
Open Access, Volume 9
Lingual abscess, an uncommon cause of tongue oedema: Case series
Anastasia Oikonomou; Methodios Stavridopoulos; Stavros Nikitopoulos; Georgia Tsiouma*
Otorhinolaryngology Department, General Hospital of Volos, Greece.
Tsiouma Georgia
Otorhinolaryngology Department, General Hospital of Volos, Greece.
Tel: +306977020468;
Email: gtsiouma@yahoo.gr
Received : April 24, 2023,
Accepted : June 07, 2023
Published : June 09, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Lingual abscess is a rare but potentially life-threatening medical entity. Consequently, it requires high medical suspicion in order to prevent misdiagnosis. Unilateral tongue oedema constitutes the characteristic clinical feature. In order to achieve a timely diagnosis, radiological imaging is often required as it provides essential information and facilitates the design of an appropriate treatment plan. Herein, we present two cases, one of a 52-year-old woman and another of a 32-year-old man, who complained of acute tongue swelling and were diagnosed with anterior lingual abscess, which was successfully treated with surgical drainage and systemic antibiotics.
Keywords: Tongue abscess; Lingual abscess; Drainage; Tongue swelling; Tongue oedema.
Abbreviations: hsCRP: high sensitivity C- Reactive Protein; CT: Computed Tomography; TIVA: Total Intravenous Anesthesia; WBC: White Blood Cell; MRI: Magnetic Resonance Imaging.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Georgia T (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Oikonomou A, Stavridopoulos M, Nikitopoulos S, Tsiouma G. Lingual abscess, an uncommon cause of tongue oedema: Case series. Open J Clin Med Case Rep. 2023; 2054.
Introduction
Few case reports of lingual abscesses have been published in English literature over the last years [1]. These articles are our main source of information regarding cause, pathogens, treatment techniques and mortality rate of tongue abscesses [2]. Despite the possibility of a compromised airway, that may require urgent tracheostomy, most cases resolve with surgical drainage and antibiotics [1,3]. The challenge when dealing with lingual abscesses resides in the timely diagnosis, which is based upon clinical manifestations and radiological findings.
Case Series
Case 1
A 52-year-old woman presented to the Emergency Department due to a 3-day history of unilateral swelling of the tongue, mild fever, dysphagia and dysphonia. She had been previously diagnosed with stomatitis by a General Practitioner and received prednisolone per os without improvement. The patient did not report any recent trauma, oral infection or dental procedure, was a non-smoker and had no history of alcohol consumption. Her medical history was unremarkable with the exception of an allergic reaction to amoxicillin/clavulanic acid and trimethoprim/sulfamethoxazole. The examination of the oral cavity showed obvious lingual swelling located on the left middle third of the tongue (Figure 1). Palpation or movement of the tongue caused severe pain to the patient. Her oral hygiene was poor but there was no sign of odontogenic inflammation. Rigid fiberoptic laryngoscopy revealed no pathology of the larynx or the base of the tongue. The laboratory tests showed leukocytosis, neutrophilia and elevated high sensitivity C- Reactive Protein (hsCRP). A Computed Tomography (CT) was performed and revealed a heterogeneous lesion with hypoattenuating borders in the left middle third of the tongue (Figure 2). The patient was hospitalized in the ENT Department and treated with clindamycin i.v. and anti-inflammatory agents, empirically. Drainage of the abscess was performed with a sublingual incision under Total Intravenous Anesthesia (TIVA). The pus culture revealed no bacteria. All the symptoms subsided within 48 hours. The patient was discharged after four days and advised to complete treatment with clindamycin per os.
Case 2
A 32-year-old male, with no previous medical history, was referred to the ENT Department due to lingual pain and oedema, which gradually worsened over the course of 48 hours. The patient was a non-smoker with no history of trauma and good oral hygiene. Palpation revealed a firm mass located in the anterior middle area of the tongue with spontaneous pus discharge streaming from its inferior surface. Rigid fiberoptic laryngoscopy revealed no pathology from the oropharynx and larynx. As for the laboratory tests, white blood cell (WBC) count and hsCRP were within normal rates, whereas the CT scan revealed soft tissue oedema of the middle line of the tongue with varying enhancement and air accumulation (Figure 3). The patient was admitted to the ENT Department and the abscess was drained under TIVA via an extension of the existing fistula (sublingual incision) (Figure 4). During hospitalization he received treatment with ampicillin/ sulbactam, metronidazole and anti-inflammatory agents i.v. empirically, as the pus culture obtained during surgery revealed no specific pathogen. The symptoms subsided after three days and the patient was discharged with oral antibiotic treatment.

Figure 1: Drawings in 6 to 9 months after UCBC therapy.
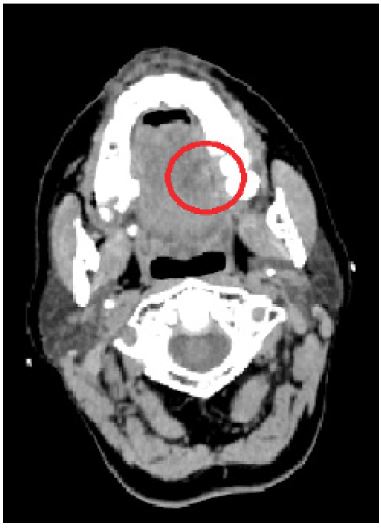
Figure 2: Cervical CT scan: lingual abscess indicated by the heterogeneous lesion with hypoattenuating borders (red circle).
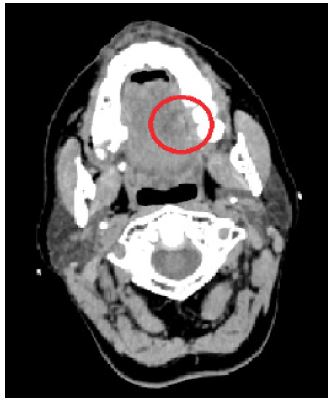
Figure 3: Cervical CT: midline tongue lesion of varying enhancement and air accumulation (red circle).

Figure 4: Intraoperative image after abscess drainage via sublingual incision.
Discussion
Tongue abscess is a rare medical entity. The anatomical structure of the tongue, which includes high vascularity, rich lymphatic supply, thick muscle and epithelium and the antibacterial agents of saliva, constitute the main protective mechanism against pathogens [1,4]. Several risk factors have been described in the literature such as foreign bodies of the tongue (e.g. fish bones), tongue piercing, poor oral hygiene, dental infections or procedures, oral infections, immunodeficiency, diabetes mellitus and heavy smoking [1, 2,5,6]. Even so, in many cases, including the ones presented in this study, no specific cause could be identified [7].
The clinical manifestations of lingual abscess include lingual swelling which is usually unilateral, tenderness upon palpation, limitation of tongue movement, referred otalgia, odynophagia, dysphagia, dysphonia, dyspnea and low-grade fever [2]. Diagnosis can be difficult, as demonstrated by our first case, in which the patient was mistakenly diagnosed as stomatitis in the first assessment. Lingual abscess may often be misdiagnosed as infected follicular lingual tonsils, thyroglossal duct cyst, neoplasm, arteriovenous malformation, angioedema, hematoma, acute epiglottitis or glossopharyngeal neuralgia [1,5,6].
The use of intraoral ultrasound has been proposed as a diagnostic means but CT and Magnetic Resonance Imaging (MRI) scans provide more detailed information especially in cases of abscess of the base of the tongue. MRI offers an advantage in the description of soft tissue anatomical structures of the oral cavity but is often time consuming or unavailable [3]. Needle aspiration of pus may also be diagnostic, especially in cases of anterior lingual abscesses, where it can be easily performed.
Standard treatment includes drainage and broad-spectrum antibiotics, initially empirically [2]. The most common microorganisms isolated from pus cultures are Streptococcus Spp. Staphylococcus Spp, Haemophilus Spp, Bacteroides Spp, Fusobacterium Spp and other anaerobic bacteria [1,2,5,8]. The antibiotic treatment can be altered afterwards according to pus culture isolates and their antibiotic sensitivity. Regarding surgical treatment, drainage of the abscess through lingual incision is the gold standard method. Needle aspiration of the abscess has also been reported with promising results, especially in patients who cannot undergo surgery due to severe comorbidities, provided that they remain in close follow-up [4,5]. In cases of lingual abscess of the base of the tongue, the initial approach is to secure the airway via intubation or tracheostomy [1,3].
Conclusion
Clinicians should consider the possibility of lingual abscess particularly in patients who present with acute unilateral tongue swelling. Especially, posterior lingual abscess requires high alert for potential airway obstruction. The standard treatment includes drainage via incision or aspiration and systematic antibiotics. Due to access to modern imaging techniques and antibiotics, mortality rate nowadays remains lower than 3% [2].
Declarations
Acknowledgements: All authors participated in the research design and writing of the paper.
Funding: The authors declare no funding.
Disclosure: The authors declare no conflicts of interest.
References
- Antoniades K, Hadjipetrou L, Antoniades V, Antoniades D. Acute tongue abscess. Report of three cases. Oral surgery, oral medicine, oral pathology, oral radiology, and endodontics. 2004; 97: 570-573.
- Srivanitchapoom C, Yata K. Lingual Abscess: Predisposing Factors, Pathophysiology, Clinical Manifestations, Diagnosis, and Management. International journal of otolaryngology. 2018; 2018: 4504270.
- Munoz A, Ballesteros AI, Brandariz Castelo JA. Primary lingual abscess presenting as acute swelling of the tongue obstructing the upper airway: diagnosis with MR. AJNR American journal of neuroradiology. 1998; 19: 496-498.
- Ozgur GT, Akdogan MV, Unler GK, Gokturk HS. A rare cause of acute Dysphagia: abscess of the base of the tongue. Case reports in gastrointestinal medicine. 2015; 2015: 431738.
- Balatsouras DG, Eliopoulos PN, Kaberos AC. Lingual abscess: diagnosis and treatment. Head & neck. 2004; 26: 550-554.
- Boon M, Pribitkin E, Spiegel J, Nazarian L, Herbison GJ. Lingual abscess from a grill cleaning brush bristle. The Laryngoscope. 2009; 119: 79-81.
- Bekele K, Markos D. Lingual abscess: a case report. International medical case reports journal. 2017; 10: 285-287.
- Vellin JF, Crestani S, Saroul N, Bivahagumye L, Gabrillargues J, Gilain L. Acute abscess of the base of the tongue: a rare but important emergency. The Journal of emergency medicine. 2011; 41: e107-10.
