
Open Access, Volume 9
Compound odontome associated with maxillary anterior region
Pooja Nagpal*; GuruPrasad R; Neeta Sharma; Shruti Pathania; Deeksha Sharma
Department of Oral Medicine and Radiology, HP Government Dental College, Shimla, India.
Pooja Nagpal
Department of Oral Medicine and Radiology, HP Government Dental College, Shimla, India.
Tel: 9599808871;
Email: nagpalpooja2018@gmail.com
Received : May 01, 2023,
Accepted : June 22, 2023
Published : June 30, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Odontomas are benign tumors of odontogenic origin. They are small in size and mostly seen solitary which can be diagnosed on routine radiographic examination. Morphologically, they are classified into complex and compound type. Early diagnosis and removal of odontomas is necessary to prevent their interference with the eruption of teeth. This article describes the case of an eight year old boy with compound odontome in the anterior maxilla which was surgically removed.
Keywords: Odontomas; Diagnosis; Teeth.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Nagpal P (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Nagpal P, Guru Prasad R, Sharma N, Pathania S, Sharma D. Compound odontome associated with maxillary anterior region. Open J Clin Med Case Rep. 2023; 2061.
Introduction
Odontomes are benign tumors which show completely differentiated epithelial and mesenchymal cells, making them odontogenic in origin. Structure resembling tooth is found i.e enamel, dentin and pulp tissue in varying proportions and degrees of development. According to WHO, the classification of odontomes include: Ameloblastic fibro-odontome, odontoameloblastoma, complex and compound odontomes [1].
Compound odontoma is a type of benign tumor, consisting of odontogenic tissue with an orderly pattern. It is formed of unilocular conglomerate of multiple tooth like structures. Some specialists consider this tumor to be included in the category of supernumerary teeth. The etiology of the odontoma is unknown, but there could be some association with trauma to deciduous teeth, inflammatory and infectious processes, hereditary anomalies and genetic mutations [2].
The incidence of compound odontome is 9 to 37% with a common predilection for females. Compound odontomas are most frequently found in the anterior region of the maxilla but they can also be localized in the other parts of dental arches. They generally do not present any symptoms and have a slow, non-aggressive and painless growth. In majority of the cases, bony expansion is observed. Over retention of deciduous teeth, impacted permanent teeth and sometimes malposition of adjacent teeth may also indicate presence of compound odontome. It is most commonly discovered in relation to a missing tooth, or by routine radiography [3,4].
Radiographically, odontoma shows a characteristic feature, i.e., a radiopaque mass suggestive for multiple small calcified structure that resemble to mini-teeth, surrounded by a radiolucent zone.
Odontomas are surgically removed and if needed with additional dental treatment e.g., orthodontic traction for included tooth. Recurrence of an odontome is quite rare but can occur in cases where it is removed in the early stage of its formation [3].
Case Presentation
A patient aged 8 years reported to Dept. of Oral Medicine and Radiology complaining of missing teeth in upper front tooth region since 2 years following shedding of deciduous teeth. Patient did not report of any infectious or inflammatory diseases or hereditary anomalies but had a history of trauma to anterior maxilla and nose 2 years back as a result of fall from stairs.
Extraorally, there were no significant findings (Figure 1). Intraorally, patient had mixed dentition with missing maxillary incisors but had slight elevation of left anterior alveolar ridge in the region of left maxillary central incisor (Figure 2a and 2b). Provisionally it was diagnosed as an odontome in maxillary anterior region.
Differential diagnosis include hypertrophied alveolar mucosa/ supernumerary tooth/ mesiodens, delayed eruption of incisors due to hypothyroidism/ ankylosis/ hypophosphatemia/ secondary to developmental defects such as dilacerations/ Ossifying fibroma or Periapical osseous dysplasia.
On radiographic investigation, IOPAR (Figure 3) and maxillary occlusal radiograph (Figure 4) revealed well defined radio-opacity superimposing normal radio density of right maxillary central incisor. In addition to above radiographic findings, OPG (Figure 5) also showed that the maxillary right lateral incisor was missing. After assessment of axial and coronal sections of CBCT of maxillary anterior region (Figure 6a, 6b, 6c. 6d, 6e), it was found that there was expansion and thinning of labial cortices of left maxillary central incisor. There was no radiographic evidence of root resorption of adjacent teeth. The root of right central incisor was dilacerated and curved with diffuse periapical rarefaction. At the area of maximum concavity, a well defined radio opaque mass was evident in the midline attached at CEJ of right maxillary central incisor (11) suggestive of odontome attached with the tooth. As a treatment plan, extraction of 11 along with the odontome was advised. After the surgery, the patient was called for follow-up and within a month, partial eruption of left maxiallary central incisor (21) was seen (Figures 8,9).

Figure 1: Extra oral front view of the patient.
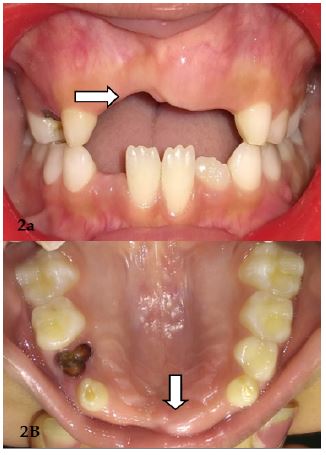
Figure 2: (A) Showing the teeth in occlusion.
(B) Showing maxillary arch.

Figure 3: IOPA reveals well defined Radio-opacity superimposing normal radio density of tooth w.r.t. 11, Incisal edge of 21 above the incisal level of 11 and partially visible 53.

Figure 4: Maxillary occlusal radiograph shows Well defined radio opacity superimposing the radiodensity of tooth w.r.t.11, Occlusal surfaces of 53,54,55,16,63,64,65,26 are evident and well defined radio-opacity resembling the normal radiodensity of crown portion of 21,22,13,14.
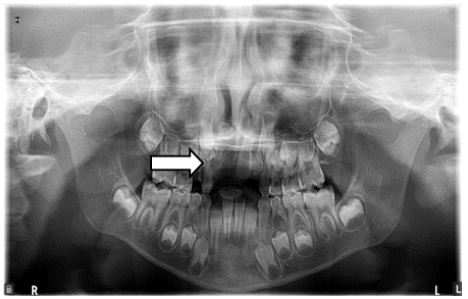
Figure 5: OPG shows well defined radio opacity with cortical border superimposing the radiodensity of 11. Incomplete apex w.r.t. 21,16,26,36,46, Crown with 2/3rd root formation w.r.t. 22, Crown formation with 1/3rd root formation w.r.t. 13,23, Crown completeion w.r.t. 14,17,24,25,27,33,34,43,44, ½ of crown completeion w.r.t. 15,35,45,37,47 and Radiographically missing 12.

Figure 6: Occlusal surfaces of teeth w.r.t. 11,13,14,53,54,55,16,21,22,23,63,64,65,26. After assessment of axial and coronal sections, Root completion with open apex w.r.t. 11, Radiographically missing 12, Crown completion with 1/3rd root formation of 13, Crown completion w.r.t. 14, ½ crown formation w.r.t. 15, Open apex w.r.t. 21 inclined labially and mesially, Expansion and thinning of labial cortices w.r.t. 21 and No radiographic evidence of root resorption of adjacent teeth or any other pathology noted.

Figure 7: (a) Intra-operative view. (b) Shows gross specimen.

Figure 8: Follow up after 1 month: Eruption of 21 seen.

Figure 9: Post-operative maxillary occlusal radiograph.
Discussion
Most common benign odontogenic tumors of epithelial and mesenchymal origin and second most common benign tumors of oral cavity are odontomas. They are also considered as hamartomas of interrupted tooth formation which account for 22% of the odontogenic tumors. This case report presents a compound odontome. Compound odontome is the malformation in which all dental tissues are represented in an orderly pattern so the lesion appears as a tooth-like structure. They can present as well-defined shaped, solitary or multiple denticles, bizarre, irregular shaped teeth and show anatomic resemblance to a normal tooth. They are formed of enamel and dentin, can also have variable amounts of cementum and pulpal tissue [1,3].
WHO classification of odontome
1. Ameloblastic fibro-odontome: Consists of varying amounts of calcified dental tissue and dental papillalike tissue, the latter component resembling fibroma.
2. Odonto-ameloblastoma: Its a very rare neoplasm which resembles an ameloblastoma both structurally and clinically but contains enamel and dentine.
3. Complex odontome: When the calcified dental tissues are simply arranged in an irregular mass bearing no morphologic similarity to rudimentary teeth.
4. Compound odontome: Composed of all odontogenic tissues in an orderly pattern that results in many teeth-like structures but without morphologic resemblance to normal teeth [1].
Gravey et al classified compound odontome as:
a) Denticulo type - composed of two or more separate denticles, resembling tooth like structure
b) Particulate type – has more than one separate masses, does not resemble tooth, consists of hard dental tissues
c) Denticulo-particulate type - This type shows the presence of both denticles and particles [4].
Odontomes commonly involve the anterior segment of maxilla and can also be located in maxillary sinuses, pituitary region, subcondylar region or ramus of the mandible. They are rarely reported in primary teeth. Clinically, they are usually asymptomatic, but sometimes consist of unerupted or impacted teeth, retainted deciduous teeth, swelling or evidence of infection. They can also displace adjacent teeth and cause malocclusion. Compound odontomes seldom cause bony expansion. The diagnosis is mainly done by routine radiographs [5,6].
Early diagnosis of odontomas helps us to:
(1) Have a less complex and less expensive treatment.
(2) Ensure better prognosis.
(3) Avoid relapse of the lesion.
(4) Avoid displacement or devitalisation of adjacent tooth.
Odontomas are either well organized/ malformed/ tooth like structures or denticles of varying size and shape, surrounded by a narrow radiolucent zone. Treatment is done by surgical removal of odontome and if needed, the associated tooth is also extracted [1,7].
The recurrence of the odontome is rare once it is enucleated, but close monitoring of children’s dentition is recommended. Consistent and regular follow-up of such cases is required to assess the eruption of the unerupted tooth [5,8].
Conclusion
It is important to correlate clinical and radiographic findings along with signs and symptoms for the diagnosis of an odontome. Early identification of odontomas prevents uneventful eruption of the permanent teeth/physiologic eruption of the impacted permanent tooth, ensuring minimal complication in the treatment and better prognosis.
Clinical significance
Undetected/long standing odontomas have predisposition to cystic changes due to the presence of various tooth formulations and can interfere with tooth eruption. Their early removal allows the impacted tooth to continue with the physiological eruption. Greater emphasis should be given on routine dental check-ups for children especially if there is any deviation in the eruption of teeth observed. So these anomalies can be detected earlier, thereby minimizing the interventions needed after enucleation.
Conflict of interests: There is no conflict of interests regarding this paper.
References
- Satish V, Magnaur C, Sharma R. Odontome: A brief overview international journal of clinical pediatric dentistry. 2011; 4.
- Shetty RM , Halawar S, Reddy H, Rath S. A complex odontome associated with maxillary impacted permanent central incisor; a case report. INT J Clin Pediart Dent. 2013; 6: 59-61.
- Shteryer A, Taicher S, marmary T. Odontoma in the subcondylar region. Br J oral surg. 1979; 17: 161-165.
- Morawala Abdul, Kapila Pragati, Chunawala Yusuf, “Compound Composite Odontoma and Its Management”, Case Reports in Dentistry. 2014; 2014: 4.
- Smitha M, Paul ST, Bagga V. Surgical Management of Compound Odontome Associated with Impacted Canine: A Case Report. Journal of South Asian Association of Pediatric Dentistry. 2019; 2.
- Uma E. Compound Odontoma in Anterior Mandible-A Case Report. Malays J Med Sci. 2017; 24: 92-95.
- Oliveira BH, Campos V, Marçal S. Compound odontoma-diagnosis and treatment: three case reports. American Academy of Pediatric Dentistry. 2001; 23: 2.
- LAN Santos, LJ Lopes, GD Roque-Torres, VF Oliveira, DQ Freitas. “Complex Odontoma: A Case Report with Micro-Computed Tomography Findings”, Case Reports in Dentistry. 2016; 2016: 6.
