
Open Access, Volume 9
A case of suspicious fatty liver and seven non-fatty liver cases with hypobetalipoproteinemia, experienced in a community cohort
Akihiro Sonoda; Toshio Shimada*
Department of Shizuoka General Hospital, 4-27-1 Kita-ando, Aoi-ku, Shizuoka, 420-8527, Japan.
Toshio Shimada
Department of Shizuoka General Hospital, 4-27-1 Kita-ando, Aoi-ku, Shizuoka, 420-8527, Japan.
Email: tshimada1946@yahoo.co.jp
Received : Aug 02, 2023,
Accepted : Sep 01, 2023
Published : Sep 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Well knowingly, hypercholesterolemia is a high-risk factor for cardiovascular disease. In contrast, we have not paid much attention to Hypobetalipoproteinemia (HBL) elieve it has a protective effect on the cardiovascular system.
Case Presentation: We encountered eight cases of HBL in a community cohort study of 203 volunteers. One had a suspicious biochemical laboratory finding of fatty liver, with a low-density lipoprotein cholesterol (LDL-C) concentration of 67 mg/dL and apolipoprotein B (apo B) concentration of 48 mg/dL. Other lipid-related variables were normal, except for aspartate aminotransferase (AST) 49 U/L, alanine aminotransferase (ALT) 102U/L, and γ-Glutamyl transpeptidase (γ-GTP) 47 U/L. Generally, liver function was almost normal in the other seven cases with HBL. Laboratory data were within a normal limit in the other seven patients with no clinical signs and symptoms except HBL. However, they had a total cholesterol concentration below 77 mg/dL, corresponding to 5 percentiles of the total cholesterol. We suspected he suffered from primary HBL. If we think seriously about the prevalence rate of HBL in this cohort, perhaps, unexpectedly, HBL may have a little higher prevalence rate in the general population.
Conclusions: Although most cases of HBL are asymptomatic or subtle, some genetic abnormalities cause fatty liver . Because cholesterol is an essential constituent of cell membranes, and a source of steroid hormones and bile acids, perhaps, HBL may be detrimental to the body. We should not disregard HBL but have further interest in HBL.
Keywords: Hypobetalipoproteinemia; Fatty liver; A community cohort study; The Prevalence rate.
Clinical Trial Registration Information: clinicaltrials.gov. Unique identifier: NCT01997749.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Shimada T (2023)
About the Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Akihiro S, Toshio S. A case of suspicious fatty liver and seven non-fatty liver cases with hypobetalipoproteinemia, experienced in a community cohort. Open J Clin Med Case Rep. 2023; 2105.
Introduction
Since abnormal lipid metabolism-related to Hypobetalipoproteinemia (HBL) is associated with a high risk of atherosclerotic vascular diseases such as cerebrovascular diseases and coronary artery diseases, academic societies and medical associations have established guidelines for diagnostic criteria and have been working to prevent such disorders. HBL is closely related to arteriosclerosis or atherosclerosis.
The Japanese Society of Atherosclerosis defines Low-Density Lipoprotein Cholesterol (LDL-C) 140 mg/dL or higher as dyslipidemia. Moreover, we have not paid any careful attention to HBL, except for lipid disorders secondary to diseases.
We started a 5-year cohort study on the preventive effect of taking pesticide-free green tea powder on lifestyle-related diseases in March 2019. Eight of 203 study volunteers had HBL in the laboratory data at starting the study. We encountered a case presenting laboratory findings of suspicious fatty liver despite HBL. The relationship between fatty liver and Hypercholesterolemia has been discussed enough, while there has not been enough discussion on HBL until now.
Case Report
57-year-old male
History: Polypectomy of the colon (+), Achilles tendon rupture (twice)
Current medical history: In treating hypertension with amlodipine besylate 5mg-10mg/day
Initial examination: Height 170.5 cm, weight 69.5 kg, abdominal circumference: 85.5 cm,
BMI: 23.9 kg/m2 , blood pressure: 112/76 mmHg, the pulse rate: 61/min, regular, Heart: sound normal and no murmur, Lung: Normal respiratory sound, no rale.
The study subjects participated as volunteers in the Prefecture Social Health and Medical Research Project to investigate the Health Improvement Effects of Taking Pesticide-Free Green Tea Powder, which began in March 2019. Health examinations were conducted thrice over six months, from March 2019 to September 2019. Among about 200 study subjects, eight volunteers had HBL. One showed the laboratory finding of a suspicious fatty liver despite HBL. Therefore, lipoprotein and apoprotein fractionation were also tested under his consent, and apo B was markedly reduced. The results of lipid and liver function tests have remained unchanged through the subsequent three visits since the study began.
Laboratory findings
Table 1 shows laboratory findings at the beginning study in March 2019. Blood count, immunological, and urine tests were all normal. Biochemical laboratory tests showed LDL-C levels of 67 mg/dL and total cholesterol (TC) levels of 135 mg/dL due to HBL. The TC concentration in Hypocholesterolemia was 135 mg/dL, indicating Hypocholesterolemia. Moreover, triglyceride concentration was 52 mg/dL, and high-density lipoprotein cholesterol (HDL-C) concentration was 53 mg/dL, respectively, within the normal range. Hepatitis laboratory tests were as follows: aspartate aminotransferase (AST) 49 U/L, alanine aminotransferase (ALT) 102 U/L, and γ-Glutamyl transpeptidase (γ-GTP) 47 U/L, which indicates a suspicious fatty liver. As shown in Table 2, apoprotein B (apo B) concentration fell to 48 mg/dL. The apoprotein A-I concentration was 171mg/dL, slightly higher than normal, but other apoproteins levels were within the normal range. Lipoprotein fractionation by agarose gel electrophoresis showed 7.7% (reference range: 7.9 - 23.8) for the Preβ fraction, and that by polyacrylamide gel disk electrophoresis showed 26% (reference range: 46 - 68) for the LDL fraction. The small dense LDL-C (sd-LDL-C) concentration lowered to 7.8 mg/ dL (reference range: 10.7 - 48.7 mg/dL). We also performed thyroid hormone-related and quantitative immunoglobulin tests, within normal limits. Figure 1 shows the histogram of LDL-C in all patients. The red bars at the left end of the histogram show the 10 cases of HBL below 77 mg/dL, corresponding to the five percentiles of the LDL-C data of all patients. Figure 2 plots the LDL-C concentration of all patients on the horizontal axis and the ratio of AST to ALT (AST/ALT) on the vertical axis to clarify the association of HBL cases with suspicious fatty liver laboratory findings. Table 3 shows the baseline data of the other seven patients. Still, seven showed no laboratory findings of suspicious fatty liver, and no abnormal values were worthy of attention in the other parameters.
Table 1: Background of the case.
| Inspection name | Result | Reference range | |
|---|---|---|---|
| T-C | 135 mg/dL | 150-219 | |
| LDL-C | 67 mg/dL | 70-139 | |
| LDL-C | 53 mg/dl | M 40-86 | F 40-96 |
| TG | 52 mg/dL | 50-149 | |
| RLP-C *1 | 2.3 mg/dL | <7.5 | |
| sd LDL-C*2 | 8.0 mg/dL | 10.7-48.7 | |
| AST | 49 U/L | 10-40 | |
| ALT | 102 U/L | 5-40 | |
| AST/ALT | 0.48 | ||
| y-GTP | 47 U/L | M <=70 | F <=30 |
| HbA1c | 5.7 % | 4.6-6.2 | |
| GLU | 96 mg/dL | ||
| Insulin | 8.10 ulU/mL | 1.84-12.2 | |
| C-peptide | 1.71 ng/mL | 0.61-2.09 | |
| BUN | 16.5 mg/dL | 8.0-22.0 | |
| CREA | 0.88 mg/dL | M 0.61-1.04 | F 0.47-0.79 |
| Cystatin C | 0.81 mg/L | M 0.63-0.95 | F 0.56-0.87 |
| UA | 5.7 mg/dL | M 3.7-7.0 | F 2.5-7.0 |
| TP | 7.8 g/dL | 6.7-8.3 | |
| ALB | 4.8 g/dL | 3.8-5.2 | |
| NT-Pro BNP | 11 pg/mL | < =125 | |
| TSH | 2.4 ulU/mL | 0.500-5.00 | |
| Free T3 *3 | 3.9 pg/mL | 2.30-4.30 | |
| Free T4 | 1.23 ng/dL | 0.90-1.70 | |
*1 Remnant-like particle cholesterol.
*2 Small dense LDL-C.
*3 The results of the thyroid test were performed for the
third time.
Table 2: Results of lipid fractionation.
| Inspection name | Result | Reference | range |
|---|---|---|---|
| Apoproteins | |||
| A- I | 171 mg/dL | M 119-155 | F 126-165 |
| A- II | 32.1 mg/dL | M 25.9-35.7 | F 24.6-33.3 |
| B | 48 mg/dl | M 73-109 | F 66-101 |
| C- II | 2.6mg/dL | M 1.8-4.6 | F 1.5-3.8 |
| C-III | 6.4mg/dL | M 5.8-10.0 | F 5.4-9.0 |
| E | 3.2mg/dL | M 2.7-4.3 | F 2.8-4.6 |
| Lipoprotein fraction *3 | *3 Agarose gel electrophoresis | ||
| α | 47.5 % | M 26.9-50.5 | F 32.6-52.5 |
| Preß | 7.7 % | M 7.9-23.8 | F 6.6-20.8 |
| ß | 41.3 % | M 35.3-55.5 | F 33.6-52.0 |
| Preß+B | - - - | ||
| Other | 3.5 | ||
| Band | - - - | ||
| Lipoprotein fraction *4 | *4 Polyacrylamide gel disk electrophoresis | ||
| HDL | 41 % | M 22-47 | F 27-50 |
| LDL | 26 % | M 46-68 | F 44-66 |
| MID Band | 15 % | ||
| VLDL | 18 % | M 3-19 | F 2-12 |
| Band | - - - % | ||
| Protein fraction | |||
| ALB | 60.9 % | 55.8-66.1 | |
| a1-globulin | 3.3 % | 2.9-4.9 | |
| a2-globulin | 8 % | 7.1-11.8 | |
| B1-globulin | 6.6 % | 4.7-7.2 | |
| 32-globulin | 6.2 % | 3.2-6.5 | |
| y-globulin | 15 % | 11.1-18.8 | |
| A/G | 1.6 | 1.3-1.9 | |
Table 3: Other 7 cases of hypocholesterolemia.
| Cases | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Age | 38 | 57 | 77 | 72 | 66 | 37 | 33 |
| Sex (M/F) | F | M | M | F | M | F | F |
| BMI (body mass index) | 22.8 | 23.6 | 22.7 | 17.6 | 25.0 | 19.0 | 21.0 |
| AC (abdominal circumscript) | 70.5 | 88.0 | 90.5 | 75.2 | 89.0 | 68.5 | 70.3 |
| BP (Blood Pressure) | 105 / 61 | 132/82 | 158/84 | 106 / 54 | 150 / 76 | 96 / 53 | 101/61 |
| HR (Heart Rate) | 61 | 75 | 64 | 76 | 80 | 78 | 94 |
| alcoholic habits | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| *LDL-C (LDL-cholesterol) | 61.2 | 66.8 | 69.2 | 69.6 | 70.4 | 74.0 | 75.8 |
| *AST / ALT (AST ALT ratio) | 1.70 | 1.17 | 1.18 | 1.81 | 1.26 | 1.18 | 1.51 |
| AST (aspartate aminotransferase) | 20 | 24 | 28 | 27 | 33 | 20 | 18 |
| ALT (alanine aminotransferase) | 11 | 24 | 20 | 15 | 28 | 17 | 11 |
| y-GTP (y-glutamyl transpeptidase) | 10 | 180 | 20 | 24 | 154 | 35 | 13 |
| TG (triglyceride) | 33 | 118 | 61 | 62 | 107 | 82 | 45 |
| TC (total cholesterol) | 126 | 174 | 140 | 205 | 160 | 153 | 156 |
| HDL-C (HDL-cholesterol) | 56 | 75 | 54 | 113 | 72 | 63 | 68 |
| RLP-C (remnant like particle-cholesterol) | 1.1 | 4.9 | 2.2 | 2.8 | 3.8 | 2.7 | 2.5 |
| Sd - LDL (small dense-LDL-C) | 13.0 | 40.3 | 28.4 | 19.1 | 37.9 | 47.6 | 11.6 |
| Insulin | 5.2 | 3.6 | 3.9 | 3.9 | 3.6 | 3.2 | 9.1 |
| CPR (C-peptide) | 0.84 | 1.08 | 0.90 | 0.75 | 0.74 | 0.95 | 1.13 |
| FBS (fasting blood sugar) | 83 | 101 | 88 | 96 | 96 | 93 | 91 |
| HbA1c (glico hemoglobin A1c) | 5.0 | 5.1 | 5.3 | 5.6 | 5.4 | 4.9 | 5.1 |
| BUN (urea nitrogen) | 15.1 | 13.9 | 14.5 | 12.5 | 10.2 | 18.3 | 9.6 |
| CRE (creatinine) | 0.62 | 0.79 | 0.93 | 0.59 | 0.75 | 0.51 | 0.55 |
| C ys-C (Cystatin-C) | 0,65 | 0.84 | 0.89 | 0.57 | 0.79 | 0.52 | 0.61 |
| UA (uric acid) | 3.6 | 6.6 | 6.8 | 4.4 | 5.8 | 5.5 | 3.3 |
| CRP (C-reactive protein) | 0.02 | 0.05 | 0.10 | 0.16 | 0.03 | 0.24 | 0.24 |
| NT-proBNP (N-terminal fragment of pro-B- type natriuretic peptide) | 92 | 19 | 95 | 44 | 32 | 19 | 30 |
| WBC (white blood cell) | 5300 | 7300 | 6300 | 5300 | 7500 | 8100 | 6200 |
| RBC (red blood cell) | 433 | 439 | 427 | 415 | 436 | 410 | 482 |
| Hgb (hemoglobin) | 13.1 | 14.2 | 14.0 | 12.7 | 14.2 | 12.7 | 13.4 |
| PLT (platelet) | 19.7 | 24.0 | 27.3 | 22.1 | 19.9 | 43.3 | 27.4 |
*Average of observation period
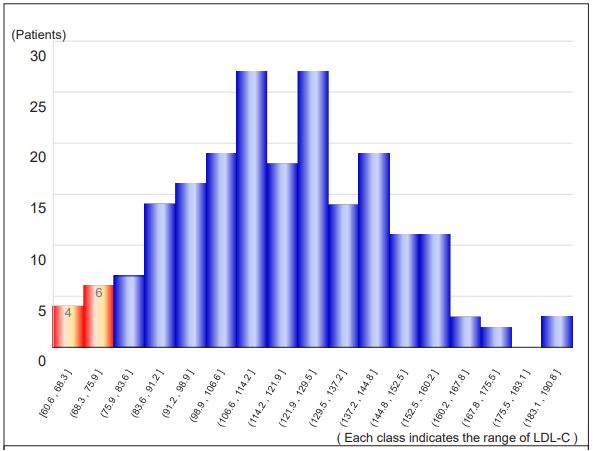
Figure 1: The distribution range of LDL-cholesterol
concentration among all study participants.
If 77 mg/dL, which corresponds to the five percentile of the total, is used as the criterion for hypocholesterolemia, the ten patients shown by the red bars in the graph fall into this category. The distribution, we excluded two patients because they received hyperlipidemia.
If 77 mg/dL, which corresponds to the five percentile of the total, is used as the criterion for hypocholesterolemia, the ten patients shown by the red bars in the graph fall into this category. The distribution, we excluded two patients because they received hyperlipidemia.
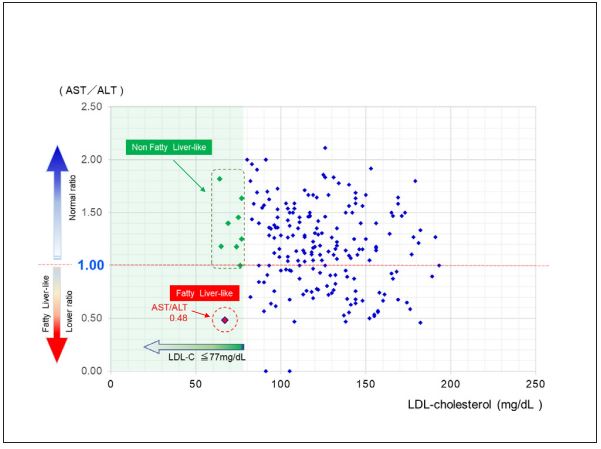
Figure 2: Relationship between LDL-cholesterol and
AST/ALT in study participants.
A red dot indicates a case with fatty liver-like features, and green dots represent the other hypocholesterolemic cases without fatty liver-like features. The ratio of AST to ALT on the vertical axis decreases as the value moves downward, indicating fatty liver-like findings.
A red dot indicates a case with fatty liver-like features, and green dots represent the other hypocholesterolemic cases without fatty liver-like features. The ratio of AST to ALT on the vertical axis decreases as the value moves downward, indicating fatty liver-like findings.
Discussion
HBL, which indicates an extreme decrease in LDL-C, is often secondary to various diseases. Still, primary HBL has also been reported and confirmed as a part of Hypocholesterolemia. We encountered a case with biochemical laboratory findings of suspicious fatty liver despite Hypocholesterolemia in our 5-year cohort study volunteers. HBL is defined as TC and LDL-C levels below the five percentile of the general population adjusted for age, sex, and race [1,2].
In our case, LDL-C levels were 63 mg/dL, which was lower than 77 mg/dL, corresponding to the five percentiles of the overall population. Apo B was lower than the reference value, and AST/ALT was 0.55, suspecting fatty liver laboratory findings. There were no symptoms or findings of small intestinal malabsorption, malnutrition, malignant disease, or hyperthyroidism [3-5], which are thought to be secondary causes of Hypocholesterolemia. Though the patient had only mild hypertension and no history of hepatitis, we attributed the elevated AST and ALT levels and decreased AST/ALT ratio to fatty liver. Therefore, we thought that secondary Hypocholesterolemia is unlikely in this case and HBL is more likely to drive from a genetic abnormality. Generally, HBL is classified into subgroups based on involved genes and the form of inheritance type Familial Hypobetalipoproteinemia (FHBL), which is autosomal dominant; Abetalipoproteinemia (ABL), which is autosomal recessive; and Anderson's Disease (AD) / Chylomicron Stagnation Disease (CRD) are autosomal recessive.
FHBL is an autosomal co-dominant genetic disorder that can cause marked ABL-like Hypocholesterolemia, impaired fat absorption, and neurological symptoms in homozygotes or compound heterozygotes [1]. Most of these are heterozygous and are asymptomatic or have only mild fatty liver and intestinal malabsorption, so we suspect that this case is also likely to be heterozygous. The fatty liver, despite Hypocholesterolemia, is attributed to the decreased release of Very Low-Density Lipoprotein (VLDL) due to abnormal lipoprotein metabolism in the liver. The lipids deposited in the liver due to reduced clearance accumulate triglycerides to produce fatty liver [6,7].
The most common cause of FHBL is a mutation in the apo B gene due to the truncation between apo B-2 and apo B-89. In addition, many genetic abnormalities of proprotein convertase subtilisin Kexin 9 (PCSK9) have also been reported, and the reduction of LDL-C is estimated to be 30-70%. This PCSK9 genetic abnormality can be caused by increased LDL receptor uptake of genetic mutations related to Angiopoietinlike protein 3 (ANGPTL3) [8]. It has been reported that homozygotes show a marked decrease in LDL-C, and compound heterozygotes show a 60% decrease in LDL-C. In comparison, heterozygotes show a 20% decrease in LDL-C, similar to the present case.
Apoprotein B gene mutations account for most FHBLs, with about one in 3,000 [9], and more than sixty types of mutations have been reported [10].
Many papers have reported that HBL with abnormal lipid metabolism is associated with a high risk of developing atherosclerotic vascular disorders such as cerebrovascular and coronary artery disease. However, cholesterol is an essential substance in the composition of cell membranes. It also contributes to synthesizing bile acids and absorbing vitamin E. Cholesterol plays a pivotal role in maintaining our lives. Cholesterol deficiency leads to decreased absorption of vitamin E, which reduces protection against oxidative injury in various body organs, such as increased lipid peroxides, which are closely related to atherosclerosis [11]. Reportedly, this kind of mechanism leads to weakening cell membranes and blood vessel walls; as a result, intracerebral hemorrhage more easily occurs [12,13].
Lipoproteins also bind to and neutralize bacterial endotoxin lipopolysaccharide (LPS) during Sepsis [14].
Compared to homozygous FHBL, heterozygous FHBL with initially mild symptoms.
However, there have been reports of cases of heterozygous FHBL with initially mild symptoms that developed severe neurological dysfunction and severe motor deficits after ten years. After that, dementia followed. The authors warned that even heterozygous FHBL could suffer from liver and systemic metabolic abnormalities [15].
Our study included eight volunteers with suspicious HBL and only one was suspected to have suspicious fatty liver. None showed specific clinical symptoms associated with HBL. Since the subjects were included in the cohort study, genetic tests could not be completed. However, considering the lack of attention and knowledge about HBL and the frequency of low LDL-C cases in this study, we focused on the fact that the prevalence of HBL might be much higher than that of previous reports.
HBL associating with genetic abnormalities includes FHBL and ANGPTL3 homozygosity, which connects to severe hypocholesterolemia. We feel the need to study the dark side of HBL.
Conclusions
We reported an unusual case with suspicious fatty liver and HBLbiochemical features in a community cohort study. Seven of eightHBL patients among 203 volunteers had no signs and symptoms except for HBL. There are rare symptomatic cases with genetic abnormalities. We have realized that Hypercholesterolemia requires medical care. In contrast, we have understood that HBL never requires it. However, some HBL may be associated with fatty liver, which can lead to atherosclerosis and cardiovascular disease. It is also concerned that HBL may not be beneficial or protective to the body because cholesterol is an essential component of cell membranes, and a source of bile acid, and steroid hormones. We should pay more attention to HBL as well as Hypercholesterolemia.
Perhaps, HBL prevalence may be more numerous than we thought as we guess from our cohort study. We may need to pay more attention to HBL as well as Hypercholesterolemia particularly in elderly.
Declarations
Acknowledgments: We sincerely thank Ms. Mikie Shiratori and Ms. Eri Hayasaka, hospital nurses, for their cooperation in this study.
Funding: The authors have no funding to report.
Competing interests: The authors have declared that no competing interests exist.
Acknowledgments: The authors have no support to report.
References
- Linton MF, Farese R V, Young SG. Familial hypobetalipoproteinemia. J Lipid Res. 1993; 34: 521-541.
- Moutzouri E, Elisaf M, Liberopoulas EN. Hypocholesterolemia. Curr Vasc Pharmacol. 2011; 9: 200-212.
- Tawfeeq SM, Al-hamadani HA, Hamzah MT. The Potential Effect of Lipid Profile on Deep Seated Versus Lobar Intracerebral Hemorrhage. 2017; 16: 57-63.
- Mathur N, Mehta A, Mathur M. Hypolipidemia: A study evaluating magnitude and underlying etiologies of the entity. Int J Adv Med. 2021; 8: 183.
- Bonde Y, Breuer O, Lütjohann D, Sjöberg S, Angelin B, et al. Thyroid hormone reduces PCSK9 and stimulates bile acid synthesis in humans. J Lipid Res. 2014; 55: 2408-2415.
- Schonfeld G. Familial hypobetalipoproteinemia: A review. J Lipid Res. 2003; 44: 878-883.
- Hooper AJ, Burnett JR. Update on primary hypobetalipoproteinemia. Curr Atheroscler Rep. 2014; 16: 423-427.
- Welty FK. Hypobetalipoproteinemia and abetalipoproteinemia. Curr Opin Lipidol. 2014; 25: 161-168.
- Burnett JR, Bell DA, Hooper AJ, Hegele RA. Clinical utility gene card for: Familial Hypobetalipoproteinaemia (APOB). Eur J Hum Genet. 2012; 20: 909.
- JP Amanda, MVB Frank, John RB. Monogenic hypocholesterolemic lipid disorders and apolipoprotein B metabolism. Critical Reviews in Clinical Laboratory Sciences. 2005; 42: 515-545.
- Niki E. Lipid oxidation that is, and is not, inhibited by vitamin E: Consideration about physiological functions of vitamin E. Free Radic Biol Med. 2021; 176: 1-15.
- AZ S, Chiu RI, Eggleston-Sexton PM, Beiser A GS. Low cholesterol as a risk factor for primary intracerebral hemorrhage: A case-control study. Ann Indian Acad Neurol. 2012; 15: 19-22.
- Lu JM, Wu MY, Yang ZM, Zhu Y, Li D, et al. Low LDL-C levels are associated with risk of mortality in a Chinese cohort study. Endocrine. 2021; 73: 563-572.
- Dandekar A, Qiu Y, Kim H, Wang J, Hou X, et al. Toll-like receptor (TLR) signaling interacts with CREBH to modulate HighDensity Lipoprotein (HDL) in response to bacterial endotoxin. J Biol Chem. 2016; 291: 23149-23158.
- Musialik J, Boguszewska-Chachulska A, Pojda-Wilczek D, Gorzkowska A, Szymańczak R, et al. A rare mutation in the APOB gene associated with neurological manifestations in familial hypobetalipoproteinemia. Int J Mol Sci. 2020; 21.
