
Open Access, Volume 9
A case series of spindle cell neoplasm of extremities
Bikram Kar*; Ankit Kumar Garg; Shubham Bhardwaj; Rudra Narayan Dash
National Agri-Food Biotechnology Institute (NABI) Mohali, Punjab, India.
Bikram Kar
National Agri-Food Biotechnology Institute (NABI) Mohali, Punjab, India.
Email: bhardwajshubham15081995@gmail.com
Received : April 24, 2023,
Accepted : June 12, 2023
Published : June 20, 2023,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kar B (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kar B, Garg AK, Bhardwa S, Dash RN. A case series of spindle cell neoplasm of extremities. Open J Clin Med Case Rep. 2023; 2055.
Introduction
A soft tissue sarcoma is a heterogeneous group of neoplasms that predominately arise from cells of embryonic mesoderm, i.e., connective tissue, muscle, joints, fat, blood vessels, and peripheral nerves. Spindle cell neoplasm arises from the mesenchymal cells, which form the body’s connective tissue system. These cells include neural, fibroblastic, myofibroblast, epithelial, or vascular tissue. Spindle cell sarcomas are usually deep-seated lesions arising from major nerves along the extremity with a preponderance of local recurrence [1].
Fibromatosis is a benign tumour of fibroblastic and myo-fibroblastic cells. It can occur as a superficial or deep form (desmoid tumour). Deep fibromatosis can be abdominal (occurs in the anterior abdominal wall or rectum), extra-abdominal (extremities, thorax, or the head and neck region), and intraabdominal fibromatosis (mesentery or intrapelvic space). Extra abdominal fibromatosis is common in patients between puberty and 40 years of age, with female predominance. These tumours usually do not metastasize, but local infiltration and compression to surrounding vital structures are common [2-6].
We present a case series of four patients with fibromatosis treated with wide local excision and good functional outcome with no recurrence in follow-up.
Case Presentation
Case 1: A 15 years old male was admitted with complaints of pain and swelling in his right arm for 1.5 years without any history of antecedent trauma. The swelling was insidious in onset and gradually progressed to become present size. On examination, there was a non-mobile, non-fluctuant, and non-pulsatile swelling of 8 x 6 cm in size over the anterolateral aspect of the right arm with a smooth surface, firm consistency, and irregular margins. The overlying skin was normal and non-adherent to underlying structures. There were no clinical signs of radial nerve entrapment.
CT of the right arm showed a large mildly hypodense soft tissue lesion in the anterolateral aspect of the right arm involving muscular and intermuscular plane with no oblivious interosseous extension or osseous erosion. MRI of right arm showed lobulated altered signal intensity lesion of size 63 x 41 x 84 mm (AP*TR*CC) in the lateral aspect of mid-arm involving deltoid and triceps muscle with few enlarged axillary lymph nodes. The lesion appeared to be a hypointense lobulated lesion with multiple flow voids within and hyperintense on T2WI/STIR. The MRI features were suggestive of soft tissue neoplasm of mesenchymal origin with differential diagnosis of round cell neoplasm and myositis ossificans.
PET-CT was suggestive of FDG avid soft tissue density in the lateral aspect of the right mid-arm involving mid-arm muscles sparing the underlying bone and overlying skin with ipsilateral axillary lymph node involvement.
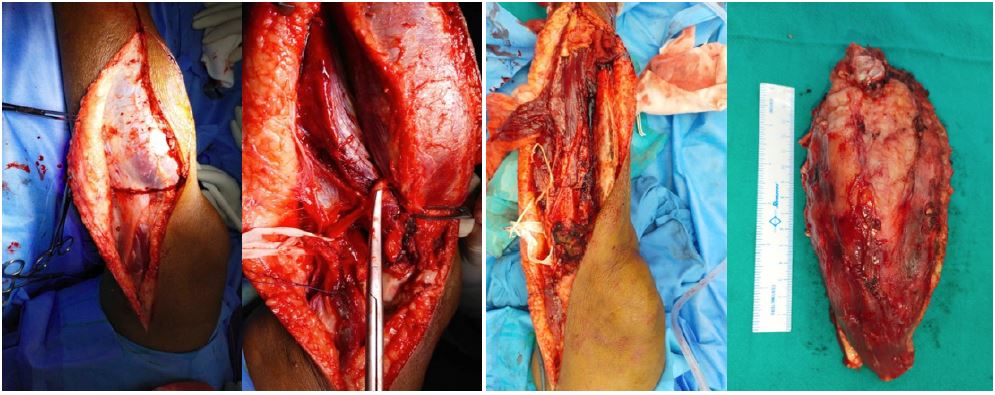
After obtaining consent regarding possible radial nerve palsy, the patient was taken for surgery. Using the posterior approach to the arm, wide excision of the tumour was done after protecting the radial nerve. The tumour was excised with wide tissue margins confirmed by a frozen section biopsy. The tumour and a few pieces from the deltoid, triceps, brachioradialis, and a few pieces of periosteum obtained from the humerus shaft were sent for histopathological examination.
Histopathological examination was suggestive of spindle cell neoplasm consistent with fibromatosis. Periosteum and all muscle pieces were found to be uninvolved by tumour cells. All the margins were tested negative. Tumour cells were S-100 negative, desman negative, SMA positive, and CD34 negative with Ki67 -1-2 %.
The immediate postoperative period was uneventful. The patient was followed up regularly at two-monthly intervals for twelve months.

MRI of the right arm

Intraoperative images

Clinical images in follow-up.
Case 2: A 25-year male presented with swelling over the right forearm, insidious onset, gradually progressive, and painless. The swelling was in the anterior aspect of the right proximal forearm, non-tender, and not fixed to underlying bone or overlying skin. MRI revealed an ill-defined cystic lesion involving the right proximal forearm's central and medial intermuscular plane. A core-needle biopsy was suggestive of fibro-myxoid sarcoma.
After obtaining consent, the patient was taken for surgery. A wide local resection was planned. However, since the mass was involving both the compartment with interosseus extension, local excision was not possible. Hence, above elbow amputation has been done. Histopathological examination was suggestive of spindle cell neoplasm consistent with fibromatosis. All the margins were tested negative. Tumour cells were S-100 negative, desman negative, SMA positive, and CD34 negative with Ki67 -1-2 %.
The immediate postoperative period was uneventful. The patient was followed up regularly at two-monthly intervals for twelve months.

Clinical images in follow-up.

Preoperative clinical images
Case 3: A 13-year male presented with a swelling at the posteromedial aspect of the right thigh, which was insidious in onset, and gradually progressive. He had a history of weight loss. On examination, a non-tender firm swelling was palpated in the proximal thigh's posterior aspect, which was not fixed to underlying bone or overlying skin.
MRI was suggestive of soft tissue neoplasm involving the posterior compartment of the thigh with sciatic nerve involvement. PET CT did not show any distant metastasis.
A USG-guided needle biopsy was performed, and tissue was sent for histopathological examination. Histopathology reported spindle-shaped tumour cells arranged in sheets and swirling patterns with abundant myxoid stroma suggestive of low-grade fibro myxoid sarcoma.
The patient was taken for surgery with due consent for sciatic nerve injury, and a wide local excision was performed. The sciatic nerve was freed from the tumour proximally. On the distal aspect common peroneal nerve had to be sacrificed as the tumour completely invaded it. Histopathological examination of the resected tumour confirmed the diagnosis of low-grade fibro myxoid sarcoma.
Postoperatively patient had weakness of ankle dorsiflexion, but hip and knee range of motion was preserved. There was no recurrence at six months follow-up.

Intraoperative images

Postoperative clinical images with deficient ankle dorsiflexion
Case 4: A 42-year male presented with a slow-growing mass over his left calf, which he noticed nine months ago. The swelling originated insidiously without a history of trauma and gradually progressed in size. There was a localized swelling over the posterior aspect of the left leg on examination. There was no local rise in temperature or tenderness. The swelling was not fixed to underlying bone or overlying skin. The skin above the swelling was normal. Knee range of motion was within normal limits. Distal neurovascular status was normal.
MRI revealed a soft tissue neoplasm originating from the soleus. PET-CT showed no distant metastasis. Core-Needle biopsy showed fibro-myxoid sarcoma.
A wide local excision was performed with negative margins. The postoperative period was uneventful. There was no distal neurovascular deficit. There was no recurrence at the nine-month follow-up.
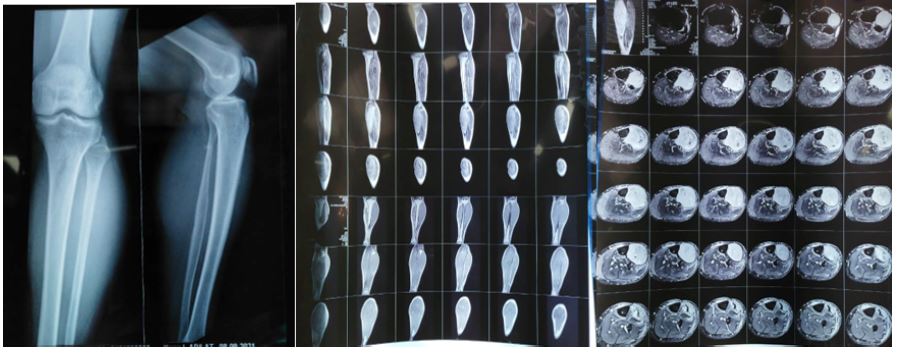
Radiological investigations
Radiological investigations
Discussion
Spindle cell neoplasm includes a broad spectrum of reactive tumour-like lesions to high-grade malignant tumours with a diverse clinical presentation. These tumours generally begin in layers of connective tissue such as under the skin, between muscles, and surrounding organs, forming a lump that grows gradually [7]. In the earlier stages, they are localized and usually do not spread beyond the encapsulated form, but they can also develop malignant potential, which is detected through microscopic examination. The incidence of these tumors is three in every 3.5 million with a 2:1 female: male predisposition. The various risk factors predispose to the development include a previous history of trauma/surgery or pregnancy exposure to ionizing radiation, lymphedema, and certain inheritable conditions, such as neurofibromatosis, Li–Fraumeni syndrome [7-9]. There was no identifiable risk factor in our patients, and all four patients were male.
It is essential to identify the cell of origin for spindle cell sarcoma using techniques like immunohistochemistry, electron microscopy, and molecular pathology to determine the biological potential of the lesions [10]. Historically, amputation was considered the treatment of choice in malignant lesions. Its use is limited to only a few cases where tumours cannot be resected due to the close proximity of neurovascular structures with limb salvage procedures [11]. However, now with the multimodal approach and radio-chemotherapy, the current goal of the treatment is to maximize the likelihood of long-term recurrence-free survival and provide an excellent functional restoration of the limb after resection [11].
The preferred treatment for limb extremity spindle cell sarcoma is wide local excision, including the biopsy site. The wide local excision includes 1-2 cm of the surrounding normal tissue and a narrower margin in case of uninvolved major critical neurovascular structures in the vicinity of the tumour. It may be supplemented by postoperative radiation therapy. Several studies suggest that a complete resection with tumour-free margins is essential to prevent recurrence [11].
We performed a wide resection of the tumour by taking negative margins from the adjacent tissue and preventing critical neurovascular structures. The resection was done carefully, taking negative margins and preventing injury to the radial nerve in case 1 and the peroneal nerve in case 4. However, in case 3, we had to sacrifice the common peroneal nerve as it had completely invaded the tumour. At one year follow-up, the functional outcome was satisfactory, and there was no recurrence in our patients.
Conclusion
Deep fibromatosis in extremities are relatively less common entity and can pose a therapeutic challenge due to its local aggressive and infiltrative nature. A prompt diagnosis, pre-op planning, and wide resection with negative margins can result in a good outcome with functional restoration of the limb.
References
- Duan Mingyue, Hua Xing, Keren Wang, Chunbo Niu, Chengwei Jiang, et al. A large and aggressive fibromatosis in the axilla: a rare case report and review of the literature. OncoTargets and Therapy. 2018; 11: 3179-3184.
- Surbhi, Metgud R, Naik S, Patel S. Spindle cell lesions: A review on immunohistochemical markers. J Can Res Ther. 2017; 13: 412-418.
- Meng, Guo-Zhao, Zhang, Hong-Ying, Bu, et al. Low-Grade Fibromyxoid Sarcoma Versus Fibromatosis: A Comparative Study of Clinicopathological and Immunohistochemical Features. Diagnostic cytopathology. 2009; 37: 96-102.
- Eric A. Walker, Jonelle M. Petscavage, Pamela L. Brian, Chika Iloanusi Logie, Kenneth M. Montini, et al. “Imaging Features of Superficial and Deep Fibromatoses in the Adult Population”, sarcoma. 2012; 17: 215810.
- Lacka DE, Nasierowska-Guttmejer A. Fibromatosis - immunohistochemical evaluation, differential diagnosis from gastrointestinal tumors, and other mesenchymal tumours. Prz Gastroenterol. 2019; 14: 79-85.
- Berner K, Johannesen TB, Hall KS, Bruland OS. Clinical epidemiology and treatment outcomes of spindle cell non-osteogenic bone sarcomas - A nationwide population-based study. J Bone Oncol. 2018; 14: 002-2.
- Sakorafas GH, Nissotakis C, Peros G. Abdominal desmoid tumors. Surgical Oncology. 2007; 16: 131-142.
- Altmann S, Lenz-Scharf O, Schneider W. Therapieoptionen bei der aggressiven fibromatose [Therapeutic options for aggressive fibromatosis]. Handchir Mikrochir Plast Chir. 2008; 40: 88-93.
- Ali Kaygin M, Dag O, Erkut B, Ates A, Kayaoglu RC, et al. Extra-abdominal fibromatosis (desmoid tumor): a rare tumor of the lower extremity arising from the popliteal fossa. Case Rep Vasc Med. 2011; 2011: 184906.
- Shaikh, Sohail, Katke, Rajshree, Raut, Soham. Spindle Cell Sarcoma Arising from Nerve Sheath Presenting as Huge Abdominal Mass. J Case Reports. 2014; 4: 232-235.
- Murray PM. Soft tissue sarcoma of the upper extremity. Hand Clin. 2004; 20: 325-333.
