
Open Access, Volume 9
A case of spondylodiscitis in patient with idiopathic Cd4+ lymphocytopenia
Francesco Giardino*; Simone Longhitano; Melissa Arcidiacono; Andrea Caruso; Pietro Castellino
Department of Internal Medicine, A.O.U. Policlinico “G. Rodolico-San Marco”, Catania, Italy.
Francesco Giardino
Department of Internal Medicine, A.O.U. Policlinico “G. Rodolico-San Marco”, Catania, Italy.
Tel: +390953782905; Email: f.giardino@policlinico.unict.it
Received : May 17, 2023,
Accepted : July 12, 2023
Published : July 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Idiopathic CD4+ lymphocytopenia is a rare and heterogeneous clinical syndrome defined by persistent CD4+ T cell lymphocytopenia in the absence of Human Immunodeficiency Virus (HIV-1) infection or any other cause of immunodeficiency.
These patients typically develop opportunistic infections, malignant tumors and autoimmune disorders.
We describe the case of a 40-year-old man affected by Idiopathic CD4+ limphocytopenia who presented a “Non-Tuberculosis Mycobacterial Lung Disease” complicated by extensive spondylodiscitis.
We performed a vertebral biopsy with detection of Mycobacterium Avium.
The patient began therapy with Isoniazide, Rifampin, Etambutol, Pyrazinamide with progressive clinical and laboratory improvement.
Keywords: Idiopathic CD4+ lymphocytopenia; Primary immunodeficiencies; Spondylodiscitis; Non-tuberculous mycobacteria (NTM).
Abbreviations: HIV: Human Immunodeficiency Virus; NTM: Non-Tuberculous Mycobacteria; NTM-NT: Non-Tuberculous Mycobacteria Lung Disease; CRP: C-reactive protein; ESR: Erythrocyte Sedimentation Rate; EGD: Esophagogastroduodenoscopy; MRI: Magnetic Resonance Imaging; CT: Computed Tomography; PET: Positron Emission Tomography; BAL: Bronchoalveolar Lavage.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Giardino F (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Francesco G, Simone L, Melissa A, Andrea C, Pietro C. A case of spondylodiscitis in patient with idiopathic Cd4+ lymphocytopenia. Open J Clin Med Case Rep. 2023; 2071.
Introduction
Idiopathic CD4+ lymphocytopenia is a rare and heterogeneous clinical syndrome defined by persistent CD4+ T cell lymphocytopenia in the absence of human immunodeficiency virus (HIV-1) infection or any other cause of immunodeficiency. About 258 cases have been described in literature, it might be associated with reduction of CD8+ T lymphocytes and immunoglobulins. These patients typically develop opportunistic infections, malignant tumors and autoimmune disorders [1].
Spondylodiscitis is the infection of one or more intervertebral discs (discites), combined with the infection of one or more vertebrae of the spine (spondylitis).
All vertebrae can be affected, but in 60-70% of cases the lumbar tract is affected.
The most frequent route of infection is hematogenous and the most involved germs are Staphylococci and Streptococci.
Case Presentation
We describe the case of a 40-year-old man who came to our observation for fever, cough and recurrent episodes of abdominal pain. He had received antibiotic therapy with Amoxicillin/Clavulanic Acid 1 gr T.I.D. for 7 days without any benefit.
The patient reported clinical well-being until the age of 37, since then he had several hospital admissions for recurrent infectious episodes. He developed two septic episodes from Staphylococcus Aureus and subsequently from Streptococcus Pneumoniae and episodes of pulmonary Aspergillosis, pneumonia from Micobatterium avium complex and from Cytomegalovirus.
On admission, his abdomen was treatable and tender, thorax examination showed a reduction of vesicular murmur, he had cough, fever up to 39°C, associated with dorsal pain.
In consideration of the patient’s age, the numerous past infectious episodes, including opportunistic infections we investigated and diagnosed Idiopathic CD4+ lymphocytopenia.
Routine blood tests, procalcytonin, HIV-test, several sets of blood cultures during febrile spikes, Quantiferon, lymphocyte typing were within the normal range except for high levels of ESR and CRP and low levels of lymphocytes CD4, CD8 and IgM (Tables 1,2).
Table 1: Laboratory data.
| Variable | On Admission | Reference Range |
|---|---|---|
| Hemoglobin (g/dL) | 9.9 | 12 – 18 |
| Platelet count (per microL) | 377000 | 130000 – 400000 |
| White cell count (per microL) | 5200 | 4800 – 10800 |
| Neutrophils (per microL) | 4210 | 1800 – 7700 |
| Lymphocytes (per microL) | 290 | 900 – 5200 |
| C-reactive protein (mg/L) | 187 | 0 – 5 |
| IgA (mg/dL) | 104 | 70 – 400 |
| IgG (mg/dL) | 942 | 700 – 1600 |
| IgM (mg/dL) | 13 | 40 – 230 |
| Total PSA (ng/mL) | 0.24 | ≤ 4 |
| CA 125 (U/mL) | 21 | < 24.8 |
| CA 19-9 (U/mL) | 9.6 | < 35.4 |
| CA 15-3 (U/ml) | 13 | < 23.4 |
| CEA (ng/mL) | 0.4 | < 5 not smoker |
| < 10 smoker |
Table 2: Lymphocyte Typing.
| Variable | On Admission | Reference range |
|---|---|---|
| T CD3+ Lymphocytes (%) | 71 | 55 – 84 |
| T CD3+ Lymphocytes (cells/microL) | 334 | 690 – 2540 |
| T CD8+ Lymphocytes (%) | 53 | 13 – 41 |
| T CD8+ Lymphocytes (cells/microL) | 250 | 190 – 1140 |
| T CD4+ Lymphocytes (%) | 17 | 31 – 60 |
| T CD4+ Lymphocytes (cells/microL) | 80 | 410 – 1590 |
| T CD45+ Lymphocytes (cells/microL) | 469 | |
| NK CD16+56+ Lymphocytes (%) | 24 | 5 – 27 |
| NK CD16+56+ Lymphocytes (cells/microL) | 113 | 90 – 590 |
| B CD19+ Lymphocytes (%) | 0 | 6 – 25 |
| B CD19+ Lymphocytes (cells/microL) | 1 | 90 – 660 |
| T CD3+ Lymphocytes (cells/microL) | 0.03 | 1 – 3.6 |
The following diagnostic procedures were performed
- Abdominal ultrasound, EGD, Colonscopy and Bone Marrow with no pathologic findings;
- Chest X-Ray showed aerial cavity in the left apical segment;
- CT scan showed: subverting of the lung parenchyma, presence of cavities in the superior lobes (Figure 1).
Given the inconclusive evidences of a pulmonary infection, a broncho-alveolar lavage was performed for standard cultural evaluation, Biofire Filmarray Pneumonia Panel and Koch Bacillus CRP research.
The tests were all negative except for the positive staining of Ziehl-Neelsen.
After B.A.L. a broad-spectrum antibiotic therapy was started, with no significant clinical improvement. The patient continued to have a fever, and high levels of CRP, ESR with negative procalcytonin.
A PET/CT scan showed a significant accumulation of tracer in the lungs and vertebrae. MRI of the spine was permormed, that showed signs consistent with spondylodiscitis extended from D6 to D10 (Figure 2).
In the suspicion of a vertebral localization of atypical Mycobacteria found in the broncho-alveolar lavage (Ziehl-Neelsen positive staining with Koch Bacillus CRP negative) we performed a vertebral biopsy with detection of Mycobacterium Avium [2,3].
We have therefore confirmed the diagnostic suspicion of “Non-Tuberculosis Mycobacterial Lung Disease complicated by extensive spondylodiscitis".
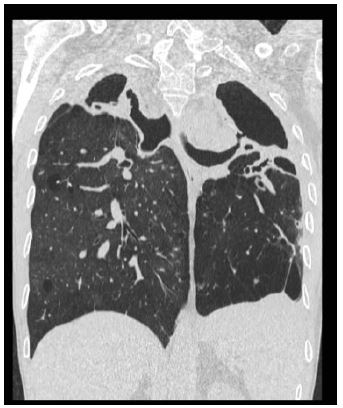
Figure 1: (Subverting of the lung parenchyma, presence of cavities in the superior lobes).

Figure 2: (spondylodiscitis extended from D6 to D10).
After consulting with the infectious specialists, the patient was started on therapy with Isoniazide, Rifampin, Etambutol, Pyrazinamide with progressive clinical and laboratory improvement [4].
Discussion
Primary immunodeficiency diseases are inherited defects of the innate or adaptive arms of the immune system that lead to an increase in the incidence, frequency, or severity of infections and/or immune dysregulation [5]. In a patient with numerous infectious episodes, in the absence of an apparent secondary cause, a primary immunodeficiency should always be ruled out. The present case, infectious episodes started at the age of 37 including opportunistic infections that very rarely affect an immunocompetent subject. The term Non Tuberculous Mycobacteria (NTM) generally refers to mycobacteria other than the Mycobacterium tuberculosis complex and M. leprae [6]. NTM are ubiquitous in the environment, including household water, natural water sources, and soil [7]. Human disease due to NTM is classified into four distinct clinical syndromes: Chronic pulmonary disease (NTM-LD), lymphadenitis, cutaneous disease, and disseminated disease. Of these, chronic pulmonary disease is the syndrome most commonly encountered clinically [6]. Most NTM disease is assumed to originate from environmental NTM [7]. Among the many possible sources of infection, airborne NTM may play an important role in respiratory disease [6]. NTM are quite resistant to commonly used water disinfectants, such as chlorine, and the ability of NTM to persist in urban water supplies may therefore be contributing to the increasing prevalence of NTM lung disease in many countries [7]. At variance with pulmonary tuberculosis, person-to-person transmission is considered an unlikely source for NTM respiratory disease for most patients [6], although evidence for this type of transmission has been reported for Cystic Fibrosis (CF) patients infected with M. Abscessus Complex (MABC) [8,9]. Ingestion is likely to be an important source of infection for children with NTM cervical lymphadenitis and for the majority of human immunodeficiency virus-infected patients, in whom M. avium dissemination begins as gastrointestinal colonization [6]. Direct inoculation of NTM organisms from water or some other material is likely to be a source of infection for those with skin and soft tissue infections [6].
Patients suffering from NTM-LD have a rather vague symptomatology that includes fever, weight loss, cough, asthenia (generalized psycho-physical fatigue), gastrointestinal disorders, night sweating and the presence of blood in the sputum, clinical management may require frequent and prolonged hospitalization. Patients at greater risk for infection include individuals over the age of 50, those with HIV infection, those with cystic fibrosis or lung disease such as Chronic Obstructive Pulmonary Disease (COPD), and those undergoing immunosuppressive therapies [10].
Spondylodiscitis is the infection of one or more intervertebral discs (discites), combined with the infection of one or more vertebrae of the spine (spondylitis).
All vertebrae can be affected, but in 60-70% of cases the lumbar tract is affected.
The most frequent route of infection is hematogenous and the most involved germs are Staphylococci and Streptococci [11].
The main clinical manifestation of spondylodiscite is pain typically localized in the area of the infected discal space and is exacerbated by physical activity or percussion in the affected area. Pain may radiate to the abdomen, leg, scrotum, groin or perineum. Fever is present in about 50% of patients. If not diagnosed and treated in time, it can cause severe neurological deficits and even death. Since spondylodiscitis’ symptoms are rather nonspecific, diagnosis often is reached late in the course of the disease and always requires the use of a wide range of diagnostic tests [12].
Our patient, in recent years, had several infectious episodes, in particular had a pneumonia from MAC, treated with specific antibiotics but for a duration not sufficient to establish the eradication. The NTM bacteria remain initially in a phase of latency within the cavities, due to the known immunodeficiency, determined first a reactivation and then the diffusion by haematogen and localization at the vertebral level.
Thanks to the PET/CT, we were able to highlight the vertebral involvement, which was then confirmed by the MRI of the spine and finally by the cultural examination through vertebral biopsy [13,14].
To our Knowledge this is the second description of a multiple spondylodiscitis secondary to atypical mycobacterial infection in patient with idiopathic CD4 Lynfhocytopenia [14].
In conclusion, immunodeficiency patients are very fragile patients, susceptible to opportunistic infections like HIV patients. All the causes of infections must always be researched, even the rarest ones with any unusual localizations. It is crucial to ensure that the infection has fully resolved at the end of a course of antibiotics, as patients with immunodeficiency almost always require longer treatment periods.
References
- Vijayakumar S, Viswanathan S, Aghoram R. Idiopathic CD4 Lymphocytopenia: Current Insights. Immunotargets Ther. 2020; 9: 79-93.
- Steven Cowman, Jakko van Ingen, David E. Griffith- Henkle E, Winthrop KL. Non-tuberculous mycobacteria infections in immunosuppressed hosts. Clin Chest Med. 2015; 36: 91-99.
- Charles S Haworth, John Banks, Toby Capstick, Andrew J Fisher, Thomas Gorsuch, et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD).Thorax. 2017; 72.
- Charkes L Daley, Kevin L Winthrop. Mycobacterium avium Complex: Addressing Gaps in Diagnosis and Management. J Infect Dis. 2020; 222: S199-S211.
- Ashley L Devonshire, Melanie Makhija. Approach to primary immunodeficiency. Allergy Asthma Proc. 2019; 40: 465-469.
- Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, et al. ATS Mycobacterial Diseases Subcommittee, American Thoracic Society, Infectious Disease Society of America. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007; 175: 367-416.
- Falkinham JO, III. Environmental sources of nontuberculous mycobacteria. Clin Chest Med. 2015; 36: 35-41.
- Bryant JM, Grogono DM, Greaves D, Juliet F, Iain R, et al. Whole-genome sequencing to identify transmission of Mycobacterium abscessus between patients with cystic fibrosis: a retrospective cohort study. Lancet. 2013; 381: 1551-1560.
- Bryant JM, Grogono DM, Daniela RR, Isobel E, Karen PB, et al. Emergence and spread of a human-transmissible multidrug-resistant nontuberculous mycobacterium. Science. 2016; 354: 751-757.
- Nontuberculous Mycobacteria Lung Disease (NTM-LD): Current Recommendations on Diagnosis, Treatment, and Patient Management. Int J Gen Med. 2022; 15: 7619-7629.
- Lars Homagk, Daniel Marmelstein, Nadine Homagk, Gunther O. Hofmann. SponDT (Spondylodiscitis Diagnosi and Treatment): Spondylodiscitis scoring system. J Orthop Sure Res. 2019; 14: 100.
- Safak Kaya, Sehmuz Kaya, Seyhmus Kavak, and Senol Comoglu. A disease that is difficult to diagnose and treat: Evaluation of 343 spondylodiscitis cases. J Int Med Res. 2021; 49.
- Carolijn Smids, IIse J. E. Kouijzer, Fidel J. Vos et al. A comparison of the diagnostic value of MRI and F-FDG-PET in suspected spondylodiscitis. Infection. 2017; 45: 41-49.
- Tetsuro Kobayashi, Eriko Morino, Jin Takasaki, Yoshinori Nagahara, Haruhito Sugiyama. Nontuberculous Mycobacterial Osteomyelitis in Human Immunodeficiency Virus-Negative Patients: A Case Series. Jpn. J. Infect. Dis. 2016; 69: 149-150.
