
Open Access, Volume 9
Squamous cell carcinoma of the ovary on dermoid cyst: About a case and review of the literature
Sarah Tabouri¹*; Nawel Maaref¹; Jezia Bentchouk²; Fadl-Allah Aboubekr³
1Department of Medicine, Djillali Liabes University Medical oncology, Cancer Center of Sidi Bel Abbes, Algeria.
2Department of Medicine, Djillali Liabes University Breast and pelvic surgery, Cancer Center of Sidi Bel Abbes, Algeria.
3Department of Medicine, Djillali Liabes University Gynecology and obstetrics, public hospital for mothers and children, Algeria.
Sarah Tabouri
Department of Medicine; Djillali Liabes University Medical oncology, Cancer Center of Sidi Bel Abbes, Algeria.
Email: tabourisarah@yahoo.com
Received : May 17, 2023,
Accepted : July 10, 2023
Published : July 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Presumed benign ovarian cysts are a common condition in gynecology-obstetrics. They can present with various anatomical, radiological, and histological features. It is difficult to determine the exact incidence of benign ovarian cysts in the population. Some are functional and do not require surgical intervention unless complications arise, while others are organic and may require surgical treatment. Approximately 1 to 4% of these presumed benign cysts will be found to be malignant upon histopathological examination.
Ovarian dermoid cysts, also known as mature teratomas, are benign germ cell tumors that account for 10 to 20% of ovarian tumors. Their transformation into malignant tumors is rare, occurring in less than 2% of cases and typically observed in menopausal women. While the occurrence of dermoid cysts in older age groups is higher than that of benign cysts, the clinical presentations can be similar.
The definitive diagnosis is made based on histopathological results. In 80% of cases, the histological type is squamous cell carcinoma, but other histological variations can occur, such as adenocarcinoma, carcinosarcoma, or even angiosarcoma.
We will report a case of squamous cell carcinoma of the ovary arising from a malignant dermoid cyst in a 40-year-old non-menopausal woman.
Keywords: Ovarian cancer; Squamous cell carcinoma; cysts.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Tabouri S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Sarah T, Nawel M, Jezia B, Fadl-Allah A. Squamous cell carcinoma of the ovary on dermoid cyst: About a case and review of the literature. Open J Clin Med Case Rep. 2023; 2070.
Observation
A 39-year-old woman, gravidity 4, parity 4, without any notable medical history, presented with pelvic pain associated with significant abdominal distension. Clinical examination revealed a mobile abdominopelvic mass. Pelvic ultrasound showed a 12-centimeter right ovarian cyst without intracystic vegetations, appearing as a simple dermoid cyst, and a simple left ovarian cyst. The patient was admitted to the operating room, and during surgical exploration, a ruptured cystic mass with adhesion to the right ovary and peritoneum was found. Tumor resection, right salpingo-oophorectomy, and peritoneal lavage were performed. The histopathological report confirmed a well-differentiated squamous cell carcinoma arising from a right mature teratoma with peritoneal infiltration. A postoperative pelvic MRI revealed three peritoneal nodules predominantly composed of fibrous tissue, located behind the left rectus abdominis muscle and anterior to the anterior aspect of the fundic corporo-uterine region. A routine 4-centimeter left ovarian luteal cyst was also observed. The patient underwent a second surgery, including total hysterectomy, left salpingo-oophorectomy, pelvic and para-aortic lymph node dissection, omentectomy with removal of tumor nodules, appendectomy, and resection of parietal nodules. The histopathological report confirmed that the omentectomy specimen and parietal nodule were infiltrated by a well-differentiated squamous cell carcinoma of ovarian origin. Additionally, the left ovarian, uterine, and cervical walls appeared normal, and all 15 excised lymph nodes showed reactive changes. An MRI performed four weeks after the second surgery revealed a 7.5-centimeter tissue mass in the right iliac fossa adherent to the right iliac muscle. Following a multidisciplinary discussion, the patient received chemotherapy consisting of Carboplatin and Paclitaxel.
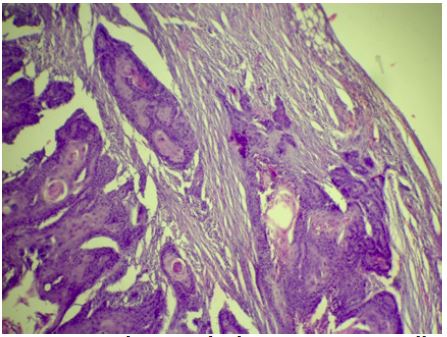
Figure 1: Microphotograph showing a cystic wall with a carcinomatous proliferation of squamous nature composed of lobules immersed in a fibro-inflammatory stroma (hematoxylin-eosin, magnification X 4).
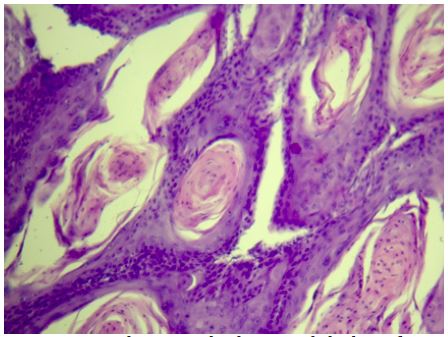
Figure 2: Microphotograph showing lobules of atypical squamous cells with central keratinization forming cornified globes (hematoxylin-eosin, magnification X 10).
Discussion
A cancerous mature teratoma is a dermoid cyst in which develops a cancer on one of the components of the cyst, the latter consisting mainly of a squamous epithelium, this degeneration occurs in 80% cases to squamous cell carcinoma [1-6]. It occurs between the ages of 50 and 60, in postmenopausal women (5.8). S.Y. rim et al. reported in one study a median age at diagnosis of 35.4 years for KDO versus 50.6 years for degenerate KDO [7-9]. However, the occurrence of a malignant transformation in young patients, especially in their forties is always possible, as in the case of our patient [9,10].
The clinical presentation varies according to the stage of the disease, but remains substantially similar to that of benign ovarian tumors, we will therefore find abdominal pain in the form of heaviness, abdominal distension, which can be very significant, or even signs of urinary or digestive compression.
On ultrasound, Uncomplicated dermoid cyst is most often a lucky find. Although their appearance is well known but often a source of trap, responsible for false positives and false negatives [11]. Typically 3 forms are described [12]: A cystic formation with a hanging echogenic nodule to its wall (Rokitansky's nodule); an attenuating echogenic mass. The posterior attenuations are secondary to the presence of hair, sebum thick within the lumen of the lesion, fat or ossified structures; or one cyst containing multiple linear echoes corresponding to floating hair in the lumen of the cyst. Alongside these classic shapes, another aspect can take on that of a seemingly banal cyst (serous content) or even a cyst presenting a liquid level. In addition, a transvaginal Doppler echo will show a flow greater intratumor blood and resistance and pulsatility indexes lower than non-cancerous ovarian KDOs, with a predictive value of 80% positive malignancy [13].
The diagnosis can therefore be suggested by ultrasound but must be confirmed by a CT scan or MRI, which will visualize an ovarian mass containing fat, a transmural extension, an invasion of neighboring structures, or the presence tumor necrosis and hemorrhage.
Another predictor of malignancy: Tumor size. Several studies have reported a median tumor size between 9.7 and 10 cm in case of degenerated KDO in squamous cell carcinomas [14,15]. As a general rule, a size greater than 10 cm should raise suspicion of malignant transformation.
The role of serum tumor markers is controversial, especially that SCC (Squamous Cell Carcinoma) antigens. In one study it was observed that ages over 40 and serum SCC antigen levels over 2.5 ng/ml predicted malignant transformation with 77% sensitivity and 96% specificity [16]. And in another that only 36.3% (4 out of 11) of transformations malignancies had a high serum level of SCC [9]. This marker is considered as useful for detecting a recurrence of the disease, when it will be high at the time of the initial diagnosis.
Therapeutic management of ovarian squamous cell carcinoma on Dermoid cyst is controversial, given the rarity of this pathology.
However, surgery remains a major therapeutic weapon in the treatment of these tumors. In the event of a stage IA tumour, in a woman wishing to pregnancy, conservative treatment, i.e. unilateral adnexectomy, can be considered. However, regular and prolonged monitoring of the patient is imperative.
For more advanced stages, complete surgery is the preferred strategy. adopt as for ovarian malignant epithelial tumors. In effect, several studies have shown that the quality of the surgical procedure makes it possible to improve significantly improved patient survival, with median survivals of 65 and 34.8 months (p=0.02) [17] and a 5-year survival of 79% and 10.1% respectively in cases of optimal and sub- optimal surgery (p=0.0001) [18]. Lymph node dissection remains controversial since the extensions are done step by step and by way peritoneal [19].
As for adjuvant treatment, there are currently no standards of protocol, but in front of such aggressiveness of these tumors one must consider after surgery platinum-based poly-chemotherapy, possibly followed by radiation therapy [20-22].
Chemotherapy alone has been tried in some cases and has had results variables. The BEP protocol (bleomycin, etoposide, cisplatin), considered as standard in germ cell tumours, is unsuitable for this histological type [20]. Paclitaxel, whose therapeutic responses in carcinomas are known epidermoids in general (cervical, ENT, pulmonary, etc.), as well as in the treatment ovarian malignant epithelial tumors, could be effective in this entity.
In case of peritoneal carcinomatosis or incomplete surgery, treatment with platinum more paclitaxel seems to be the best option [21]. Pelvic radiotherapy alone, delivered after surgery, even in the stages advanced, seems ineffective and even deleterious, giving rise to morbidity important [21,22].
A study published in 2007 showed a potential benefit of radiochemotherapy concomitant Cisplatin-based medication weekly for patients whose tumors are stage I or II. The rational was based on the fact that a carcinoma squamous cell (which is a radiosensitive tumour) can be treated similarly to a squamous cell carcinoma of the cervix or vulva, which it looks more like than an ovarian epithelial tumor [14].
Ovarian degenerated dermoid cysts have a poor prognosis [17,23,24]. With an overall 5-year survival ranging from 50 to 75% for stage I, 25% for stages II, 12% for stages III and 0% for stages IV [23-25].
Poor prognostic factors are young age, tumor stage, intraoperative tumor rupture, and incomplete surgery [26]. Our patient moreover made a very early recurrence, probably due to the fact that the tumor is ruptured in the abdomen.
Conclusion
Malignant transformation of ovarian dermoid cysts is a pathology rare but extremely aggressive. It must be suspected in front of a tumor very large ovary, in a postmenopausal woman, even if more and more more publications report cases occurring in young women. We currently lacks standards in the therapeutic management of these tumours, however surgery remains the cornerstone of treatment. In all the case, the therapeutic decision and the treatment must be multidisciplinary.
References
- Audebert A. Kystes de l’ovaire de l’adolescente. en Medecine de la Reproduction. Gynecologie Endocrinologie. 2013; 15: 378-386.
- F Demont, F Fourquet, M Rogers, J Lansac. Epidemiologie des kystes de l’ovaire apparemment benins. Journal de Gynecologie Obstetrique et Biologie de la Reproduction. 2001; 30.
- D Griffiths, J Wass, K Look, G Sutton. Malignant degeneration of a mature cystic teratoma five decades after discovery. Gynecol Oncol. 1995; 59: 427-429.
- F Wei, Z Jiang, C Yan. Analysis of 20 mature ovarian cystic teratoma cases in postmenopausal women. Chin Med J Engl. 2001; 114: 137-138.
- S Tangjitgamol, S Manusirivithaya, C Sheanakul, S Leela- hakorn, T Thawaramara, et al. Squamous cell carcinoma arising from dermoid cyst: case reports and review of literature. Int J Gynecol Cancer. 2003; 13: 558-563.
- Appareil genital feminin. Sebastien Henno. Memento de pathologie, 2017; 5: 232-233.
- AL Contreras, A Malpica. Angiosarcoma arising in mature cystic teratoma of the ovary: A case report and review of the literature. Int J Gynecol Pathol. 2009; 28: 453-457.
- X Argoitia, I Duga, E Labeyrie, L Toledo, C Couteau, et al. Degenerescence des kystes dermoïdes : A propos d’un cas de transformation maligne. Obstetrique & Fertilite. 2007; 35: 1005-1008.
- SY Rim, SM Kim, HS Choi. Malignant transformation of ovarian mature cystic teratoma. Int J Gynecol Cancer. 2006; 16: 140-144.
- La transformation maligne des kystes dermoïdes de l’ovaire : A propos de deux cas et revue de la litterature. I. Elghissassi, G. Belbaraka, H. Inrhaoun, C. Lhomme, H. Errihani. La Lettre du Cancerologue. 2011; 10.
- Y Ardaens, B Guerin du Masgenet, Coquel. Echographie en pratique gynecologique. Masson, collection d’imagerie medicale-Diagnostic. 2001.
- B Damarey, MO Farine, D Vinatier, P Collinet, JP Lucot, et al. Journal de Radiologie. Teratomes ovariens matures et immatures : Caracteristiques en echographie. 2010; 91:27-36.
- M Emoto, H Obama, S Horiuchi, T Miyakawa, T Kawara- bayashi. Transvaginal color Doppler ultrasonic characteri- zation of benign and malignant ovarian cystic teratomas and comparison with serum squamous cell carcinoma antigen. Cancer. 2000; 88: 2298-2304.
- L Dos Santos, E Mok, A Iasonos, K Park, Robert AS, et al. Squamous cell carcinoma arising in mature cystic teratoma of the ovary: A case series and review of the literature. Gynecol Oncol. 2007; 105: 321-324.
- Y Yamanaka, Y Tateiwa, H Miyamoto, Y Umemoto, Y Takeuchi, et al. Preoperative diagnosis of malignant transformation in mature cystic teratoma of the ovary. Eur J Gynaecol Oncol. 2005; 26: 391-392.
- Y Mori, H Nishii, K Takabe, H Shinozaki, N Matsumoto, et al. Preoperative diagnosis of malignant transformation arising from mature cystic teratoma of the ovary. Gynecol Oncol 2003; 90: 338-341.
- C Tseng, H Chou, K Huang, TC Chang, CC Liang, et al. Squamous cell carcinoma arising in mature cystic teratoma of the ovary. Gynecol Oncol. 1996; 63: 364-370.
- F Kikkawa, H Ishikawa, K Tamakoshi, A Nawa, N Suganuma, et al. Squamous cell carcinoma arising from mature cystic teratoma of the ovary: a clinicopathologic analysis. Obstet Gynecol. 1997; 89: 1017-1022.
- F Kornreich, J Holt, A Barnard, J Snoeck, J Kramer, et al. Comparison of Frank’s and McFee’s lead systems using multivariate statistics. Eur J Cardiol. 1976; 4: 131-140.
- Lee YC, Abulafia O, Montalto N, Holcomb K, Matthews R, et al. Malignant transformation of an ovarian mature cystic teratoma presenting as a rectal mass. Gynecol Oncol. 1999; 75: 499-503.
- Stamp GW, McConnell EM. Malignancy arising in cystic ovarian teratomas. A report of 24 cases. Br J Obstet Gynecol. 1983; 90: 671-675.
- Ribeiro G, Hughesdon P, Wiltshaw E. Squamous carci-noma arising in dermoid cysts and associated with hyper-calcemia: A clinicopathologic study of six cases. Gynecol Oncol. 1988; 29: 222-230.
- Peterson WF. Malignant degeneration of benign cystic teratomas of the ovary: a collective review of the literature. Obstet Gynecol. 1957; 12:793-830.
- Pins MR, Young RH, Daly WJ, Scully RE. Primary squamous cell carcinoma of the ovary. A report of 37 cases. Am J Surg Pathol. 1996; 20: 823-833.
- Kashimura M, Shinohara M, Hirakawa T, Kamura T, Matsukuma K. Clinicopathologic study of squamous cell carcinoma of the ovary. Gynecol Oncol. 1989; 34: 75-79.
- Sakuma M, Otsuki T, Yoshinaga K, Utsunomiya H, Nagase S, et al. Malignant trans-formation arising from mature cystic teratoma of the ovary: a retrospective study of 20 cases. Int J Gynecol Cancer. 2010; 20: 766-771.
