
Open Access, Volume 9
Unusual pararectal mass
Béatrice Akiki1*; Samah El Naderi1,2; Joe El Khoury3; Claude Ghorra1
1Department of Anatomical Pathology, Lebanese University-Faculty of Medicine, Lebanon.
2Department of Anatomical Pathology, Lebanese Hospital Geitaoui, Lebanon.
3Department of Medical Imaging of the Interventional Therapeutic Division, Lebanese University-Faculty of Medicine, Lebanon.
Beatrice Akiki
Department of Anatomical Pathology, Lebanese University-Faculty of Medicine, Lebanon.
Email: beatrice.akiki@gmail.com
Received : May 04, 2023,
Accepted : June 26, 2023
Published : June 30, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Signet ring cell morphology associated with neuroendocrine neoplasms is an extremely rare occurrence. Only a few cases have been reported in the English literature, all of them associated with neuroendocrine tumors. We herein report a case of neuroendocrine carcinoma with signet ring cells in an 81-year-old man, with a review of the literature. This association of signet ring cell morphology with a neuroendocrine neoplasm is important to know in order to reach an accurate diagnosis.
Keywords: Neuroendocrine neoplasms; Signet ring cell; Prostatic adenocarcinoma; Neuroendocrine carcinoma; Unknown primary.
Abbreviations: Neural Cell Adhesion Molecule; CDX2: Caudal-Type Homeobox Transcription Factor 2; PSA: Prostate Specific Antigen; MIB1: MIB E3 Ubiquitin Protein Ligase 1; INSM1: Insulinoma-Associated Protein 1; Minens: Mixed Neuroendocrine/Non Neuroendocrine Neoplasms.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Akiki B (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Akiki B, Naderi SE, Khoury JE, Ghorra C. Unusual pararectal mass. Open J Clin Med Case Rep. 2023; 2062.
Introduction
Neuroendocrine neoplasms of unknown primary origin are uncommon, with most of these neoplasms arising from a clinically undetected primary site. Morphological features help identify neuroendocrine differentiation which is then confirmed with immunohistochemical workup. Classically, signet ring cell appearance is associated with adenocarcinomas. Tumors displaying simultaneously both morphologies are uncommon and can raise a number of differential diagnoses.
Case Presentation
An 81-year-old man with a previous history of prostatic adenocarcinoma, diagnosed and treated 2-years prior, presents with an invasive left pararectal mass. A fine needle biopsy of this mass was performed and sent for histological analysis.
Microscopic examination showed a largely necrotic tumor consisting of nests and trabeculae of medium- to large- cells, often exhibiting a signet ring appearance (Figure 1A). The cells had finely stippled chromatin and inconspicuous nucleoli. Mucin stain was negative (Figure 1B). The immunohistochemical study revealed the expression of pan-cytokeratin as well as synaptophysin, chromogranin A and CD56 (Figure 2) by tumor cells. Anti-CDX2 and anti-PSA were negative. The proliferation index (MIB-1) was evaluated to 60%.
Based on the morphological appearance and immunohistochemistry results, a diagnosis of neuroendocrine carcinoma with signet ring cells morphology was made.
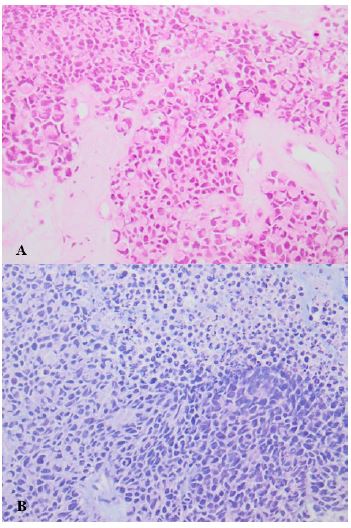
Figure 1: Drawings in 6 to 9 months after UCBC therapy.
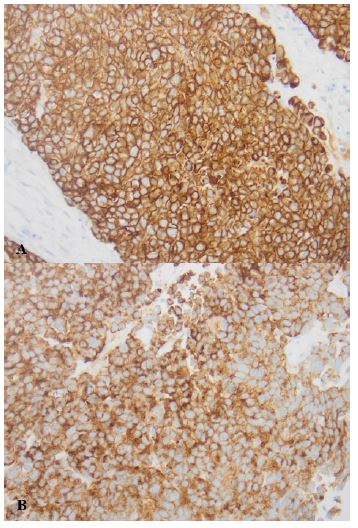
Figure 2: Immunohistochemical stain showing expression of pan-cytokeratin (A) and synaptophysin (B) by tumor cells.
Discussion
The diagnosis of neuroendocrine neoplasms is usually suggested in the presence of architectural and cytological characteristics, in particular an organoid architecture and a “salt and pepper” chromatin. Neuroendocrine markers, including INSM1, chromogranin A, synaptophysin, and CD56, confirm the neuroendocrine nature of the proliferation. Once the diagnosis is made, these neoplasms are further separated into well-differentiated neuroendocrine tumors and poorly differentiated neuroendocrine carcinomas, based on their differentiation. Next, neuroendocrine tumors are separated into three grades, by measuring proliferation, either by mitotic count and/or Ki-67 index assessment [1]. Neuroendocrine carcinomas are by definition a high grade proliferation.
Signet ring cell appearance is classically associated with adenocarcinomas. Although this scenario works in most cases, it is important to be aware that this morphology is not restricted to adenocarcinomas. It can be observed in other types of malignant tumors such as melanomas, germ cell tumors, and occasionally in neuroendocrine neoplasms [2].
Neuroendocrine neoplasms with signet ring cell appearance are characterized by the presence of intracytoplasmic vacuoles negative for mucin stains. These vacuoles correspond in electron microscopy to intermediate filaments, and stain positive with cytokeratin [3]. This unusual morphological appearance has been described in well-differentiated neuroendocrine tumors from different locations, most often arising in the appendix [4], and less often, they involve the gallbladder, the lung, the liver, and the pancreas [3]. In the appendix, they usually occur in young patients and are associated with a good prognosis [5]. In the liver, a total of seven cases of signet ring cell-appearing neuroendocrine tumors have been described in the literature [2,3,6,7]. They are associated with slow progression and no recurrence or development of metastasis after resection. On the other hand, the clinical evolution of this morphological appearance is aggressive in the pancreas [3]. The prognosis of neuroendocrine signet ring cell tumors of the gallbladder remains poorly known, given the presence of a single case reported in the literature.
In regard to the location and the clinical history of the case we report, a number of hypothesis should be considered regarding the origin of the neoplasm:
1. Localization of a lower gastro-intestinal tract neuroendocrine neoplasm: the negative CDX2 expression by the tumor cells does not favor this diagnosis.
2. The recurrence of a prostatic neuroendocrine missed component: in this case we should see coexpression by tumor cells of PSA and neuroendocrine markers. To note that a loss of PSA expression has been reported after treatment. By elimination, this diagnosis has been retained.
Conclusion
It is interesting to note, that signet ring cell morphology, classically attributed to adenocarcinomas, poses significant diagnostic challenges. To date, there have been no reported cases in the literature of neuroendocrine carcinoma with signet ring cell appearance in any location. Recognition of this morphological variant of neuroendocrine carcinoma is important. This distinction has therapeutic consequences, and pathologists should be aware of this entity.
References
- Rindi G, Moch H, McCluggage WG, Travis WD, Osamura RY, et al. Neuroendocrine neoplasms in non-endocrine organs. In: WHO Classification of Tumours Editorial Board. Endocrine and neuroendocrine tumours. Lyon (France): International Agency for Research on Cancer. 2022.
- Madakshira MG, Radotra BD, Singh V. Signet ring: A rare morphology of metastatic neuroendocrine tumor. Indian J Pathol Microbiol. 2019; 62: 335-336.
- Zhu H, Sun K, Ward SC, Schwartz M, Thung SN, et al. Primary hepatic signet ring cell neuroendocrine tumor: A case report with literature review. In: Seminars in Liver Disease. © Thieme Medical Publishers; 2010; 422-428.
- Kim JY, Hong SM, Ro JY. Recent updates on grading and classification of neuroendocrine tumors. Ann Diagn Pathol. 2017; 29: 11-16.
- La Rosa S, Uccella S. Classification of neuroendocrine neoplasms: lights and shadows. Rev Endocr Metab Disord. 2020.
- Haq S, Batra VV, Majumdar K, Javed A, Agarwal AK, Sakhuja P. Signet ring cell neuroendocrine tumor liver with mesenteric metastasis: Description of a rare phenomenon, with literature review. J Cancer Res Ther. 2015; 11: 658.
- Bansal N, Satapathy B. Primary multifocal cystic signet ring neuroendocrine tumor of liver: A case report. J Liver Cancer. 2021; 21: 187-193.
