
Open Access, Volume 9
A 4:1 ketogenic diet to acute stroke patients is safe and feasible: A randomized controlled trial
Charlotte Gylling Mortensen1; Rie Johanne Pedersen1; Britta Marie Steen1; Helle Klingenberg Iversen2; Per Meden3; Karsten Overgaard4; Jens Rikardt Andersen1,5
1Department of Nutrition, Exercise and Sports, University of Copenhagen, Denmark.
2Department of Neurology, Glostrup Hospital, Glostrup, Denmark.
3Department of Neurology, Bispebjerg Hospital, Copenhagen, Denmark.
4Department of Neurology, Herlev Hospital, Herlev, Denmark.
5Nutrition Unit 5711, Rigshospitalet, Copenhagen, Denmark.
Jens Rikardt Andersen, MD, MPA
Department of Nutrition, Exercise and Sports, University of Copenhagen, Rolighedsvej 26, 1958 FC, Copenhagen, Denmark.
Phone: +4523346654, Fax: +4535332483;
Email: jra@nexs.ku.dk
Received : July 26, 2023,
Accepted : Sep 04, 2023
Published : Sep 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Objective: Ketone bodies can meet more than 60% of brain’s energy needs. Controlled studies consistently show neuroprotective effects in ketotic rodents with induced ischemia. We studied the safety and feasibility of using a ketogenic diet for acute stroke patients and investigated potential neuroprotective effects.
Research Methods & Procedures: Acute stroke patients were randomized to a 4:1 ketogenic diet or to a standard hospital diet for one week at three different hospitals in Copenhagen. Primary endpoints were: physical function, fasting b-glucose and p-C-peptide. Secondary endpoints included: nutritional intake, gastrointestinal complications, lipids, safety blood markers and degree of ketosis.
Results: 17 patients were randomized to intervention (n=6) and control (n=11). Differences were found from baseline to seven days for b-β-hydroxybutyrate (p=0.001), p-phosphate (p=0.009), and energy intake (p=0.005). Three of six patients in the intervention group developed clinically relevant ketosis (>1.5 mmol/l) at a median time of 2.5 days and patients on the ketogenic diet had a higher energy intake (p=0.005). No differences were found on the primary endpoints.
Conclusions: A 4:1 ketogenic diet is safe and well tolerated by acute stroke patients. The diet can increase energy intake, but the degree of ketosis was insufficient for investigating neuroprotective effects of a ketogenic diet. Other methods of inducing acute ketosis need to be developed to reveal potential clinically relevant effects.
Keywords: Acute stroke; ketogenic diet; ketosis; neuroprotection; nutrition.
Clinical Trial Registration Information: clinicaltrials.gov. Unique identifier: NCT01997749.
Copy right Statement:Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Rikardt Andersen J (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Gylling Mortensen C, Johanne Pedersen R, Marie Steen B, Klingenberg Iversen H, Meden P, Overgaard K, Rikardt Andersen J. A 4:1 ketogenic diet to acute stroke patients is safe and feasible: A randomized controlled trial. Open J Clin Med Case Rep. 2023; 2106.
Introduction
A ketogenic diet can exert neuroprotection in epilepsy by reducing seizure frequencies [1]. Clinical studies also suggest that ketone metabolism may improve cognitive function in other neurological conditions such as Alzheimer’s [2,3] and Parkinson’s Disease [4]. There are no published clinical studies regarding stroke, however, a systematic review of 16 controlled rodent studies [5] investigated effects of ketosis on stroke outcomes. All reviewed studies showed beneficial effects on pathological and functional outcomes following experimental stroke, independent of whether ketosis was induced by carbohydrate restriction, ketone bodies or ketogenic diet. The suggested neuroprotective mechanisms include decreased lactate and reactive oxygen species production and improved neuron energy status [6,7]. We investigated the feasibility and safety of a ketogenic diet to acute stroke patients in a randomized, controlled, multicenter trial and assessed effects on physical function, fasting b-glucose and p-C-peptide levels.
Materials and Methods
Study design and period
This unblinded, randomized controlled trial took place in the acute stroke units of three Copenhagen hospitals (Glostrup, Bispebjerg, Herlev). Block randomization was used and randomization was concealed, using sealed, non-transparent envelopes. The Regional Scientific Ethical Committee approved the study protocol and informed written consent was obtained from every participant. The investigation was in accordance with the principles of Helsinki.
Eligibility
Consecutive patients were screened for eligibility. Inclusion criteria were: ischemic or hemorrhagic stroke, National Institutes of Health Stroke Scale (NIHSS) score ≥5, primary and recurrent incidents, age ≥18 years, randomization within 72 hrs after symptom onset and planned hospitalization ≥1 wk. Exclusion criteria were: sub-arachnoid hemorrhage, traumatic hematoma, pancreatic insufficiency or inability to give informed consent (Figure 1, Table 1).
Intervention
Patients were randomized as soon as possible after admittance and diagnostic procedures to a oneweek dietary intervention of a classical 4:1 ketogenic diet or a standard hospital diet. The ketogenic diet (4 g fat to 1 g protein and carbohydrate) intended to give patients a maximum of 20 g of carbohydrate daily and consisted of Ketocal 4:1 Lq® (Nutricia) and a variety of 4:1 ketogenic dishes (ice cream, yoghurt, shakes, muffins, soups and salmon mousse). Prepared at the hospitals, the ketogenic dishes had fixed amounts of calories (500 or 1000 kJ) to facilitate intake estimates. Patients who were able to eat chose their daily diet together with project staff. The selected dishes would then be placed on a tray with the patient’s name to help control that the patient would only eat ketogenic dishes. Patients were encouraged to drink Ketocal 4:1 Lq® in between main meals. For patients requiring enteral nutrition, Ketocal 4:1 Lq® would be provided in 3-5 meals during the day. For all included patients, the intention was to meet a minimum of 75% of their estimated energy needs every day during the intervention period.
Data collection
Baseline data were collected on the inclusion day or day 1. Patients were monitored closely for adverse effects, dietary intake and metabolic blood markers during the intervention period. Follow up measurements took place at 7 days ± 1 day after inclusion, 30 days ± 3 days and 90 days ± 7 days.
Primary outcomes
Primary endpoints included the standard stroke function scores (NIHSS, Barthel 100 and Modified Rankin Score), fasting b-glucose and fasting p-C-peptide. Effects were estimated as difference from baseline score at day 7, 30 and 90. During the intervention period, fasting b-glucose was measured every morning before breakfast. Fasting p-C-peptide was measured in the morning before breakfast at baseline, day 7, 30 and 90.
Secondary outcomes
Secondary endpoints included blood ketone concentration, nutritional markers, gastrointestinal complications, lipids, liver tests, mortality, infections, and electrolytes.
Fasting blood ketone, β-hydroxybutyrate (β-OHB) concentrations were monitored every morning before breakfast during the intervention period (Freestyle Precision, Abbott laboratories, Abbott Park, IL, USA).
Nutritional risk (NRS 2002) was assessed at baseline and day 7, 30 and 90. Food and energy intake was recorded meticulously every day of the intervention period by the research- or ward staff. Intake of the drink thickener, Resource® ThickenUp™, used for patients with some degree of dysphagia, was also recorded daily since it contains carbohydrates and could possibly affect ketosis negatively.
P-LDL and liver biochemistry was measured at baseline and day 7, 30 and 90. Fasting p-triglyceride, p-phosphate, p-potassium, gastrointestinal complications (nausea, vomit, diarrhea, constipation, abdominal pain) and pneumonia were measured/registered daily before breakfast during the intervention period.
Statistical analysis
Mann-Whitney rank sum test was used for unpaired variables, Wilcoxon rank sum test for paired variables, and Fisher’s exact test for binary variables. Statistical analysis was performed by the intentionto-treat principle, using STATA® (version 12.1 ).
Results
Participant flow is summarized in figure 1. Six-hundred-twenty-eight acute stroke patients were screened for eligibility, and 17 patients were randomly assigned to either the intervention (n=6) or the control diet (n=11). Baseline characteristics in the two groups were similar (Table 1). By one week, one patient had died in the control group and by 90 days, one patient refused follow up in the control group.
Table 1: Baseline characteristics for patients with acute stroke. Median (range)/number (%).
| Intervention n=6 | Control n=11 | Total‡ n=17 | |
|---|---|---|---|
| Age, years | 74 (56-88) | 77 (47-91) | 77 (47-91) |
| Men | 2 (33.3) | 6 (54.5) | 8 (47) |
| Stroke: | |||
| Symptom onset to randomization, hrs* | 25.75 (23-48.25) | 31.5 (18.5-70.5) | 30 (18.5-70.5) |
| Hemorrhage | 2 (33.3) | 2 (18) | 4 (23.5) |
| NIHSS | 14 (7-15) | 9 (5-16) | 10 (5-16) |
| Nutrition: | |||
| Nutritional risk (NRS2002) | 2 (2-4) | 3 (2-5) | 3 (2-5) |
| BMI, kg/m2 | 26.7 (21.7-38.2) | 23.3 (17.7-36.2) | 25.8 (17.7-38.2) |
| Tube feeding | 1 (17) | 3 (27) | 4 (23.5) |
| Stroke risk factor: | |||
| Diabetes | 0 (0) | 3 (27) | 3 (17.5) |
‡ P=No significant differences between any groups
Table 2: Whole blood β-hydroxybutyrate values (mmol/L) at baseline and after seven days
| Median (range) | Intervention (n=6) | Control (n=11) | P* |
|---|---|---|---|
| Baseline | 0,2 (0,1-0,7) | 0,3 (0,1-2,2) | N/S |
| 7 days | 1,1 (0,7-3,6) | 0,1 (0,1-0,7) n=10 | 0.001 |
* Mann Whitney rank sum test
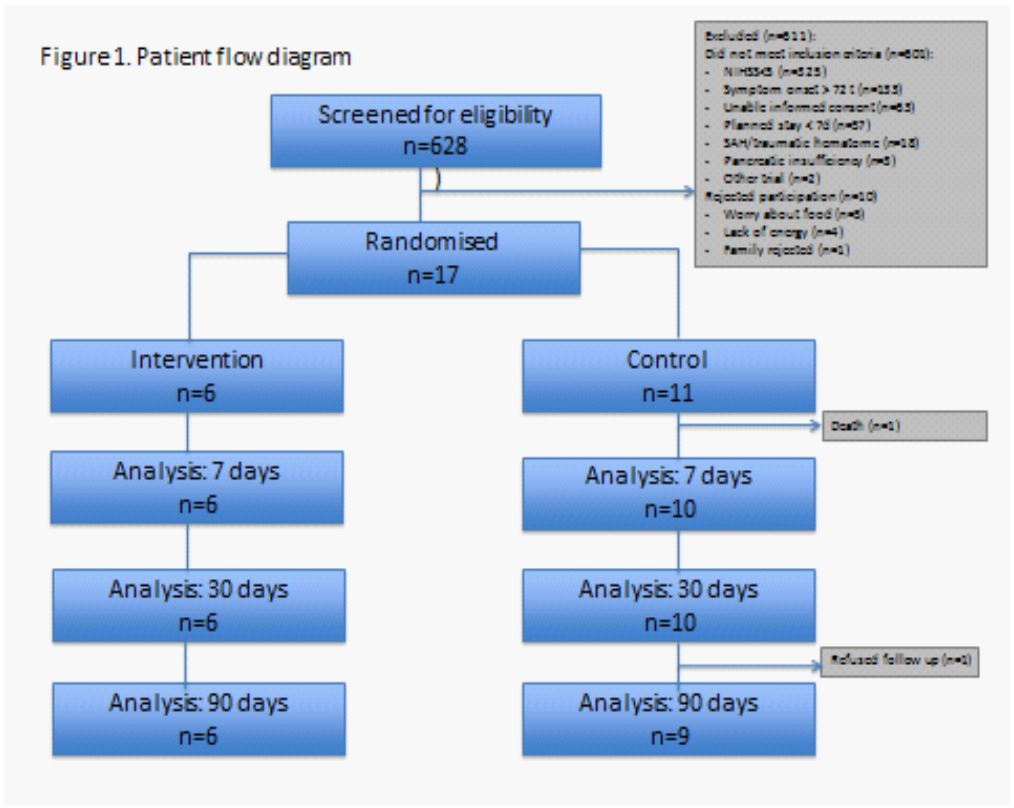
Figure 1: Patient flow diagram.
No differences were found in the primary outcomes, physical function, fasting b-glucose and p-Cpeptide.
Compliance with the ketogenic diet was high and patients in the intervention group had increases in b-β-hydroxybutyrate levels to a median of 1.1 mmol/l (0.7-3.6) after seven days compared to a median of 0.1mmol/l in the control group (0.1-0.7) (p=0.001) (table 2).
Despite the high compliance with the ketogenic diet, only three of six patients in the intervention group developed convincing ketosis (>1.5 mmol/l) after a median of 2.5 days (1-4 days). Two of the three were able to maintain ketosis for the rest of the intervention period. The three non-ketotic patients in the intervention group all used the drink thickener, Resource® ThickenUp™, daily.
The median energy intake in the intervention group ranged from 4560-10040 kJ/day, representing 65-111% of their estimated needs, compared to 2000-6330 kJ/day among control patients, representing 33-85% of their estimated needs (p=0.005, p=0.018, respectively). No difference in nutritional risk screenings in the intervention and control groups were found at 7, 30 and 90 days.
Regarding GI symptoms, lipids, liver tests, mortality or pneumonia, the intervention group did not experience adverse effects different from the control group. Difference in p-phosphate values from baseline-day 7 was significantly higher (p=0.015) in the intervention group, most likely explained by phosphate-rich dairy products in the ketogenic dishes.
Discussion
Most important, our findings indicate that acute stroke patients tolerate a 4:1 ketogenic diet.
Additionally, a ketogenic diet may help acute stroke patients eat sufficiently. This is an advantage because stroke patients typically face initial eating difficulties [8] which increases the likelihood of becoming at nutritional risk while hospitalized [9]. The higher energy intake can most likely be explained by the nutrient density of the ketogenic dishes, which made it relatively easy for patients to meet a minimum of 75% of their estimated energy needs.
Study strengths include the randomized controlled design, high compliance with the diet and proportion of completers (88%). The largest limitation of this study is its small sample size, which was primarily due to very restrictive inclusion criteria, particularly the requirement of a NIHSS score ≥5. Furthermore, the ketogenic diet proved inefficient in inducing and sustaining ketosis on a convincing level. This cannot be explained by low compliance with the diet, since compliance was high, ensured by close communication between patients, their families, ward and research staff and by close monitoring of intake. The most likely explanation for the lack of ketosis among three patients can be explained by their intake of Resource® ThickenUp™ due to various levels of dysphagia. Resource® ThickenUp™ is high in the carbohydrates maltodextrin and zanthan gum, which meant that the patients exceeded the maximum daily intake of 20 grams of carbohydrates in the 4:1 ketogenic diet. The use of Resource® ThickenUp™ was a concern when planning the study, however the hospitals had no alternatives. A fasting protocol that could have induced ketosis more quickly was considered but deemed unethical, because malnutrition is a well-known phenomenon among older stroke patients [8].
To our knowledge, this is the first randomized trial to test effects and safety of a ketogenic diet in patients with stroke in the acute phase. Future research should use other methods for the induction of acute ketosis faster/within few hours such as medium-chain triglycerides [10], ketone esters [11] or fasting if clinically relevant neuroprotective effects are to be obtained in a stroke population. At the same time, the load of fast acting carbohydrates should be minimal.
Disclosures: No author had any conflict of interest.
References
- Levy RG, Cooper PN, Giri P. Ketogenic diet and other dietary treatments for epilepsy (review). Cochrane Database Syst Rev. 2012:1-27.
- Henderson ST, Vogel JL, Barr LJ, Garvin F, Jones JJ, et al. Study of the ketogenic agent AC-1202 in mild to moderate Alzheimer’s disease: A randomized, double-blind, placebo-controlled, multicenter trial. Nutr Metab (Lond). 2009; 6: 31.
- Krikorian R, Shidler MD, Dangelo K, Couch SC, Benoit SC, et al. Dietary ketosis enhances memory in mild cognitive impairment. Neurobiol Aging. 2012; 33: 425.e19-27
- Vanitallie TB, Nonas C, Di Rocco A, Boyar K, Hyams K, et al. Treatment of Parkinson disease with diet-induced hyperketonemia: a feasibility study. Neurology. 2005; 64: 728-730.
- Gibson CL, Murphy AN, Murphy SP. Stroke outcome in the ketogenic state- a systematic review of the animal data. J Neurochem. 2012; 123: 52-57.
- Puchowicz MA, Emancipator DS, Xu K, Magness DL, Ndubuizu OI, et al. Adaptation to chronic hypoxia during diet-induced ketosis. Adv Exp Med Biol. 2005; 566: 51-57.
- Veech RL. The therapeutic implications of ketone bodies: the effects of ketone bodies in pathological conditions: ketosis, ketogenic diet, redox states, insulin resistance, and mitochondrial metabolism. Prostaglandins Leukot Essent Fatty Acids. 2004; 70: 309-319.
- Prosser-Loose EJ, Paterson PG. The FOOD Trial Collaboration: nutritional supplementation strategies and acute stroke outcome. Nutr Rev. 2006; 64: 289-294.
- Mosselman MJ, Kruitwagen CL, Schuurmans MJ, Hafsteinsdottir TB. Malnutrition and Risk of Malnutrition in Patients with Stroke: Prevalence during Hospital Stay. J Neurosci Nurs. 2013; 45:194-204.
- Liu YM, Wang HS. Medium-chain triglyceride ketogenic diet, an effective treatment for drug-resistant epilepsy and a comparison with other ketogenic diets. Biomed J. 2013; 36: 9-15
- Clarke K, Tchabanenko K, Pawlosky R, Carter E, Todd King M, et al. Kinetics, safety and tolerability of (R)-3-hydroxybutyl (R)-3-hydroxybutyrate in healthy adult subjects. Regul Toxicol Pharmacol. 2012; 63: 401-408.
