
Open Access, Volume 9
Acute pericarditis complicating transcatheter mitral valve repair: A case report
Andromahi Zygouri*; Eva Nyktari; Dimitrios Alexiou; Ilias Kosmas; Evangelos Leontiadis; Ioannis Iakovou
Department of Cardiology, Onassis Cardiac Surgery Center, Athens, Greece.
Andromahi Zygouri
Department of Cardiology, Onassis Cardiac Surgery Center, Athens, Greece.
Tel: +30-6950968058; Email: andromaxizyg@gmail.com
Received : June 20, 2023,
Accepted : Aug 03, 2023
Published : Aug 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Post-cardiac injury syndrome may occur after acute myocardial infarction, cardiac surgery or percutaneous cardiac interventions, such as percutaneous coronary angioplasty, pacemaker lead insertion and post-ablation procedures. In this case report, we describe the case of an 80-year-old female patient who developed acute pericarditis complicating transcatheter mitral valve repair, performed in our hospital for symptomatic severe degenerative mitral valve regurgitation. Post-cardiac injury syndrome was suspected as the pathophysiological mechanism of our patient’s clinical presentation, after excluding mechanical and infectious causes. Multimodality imaging consisting of focus bedside echocardiography and cardiac magnetic resonance was essential in establishing the diagnosis and the management of the patient by confirming the clinical suspicion.
Keywords: Acute pericarditis; Electrocardiography; Echocardiography; Cardiac magnetic resonance; Multimodality imaging.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Zygouri A(2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Andromahi Z, Eva N, Alexiou D, Ilias K, Evangelos L, Ioannis I. Acute pericarditis complicating transcatheter mitral valve repair: A case report. Open J Clin Med Case Rep. 2023; 2086.
Introduction
Post-Cardiac Injury Syndrome (PCIS) constitutes a clinical syndrome of acute pericarditis due to injury to the pericardium [1]. The responsible pathophysiological mechanism is not completely elucidated. Possibly, a local and systemic inflammatory response of the pericardium sets in which clinically translates into pericardial chest pain, and/or fever, diffuse ST-segment elevation on ECG, pericardial friction rubs or pericardial effusion [2]. Post-cardiac injury syndrome may complicate acute myocardial infarction, cardiac surgery or percutaneous cardiac interventions [1,2]. It also may constitute a very rare complication after transcatheter interventions, mainly transcatheter mitral valve repair, as demonstrated in our case.
Case Presentation
An 80-year-old female patient was referred to our hospital for evaluation for transcatheter mitral valve repair. Over the last 6 months, the patient was complaining for shortness of breath (NYHA III class) due to severe degenerative mitral valve regurgitation. Past medical history included former smoking, peripheral artery disease and moderate renal impairment. Transthoracic echocardiography revealed normal left ventricular systolic function with an estimated left ventricular ejection fraction of 60%, left atrium dilatation and severe degenerative mitral regurgitation, normal right ventricular systolic function, mild tricuspid regurgitation and an estimated pulmonary artery systolic pressure of 55 mmHg.
After evaluation by the Heart Team of our hospital and after discussion with the patient and her family, the patient underwent transcatheter mitral valve repair under transoesophageal guidance with significant reduction of mitral regurgitation, without periprocedural complications.
The third day after the initial intervention, the patient complained of chest pain and fever. Chest pain improved when the patient was leaning forward and became worse when lying flat, as well as with deep inspiration. The patient was normotensive with blood pressure of 130/80 mmHg, with heart rate of 70 bpm, oxygen saturation 97% while breathing ambient air and body temperature of 38.5o C. Cardiac auscultation was unremarkable without any pericardial friction rub. An ECG was conducted and showed sinus rhythm with up to 1 mm concave shaped ST-segment elevation in leads I, II, aVF, V5-V6 without reciprocal changes, as shown in Figure 1.
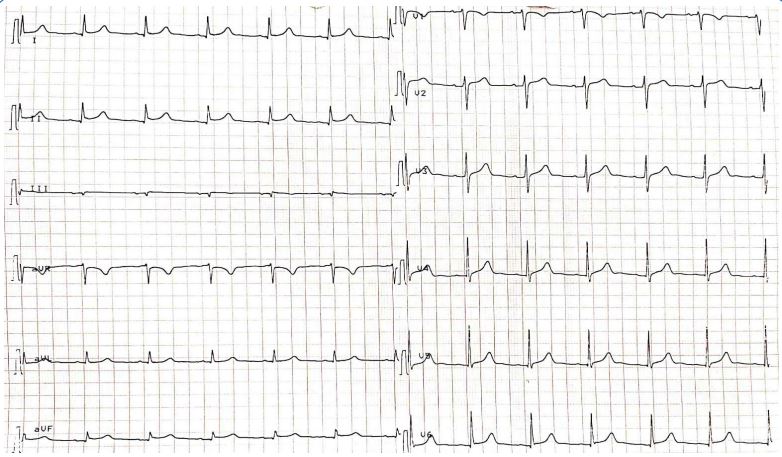
Figure 1:ECG showing sinus rhythm with up to 1-mm concave shaped ST-segment elevation in leads I, II, aVF, V5-V6.
Bedside echocardiography was performed and showed mild circumferential pericardial effusion, without evidence of hemodynamic compromise (Figure 2). A chest X-ray revealed a small left pleural effusion (Figure 3). Echocardiographic studies from day 1 and 2 after the initial operation were reviewed and did not show any pericardial effusion. Thus, the patient had a newly developed pericardial effusion on day 3. Laboratory exams showed elevated white blood cells and c-reactive protein, with negative values of procalcitonin and negative blood cultures on multiple samples. Mechanical and infectious causes of pericardial effusion had been excluded. Post-cardiac injury syndrome was considered as a possible working diagnosis.

Figure 2: Focus bedside echocardiography showing mild circumferential pericardial effusion (white arrows).
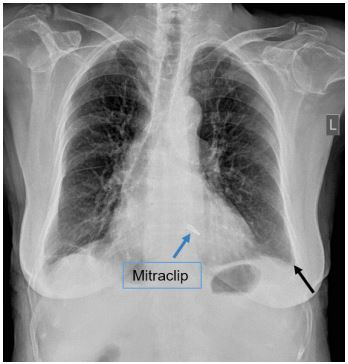
Figure 3: Chest X-ray revealed a small left pleural effusion (black arrow).
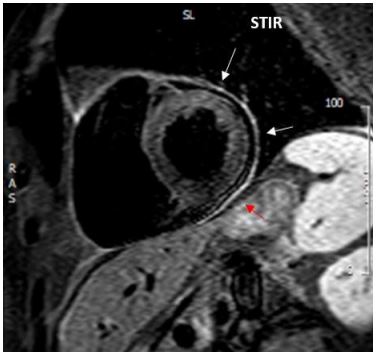
Figure 4:Cardiac magnetic resonance showing diffuse increased signal of the pericardium on T2 STIR image corresponding to inflammation of the pericardium.
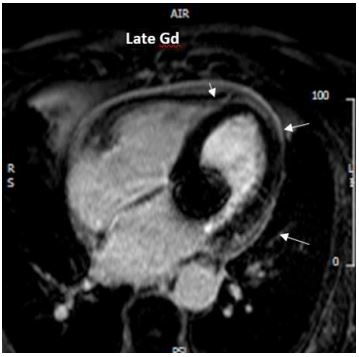
Figure 5: Cardiac magnetic resonance depicting pericardial Late Gadolinium Enhancement (LGE) and a small circumferential pericardial effusion.
Cardiac magnetic resonance finally confirmed the diagnosis of acute pericarditis, by demonstrating diffuse inflammation and oedema of the pericardium (Figure 4). Pericardial late gadolinium enhancement (LGE) was also detected (Figure 5).
Anti-inflammatory therapy was initiated with aspirin 750 mg every 8 hours and colchicine 0.5 mg twice daily and resulted in remission of clinical symptoms and inflammatory biomarkers. Before discharge, on day 10, an echocardiogram was performed and was completely normal, without pericardial effusion. On one-month follow-up, the patient claimed to be asymptomatic with marked improvement in dyspnea and functional capacity. We gradually decreased aspirin dosage during a 3-month follow-up period according to the current guidelines and also continued colchicine for the same period. The patient did not experience any occurrence of pericarditis and is monitored clinically and echocardiographically for detecting possible reccurence or evolution to constriction.
Discussion
This patient presented with fever, pleuritic chest pain, a small new pericardial and pleural effusion and elevated inflammatory markers on the third day after transcatheter mitral valve repair. Mechanical and infectious causes had been excluded. Cardiac magnetic resonance was remarkable for diffuse inflammation and oedema of the pericardium and post-cardiac injury syndrome was considered as the final diagnosis in our patient. Most patients present with chest pain, elevation of inflammatory markers as well as pericardial and pleural effusion [1]. Diagnostic criteria include fever without alternative causes, pleuritic chest pain, friction rub, development of a new or worsening of pericardial effusion in addition to the development of a new or worsening of pleural effusion, after ruling out other causes such as mechanical complications or infectious causes [1]. At least two of these criteria should be present to confirm the diagnosis [1].
The treatment of PCIS, as in acute pericarditis, consists of an anti-inflammatory drug as ibuprofen or high-dose aspirin in addition to colchicine to prevent recurrence [1]. According to our knowledge, only another one case report [3] has been referred in the literature so far and it constitutes a very rare complication after transcatheter procedures. Clinical suspicion and an holistic approach combining comprehensive history, physical examination, laboratory investigations, electrocardiography, echocardiography as well as cardiac magnetic resonance remains crucial for establishing the diagnosis. Early management of acute pericarditis and close follow-up is essential to prevent complications like recurrence and constriction.
Declaration of interests: None
Consent: A patient’s written consent was given.
References
- Yehuda Adler and others, 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS), European Heart Journal. 2015; 36: 2921-2964.
- Ankit Agrawal, Beni Verma, Ashwin Kumar, Abdullah Yesilyaprak, Muhammad Majid, et al. Post ablation pericarditis, Expert Analysis, American College of Cardiology.
- Alachkar MN, Lehrke M, Marx N, Almalla M. Post-cardiac injury syndrome after transcatheter mitral valve repair using MitraClip system: a case report. Eur Heart J Case Rep. 2020; 4: 1-5.
