atresia was found.
The esophageal atresia was carefully opened, and the ends of the healthy esophagus were identified. Utilizing a microsurgical approach, the two ends of the esophagus were connected (Figure 2). To provide additional support and stability during the anastomosis, a transanastomotic tube was employed to splint the esophagus. Following successful esophageal anastomosis, a thorough inspection for potential leaks was performed. No signs of leakage were detected.
On day 7, a postoperative contrast study was performed, revealing no evidence of leakage or stenosis at the level of the anastomosis (Figure 3).
After radiographic assessment the postoperative nutritional intake proved to be challenging. The patient began experiencing repeated episodes of projectile vomiting and showed no signs of weight gain. An ultrasound examination of the abdomen was conducted, revealing the characteristic pattern of hypertrophic pyloric stenosis (Figure 4).

Figure 2: lIntraoperative image of esophageal atresia. The proximal and distal ends of the esophagus are located
close together. The tracheoesophageal fistula is yellow
looped. The azygos vein (blue looped) is kept free.
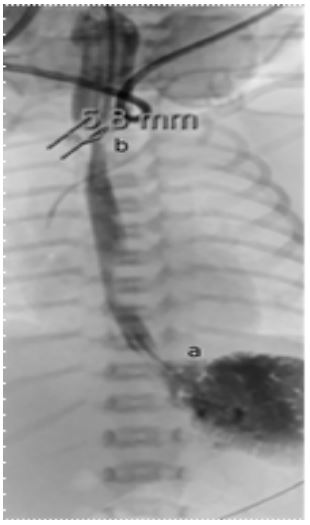
Figure 3: Contrast-enhanced radiographic assessment
was conducted on the 8th postoperative day following
surgical correction of esophageal atresia. The transanastomotic gastric tube remained in situ and was gently
loosened and retracted proximal to the anastomosis (a).
A radiographic contrast agent was administered, revealing
no extravasation or luminal narrowing. The HIS- angle exhibited with a flattened configuration (b)
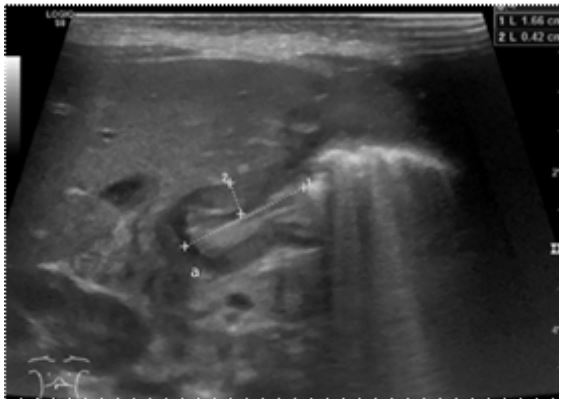
Figure 4: Abdominal ultrasound, revealing a uniform enlargement and wall thickening of the pylorus measuring 1.7
cm x 0.4 cm, consistent with the characteristic radiological
findings of hypertrophic pyloric stenosis (a). Upon instillation of breast milk for probing, no passage through the pylorus was observed, confirming the presence of obstruction.
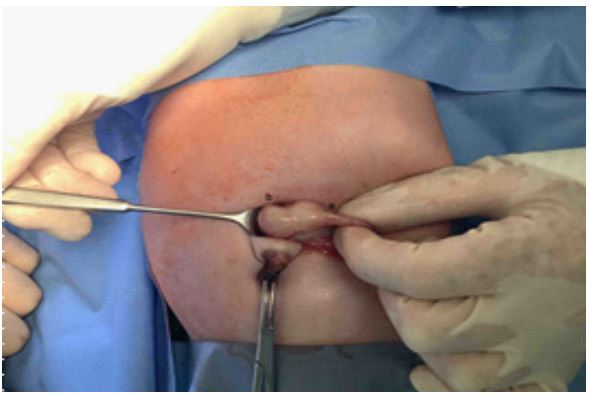
Figure 5: Intraoperative image of hypertrophic pyloric stenosis. Contrasting with the normal thickness of
the pyloric segment (a), the distal aspect of the pylorus
demonstrated uniform enlargement and thickening along
its entirety (b). The surgical access followed the Bianchi
technique.
An open surgical approach using the Bianchi- transumbilical- method was chosen to create a precise access to the pylorus. Intraoperatively, the pylorus exhibited significant hypertrophic, as previously described in the ultrasound (Figure 5). A myotomy was performed, involving the removal of the hypertrophic muscle layer to eliminate the stenosis.
Subsequently, the patient was transferred back to the pediatric intensive care unit for appropriate postoperative care.
The postoperative nutritional rehabilitation was initiated expeditiously, resulting in the cessation of projectile vomiting and the manifestation of appropriate weight gain. On the 24th postoperative day, the patient was discharged to the peripheral general ward, and on the 31th day he was discharged for continued outpatient management.
Discussion
The simultaneous occurrence of esophageal atresia (EA) and hypertrophic pyloric stenosis (HPS) in patients can vary depending on the severity of the conditions and gives unique challenges in diagnosis and management. The exact etiology of the simultaneous occurrence of EA and HPS is not well understood. However, it is believed that both conditions arise from disruptions in the normal embryological development of the gastrointestinal tract. EA is thought to result from a failure of the esophagus to separate from the trachea during fetal development, while HPS is believed to be caused by an abnormal thickening of the muscles in the pylorus [11]. Genetic factors have also been implicated in the development of HPS and EA and may also play a role in the development of congenital malformations [12].
While there is limited literature specifically addressing the need for diagnostic screening of HPS in patients with EA, several studies highlight the importance of comprehensive evaluation and surveillance for associated gastrointestinal abnormalities [3]. Patients with EA often have a higher risk of gastrointestinal complications, including HPS, as reported in various studies [4-8]. The presence of overlapping or nonspecific clinical findings in neonatal gastrointestinal emergencies further emphasizes the need for appropriate imaging to ensure accurate and timely diagnosis [9]. Imaging modalities such as abdominal radiography, upper gastrointestinal (UGI) contrast studies, and contrast enemas play a crucial role in the early and accurate diagnosis of gastrointestinal abnormalities, including duodenal stenosis or HPS [10].
Delayed diagnosis of HPS in patients with EA has been reported, possibly due to modified symptoms and the presence of other comorbidities [2]. The characteristic non-bilious vomiting associated with HPS may be masked or attributed to other factors in patients with EA, leading to a delay in diagnosis. In our case, our patient was first nutriced through gastric tube, which probably dislocated during the contrast enhancement and therefore the patient was first lacking the typical symptom of bilious vomiting. Therefore, a high index of suspicion and careful evaluation are necessary to identify HPS in this population.
Conclusions
In conclusion, the coexistence of HPS and EA is a rare but possible combination of congenital anomalies affecting the gastrointestinal tract in neonates and infants. The exact etiology of this co-occurrence is not well understood, but it is believed to result from disruptions in the normal embryological development of the gastrointestinal tract. The presence of overlapping clinical findings and the increased risk of gastrointestinal complications highlights the importance of comprehensive evaluation and surveillance to detect feeding and swallowing difficulties, as well as to detect and manage potential complications. Appropriate imaging modalities and a multidisciplinary approach involving pediatric surgeons, neonatologists, and gastroenterologists are essential for accurate diagnosis and optimal management. Further research and guidelines specific to the simultaneous occurrence of EA and HPS would be valuable in guiding clinical practice. Surgical intervention remains the mainstay of treatment.
Declarations
Acknowledgements: Our deepest appreciation to all those who have contributed to this work. A special thanks to our colleagues M. Herbst and H. Öhl, performing the operation, as well as K. Großer overviewing the work. Finally, we are grateful to the reviewers for their constructive feedback, improving the quality of our work.
Authors’ contributions: A. Beher drafted the manuscript and participated in its design and coordination. S. Ortega-Lawerenz provided the preoperative and postoperative imaging. M. Herbst and H. Öhl performed the operation and provided the intraoperative images. K. Großer supervised and oversaw our work. All authors read and approved the final manuscript.
Funding: I declare that no significant financial support for this work could have influenced its outcomes.
Availability of data and materials
Ethics approval and consent to participate: Not applicable.
Consent for publication: We obtained the written consent for publication from the participant, in addition to written consent for photography because it contains photographs and radiological images. Proof of consent to publish from study participant can be requested at any time.
Competing interests: The authors declare that they have no competing interests.
References
- Kate C, Brouwer R, Bever Y, Martens V, Brands T, Beelenet al. Infantile Hypertrophic Pyloric Stenosis in Patients with Esophageal Atresia, Birth Defects Research. 2020; 112: 670-687.
- Chattopadhyay A. Pyloric Stenosis in a Patient with Pure Esophageal Atresia: A Difficult Diagnosis. J Indian Assoc Pediatr Surg. 2014; 19: 112.
- Seguier-Lipszyc E, Klin B. Hypertrophic Pyloric Stenosis Following Repair of Esophageal Atresia and Tracheo-esophageal Fistula. J Neonatal Surg. 2014.
- Bögershausen N, Wollnik B. Mutational Landscapes and Phenotypic Spectrum of Swi/snf-related Intellectual Disability Disorders. Front. Mol. Neurosci. 2018.
- Virupakshappa P, Rajendra N. Burden and Spectrum of Neonatal Surgical Diseases In A Tertiary Hospital: A Decade Experience. Int J Contemp Pediatr. 2018.
- Rehman S, Makki, Y, Fazal Z, Babar T, Ishtiaq F, et al. Pattern and Outcome Of Neonatal Gastrointestinal Surgical Emergencies: A Prospective Analysis. TPMJ. 2021; 28: 415-421.
- Uplonkar V, Shinde N, Kumar V. Audit Of Neonatal Congenital Anomalies Required Surgical Intervention At Tertiary Care Centre. Int J Contemp Pediatr. 2019.
- Kepple J, Fishler K, Peeples, E. Surveillance Guidelines for Children With Trisomy 18. Am J Med Genet. 2019; 185: 1294-1303.
- Choi G, Je B, Kim Y. Gastrointestinal Emergency in Neonates and Infants: A Pictorial Essay. Korean J Radiol. 2022.
- Desoky S, Kylat R, Udayasankar U, Gilbertson-Dahdal D. Managing Neonatal Bowel Obstruction: Clinical Perspectives. RRN. 2018.
- Maybee J, Deck J, Jensen E, Ruiz A, Kinder S, et al. Feeding and Swallowing Characteristics of Children with Esophageal Atresia And Tracheoesophageal Fistula. Journal of Pediatric Gastroenterology and Nutrition. 2018; 76: 288-294.
- Fadista, J, Skotte L, Geller F, Bybjerg-Grauholm J, Gørtz S, et al. Genome-wide Meta-analysis Identifies BARX1 and EML4-MTA3 as New Loci Associated with Infantile Hypertrophic Pyloric Stenosis. Human Molecular Genetics. 2018; 28: 332-340.
