
Open Access, Volume 9
Severe dysthyroid optic neuropathy following SARS-Cov-2 vaccination treated with tocilizumab: First two reported cases
Fatima Alalawi1; Ohood Almazroui2; Ahmed Alsaadi1; Habibullah Eatamadi2*
1Sheikh Khalifa Medical City, Abu Dhabi, United Arab Emirates.
2Sheikh Shakhbout Medical City, Abu Dhabi, United Arab Emirates.
Habibullah Eatamadi
Sheikh Shakhbout Medical City, Abu Dhabi, United Arab Emirates.
Tel: 00971501149112;
Email: Habibcornea@yahoo.co.uk
Received : April 17, 2023,
Accepted : June 02, 2023
Published : June 09, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Background: Thyroid eye disease is a condition that is mostly associated with Graves’ disease. It is an autoimmune condition that can have various clinical presentations and associations. Recently association of COVID-19 infection and/or vaccination with de novo occurrence of thyroid eye disease has been described. Our aim is to report two cases of new onset dysthyroid optic neuropathy after recent COVID-19 vaccination. These cases will describe their presentation, management, and the outcome following the treatment with tocilizumab.
Case report: We are reporting two cases who presented with severe thyroid eye disease and concurrent dysthyroid optic neuropathy following COVID-19 vaccination in the absence of active COVID-19 infection treated with tocilizumab injection. To our best knowledge, these are the first reported cases of dysthyroid optic neuropathy following the administration of different types of COVID-19 vaccines that were resistant to conventional treatment and favorably treated with intravenous tocilizumab.
Conclusion: COVID-19 vaccine related autoimmune thyroid eye disease is a well-documented condition. The correlation between COVID-19 infection and its vaccine with thyroid disease is currently being extensively investigated. Most probably it occurs as a result of immune system deregulation. The occurrence of dysthyroid optic neuropathy in thyroid eye disease is not frequent. The finding of dysthyroid optic neuropathy following COVID-19 vaccination and treatment with tocilizumab has not been reported in the literature. The clinicians must be aware of this association and educate patients to be monitored appropriately and treated when appropriate. However, this should not deter patients from getting proper and timely vaccination against the virus.
Keywords: COVID-19 vaccine; Graves ophthalmopathy; SARS-CoV-2.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Eatamadi H (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Alalawi F, Almazroui O, Alsaadi A, Eatamadi H. Severe dysthyroid optic neuropathy following SARS-Cov-2 vaccination treated with tocilizumab: First two reported cases. Open J Clin Med Case Rep. 2023; 2051.
Introduction
Thyroid Eye Disease (TED) is an autoimmune disorder associated in most cases with hyperthyroidism and less with euthyroid or hypothyroidism [1].
Ophthalmic manifestations can present in up to 50% of patients with Graves’ disease [1]. Symptoms are extremely variable and can range from mild to severe. The occurrence of dysthyroid optic neuropathy (DON) is rare [1]. and constitutes about 4% to 8% of all complications [2].
Treatment of TED has evolved in recent years from systemic steroids and other immunosuppressors to targeted biological therapies, for example, tocilizumab and teprotumumab [3].
Other autoimmune diseases can occur concomitantly with Thyroid eye disease. These include myasthenia gravis, type 1 diabetes mellitus, rheumatoid arthritis, vitiligo, Addison’s disease, and celiac disease [4]. Thyroid eye disease also can coexist or be triggered by other factors that affect the immune system of the body. Examples include smoking and stressful life event like grievance and divorce [5].
Since its start in late 2019, different types of vaccines have been developed and administered to tackle the pandemic. One widely used vaccine is BNT162b2 vaccine (Pfizer–BioNTech) that has been approved by FDA on Aug. 23, 2021 [6]. Another well-established vaccine is Oxford-AstraZeneca (AZD1222), approved for emergency use in the UK on December 30, 2020 [7].
The vaccination has been associated with relatively minor side effects, including pain at the injection site (71% of older recipients and 83% of younger recipients, after the first dose), as well as fatigue and headache (59% and 52%, respectively, within the younger recipients and 51% and 39% within the older recipients) [8]. It has also been associated with an elevated risk of immune-related reactions including Graves’ disease, myocarditis, immune thrombotic thrombocytopenia, Guillain– Barré syndrome, rheumatoid arthritis, and systemic lupus erythematosus [9,10]. Treatment of these complications depends on the nature and severity of the case [11-13].
Hereby we are reporting the characteristics and treatment of two cases of dysthyroid optic neuropathy following two different types of Covid vaccination.
To our knowledge, this is the first reported case of dysthyroid optic neuropathy following Covid 19 vaccination. Both cases were favorably treated with tocilizumab infusion following an unsuccessful response to a high dose of systemic steroid [14-16].
Case 1
A 55-year-old male, heavy smoker (1.5 packs a day for the past 18 years), with no previous history of hyperthyroidism and thyroid eye disease, presented with progressive right eye redness, pain, double vision, and severe exophthalmos. He had four doses of BNT162b2 vaccine (Pfizer–BioNTech) starting in May 2021, each one month apart. Shortly after receiving the third dose of the vaccine, his right eye started to slowly become exophthalmic, red, and uncomfortable. After taking the fourth dose, the right eye condition worsened dramatically with increasing redness, pain, double vision, and progressive exophthalmos. He was seen in another healthcare facility and was administered a full dose of intravenous steroid as per European Group of Graves Orbitopathy (EUGOGO), (6 doses of weekly 500 mg IV methylprednisolone followed by another six doses 250 mg of IV methylprednisolone) [17], with no improvement but rather deterioration of his eye condition.
On presentation to our facility, his best corrected visual acuity was 6/60 in the right eye and 6/7.5 in the left eye. Pupil examination showed right Relative Afferent Pupillary Defect (RAPD). External examination showed bilateral exophthalmos (mild in the left eye), upper eyelid retraction, redness, and edema with severe right lower eyelid entropion.
The right eye conjunctiva was injected and edematous with moderate inferior corneal punctate epithelial erosions and relatively clear central cornea.
The right eye was hypotropic in primary position, with minimal supraduction with restriction of abduction (-3) and adduction (-1) (Figure 1).
Dilated fundus examination showed normal bilateral optic nerves but prominent choroidal folds inferior to the right macula. His left eye examination was normal. Color vision was 11/17 in the right eye and 17/17 in the left eye. Hertel exophthalmometry measurements were 26mm OD and 21mm OS at a base of 120mm. No previous measurements are available for comparison as initially he was seen and treated in another facility.
Humphrey 24-2 visual fields displayed right eye inferior patchy visual field defect that was not respecting the vertical line (Figure 2).
Computed Tomography (CT) scan showed marked right inferior rectus muscle belly enlargement while sparing the tendons. The rest of EOM were enlarged but to a lesser extent. There was stretching of the right optic nerve with crowding of the orbital apex compared to the left side with a Barrett’s index of 64%. (Figure 3).
Laboratory testing showed euthyroid status including normal Thyroid-Stimulating Hormone (TSH) and normal free thyroxine (T3, T4). However, his thyroid stimulating immunoglobulins (TSI) were high (10.00 IU/L; N< 1.75 IU/L), as well as interleukin 6 (IL-6) level. (54.7 pg/mL; N< 7.0).
Further laboratory investigations were not significant. Based on the clinical and laboratory findings and upon consultation with the endocrinology team a diagnosis of euthyroid thyroid eye disease with DON was done. Due to insurance disapproval, the visual evoked potential was not performed. As the patient had not responded to systemic intravenous steroid treatment, a decision was made to start the patient on tocilizumab infusion after taking full consent.
The patient received 4 Tocilizumab infusions (8 mg/kg), each infusion one month apart. His final best corrected visual acuity was 6/9 OD and 6/6 OS and his RAPD had resolved. Exophthalmometry was 23 mm OD and 21 mm OS at a base of 120 mm (Figure 1). His color vision and visual fields returned to normal. Approximately 2 months following the fourth dose of Tocilizumab, the patient had recurrent signs and symptoms of DON in the right eye. His visual acuity in the right eye dropped to 6/24 with RAPD. His clinical activity score was at least 8 in the right eye. His laboratory investigations showed severe hypothyroid status, with markedly elevated TSH (98.800 milli IU/L; N>0.270<4.200), and low free T3 (1.49 pmol/L; N>3.10< 6.80) and free T4 (2.3 pmol/L; N>12.0< 22.0). He was started on 50 mcg levothyroxine. He received 2 more doses of Tocilizumab infusion (8 mg/kg), each infusion one month apart, following which his condition stabilized again, and his lab results returned back to normal.
Case 2
A 52 years-old-female non-smoker presented to our oculoplastic service with severe bilateral thyroid eye disease and signs and symptoms of right-sided dysthyroid optic neuropathy. Her hyperthyroidism started 10 years ago and she had partial thyroidectomy 3 years before presentation. Her thyroid status has been stable since then.
The patient developed moderate to severe TED shortly after she received the second dose of ChAdOzx1-S vaccine (Oxford/Astra Zeneca). She had systemic IV steroid and noticed an improvement in her condition (Three doses of 1g IV followed by a tapering dose of oral steroid for two months). However her condition worsened again after receiving the third dose of vaccine one month later and following the tapering of oral steroids. This included bilateral blurry vision (more pronounced in the right eye), severe bilateral conjunctival and caruncular injection and edema, bilateral upper and lower lid edema, bilateral proptosis, double vision, and pain behind the eyes (Figure 4).
On presentation to our facility, ocular examination showed best corrected visual acuity of hand movement (HM) for the right eye and 6/10 for the left eye. Intraocular pressure was 32 mmHg OD and 24 mmHg OS. External examination showed bilateral lower eyelid retraction and severe bilateral upper and lower lid redness and swelling. The patient had bilateral conjunctival and caruncular injection with superficial inferior punctate keratitis. Posterior segment examination was unremarkable. There was a right relative afferent pupillary defect. Exophthalmometry was 26mm bilaterally. A visual field test was done but revealed unreliable results because of her poor vision. Her eyes were straight in primary position, however orthoptic examination showed restriction of (-4) in supraduction and (-2) in all other directions. Color vision was not recordable, due to bilateral color blindness. As the patient was a self-pay, she did not agree to the VEP test. CT imaging was brought by the patient in the form of printed films from her home country and it was not possible to measure the Barrett’s index.
Laboratory results showed high IL-6 (30.6 pg/mL; N< 7.0), High TSH (5.120 milli IU/L; N>0.270< 4.200), and high TSI (16.40 IU/L; N< 1.75 IU/L).
She was started on four doses of intravenous Tocilizumab (8 mg/kg), each infusion one month apart. Her vision improved to 6/9 in the right eye and 6/6 in the left eye. Her Exophthalmometry reading improved to 23 mm OD and 22 mm OS.
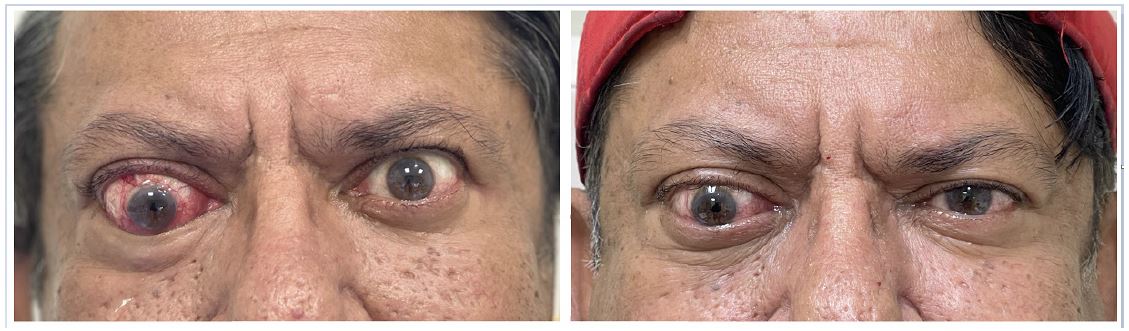
Figure 1: (case 1) Left: patient on presentation showing right eye hypotropia, apparent proptosis, severe conjunctival and caruncular injection and lower eyelid entropion. Right: patient after 6 injections of Tocilizumab.

Figure 2: (case 1) Humphrey 24-2 visual fields on presentation: right eye inferior patchy visual field defect not respecting the vertical line.

Figure 3: (case 1) CT scan A: coronal section, showing vertical Barret’s index of 64% which is highly sensitive and specific for DON. B: CT scan, axial section, showing stretched right optic nerve (blue arrow) with slight enlargement of muscles bellies sparing the tendons. C: coronal section, the mainly enlarged muscle is the right inferior rectus (red arrow) causing crowding of orbital apex.

Figure 4: (case 2) Left: Patient on presentation showing right eye hypertropia, bilateral upper and lower eyelid edema and bilateral conjunctival and carbuncular injection. Right: patient after 4 injections of Tocilizumab.
Discussion
Coronavirus disease 2019 (COVID-19) is a highly contagious infectious disease that causes severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [18].
The World Health Organization defines post-vaccine adverse events as any untoward medical occurrence that follows the immunization, which does not necessarily have a causal relationship with the use of the vaccine [19].
Lately, an increasing number of autoimmune phenomena following the infection itself or after COVID–19 vaccinations have been reported, mostly vaccine-induced thrombotic thrombocytopenia [10,20]. Other autoimmune diseases include autoimmune liver diseases, immune thrombocytopenic purpura, Guillain–Barré syndrome, IgA nephropathy, inflammatory arthritis, SLE, lupus nephritis, and Graves' disease [10,20].
The potential mechanisms of immune activation comprise molecular mimicry mechanism, production of particular autoantibodies, and the role of vaccine adjuvants [10]. Molecular mimicry is caused by the similarity between some vaccine components and certain human proteins, and this could trigger the immune system to attack similar proteins in the body of susceptible individuals and cause autoimmune diseases [10].
Adjuvants play an essential role in the immunogenicity of active ingredients of the vaccines. However, one unwanted consequence of this response is the triggering of autoimmune diseases including thyroid disease [21].
Subacute thyroiditis is the most commonly reported SARS-CoV-2 vaccination-related thyroid disease, followed by Graves' disease [22]. In Graves’ disease, enhanced levels of Interleukin 6 (IL-6 ) have been detected [23]. Likewise, the SARS-CoV-2-associated hyper-inflammatory cascade has similarly been found to be regulated by type 1 T helper cells (Th1) and IL-6 [24].
There have been numerous studies showing the role of IL-6 in the pathogenesis of active thyroid eye disease and the effectiveness of tocilizumab, a recombinant humanized anti-IL-6 receptor antibody [25].
Our hospital is a tertiary center within the country. The prevalence of TED in Graves’ disease is approximately 40%. However, the incidence of covid vaccine induced DON is extremely rare.
Both of our cases presented with sudden onset and rapidly progressive DON following different types of COVID-19 vaccination. Both had elevated levels of TSI and IL-6.
Elevated levels of TSI and IL 6 have been well documented in severe active thyroid eye disease [26].
One of our cases is a male patient, and it is well-known that males are genetically less susceptible to developing autoimmune syndromes [27]. The patient was a heavy smoker and smoking is a well-recognized factor to increase the inflammatory responses and trigger the immune system and cause autoimmune syndromes including Graves’ disease [27]. However, no strong risk factor or predictor has been identified to influence Graves' disease occurrence after SARS-CoV-2 vaccination.
Development of TED has been reported following COVID-19 infection or vaccination [28].
Thyroid stimulating immunoglobulin (TSI) is a well-known autoantibody in the development of thyroid eye disease. On presentation one of our patients (female) had previous history of hyperthyroidism and thyroidectomy. The hyperthyroid status of this patients has been stable for many years before the vaccination. The male patient did not have any previous history of thyroid dysfunction and at presentation his thyroid function tests were normal – The only autoimmune indicator was elevated TSI and IL-6 levels. In this patient, DON occurred de novo following vaccination with Covid -19. However, this patient subsequently developed a hypothyroid status with a recurrence of DON.
Recently, there have been reports of the presence of various organ-specific and systemic autoantibodies in the serum of patients with autoimmune syndromes following COVID-19 vaccine. Both cases have thyroid-specific autoantibodies and elevated IL-6 levels [29-31].
Systemic corticosteroid treatment has been the first line of treatment in DON [17]. Both of our patients had received high doses of intravenous steroids, followed by long-term oral steroids. None of the patients improved with systemic steroids. Bartalena et al have shown that systemic steroid treatment is not effective in up to 20-30% of cases who suffer severe thyroid eye disease [32]. However, there is no evidence from any randomized controlled trials currently to evaluate the side effects of tocilizumab for the treatment of patients with TED [33].
Following administration of intravenous tocilizumab, a positive response was observed within the first 4 weeks of the treatment. By the end of the treatment course (4-6 doses of tocilizumab) both patients experienced an improvement in visual functions and signs and symptoms of DON were alleviated.
Similar positive responses have been reported to tocilizumab in severe thyroid eye disease by multiple authors [15,16,34,35].
Conclusions
Among other complications of Covid-19 infection or its vaccination, the development of severe thyroid eye disease with optic nerve compression should be considered and vaccination should be offered with care. Nevertheless, patients should not be discouraged from obtaining appropriate and timely vaccination against the virus.
Responsiveness of these two cases to tocilizumab has shown that it can be a promising treatment option for DON including those cases that are not responsive to systemic steroids.
We have encountered two cases only, more long-term results and observations are needed to further explore this relationship while looking into the optimum treatment protocols for Covid-19 related thyroid eye disease, the severity of resultant TED, and treatment options.
References
- Weiler DL. Thyroid eye disease: A review. Clin Exp Optom. 2017; 100: 20-25.
- Salleh NA, Seng WH, Isa HD. Optic Neuropathy in Thyroid Eye Disease: A Case Series. Korean J Fam Med. 2016; 37: 197-201.
- Dosiou C, Kossler AL. Thyroid Eye Disease: Navigating the New Treatment Landscape. J Endocr Soc. 2021; 5: bvab034.
- Boelaert K, Newby PR, Simmonds MJ, Holder RL, Carr-Smith JD, Heward JM, et al. Prevalence and relative risk of other autoimmune diseases in subjects with autoimmune thyroid disease. Am J Med. 2010; 123: 183.e1-9.
- Dolman PJ. Evaluating Graves’ orbitopathy. Best Pract Res Clin Endocrinol Metab. 2012; 26: 229-248.
- Parums DV. Editorial: First Full Regulatory Approval of a COVID-19 Vaccine, the BNT162b2 Pfizer-BioNTech Vaccine, and the Real-World Implications for Public Health Policy. Med Sci Monit. 2021; 27: e934625.
- Kashte S, Gulbake A, El-Amin Iii SF, Gupta A. COVID-19 vaccines: rapid development, implications, challenges and future prospects. Hum Cell. 2021; 34: 711-733.
- Skowronski DM, De Serres G. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med. 2021; 384: 1576-1577.
- Dagan N, Barda N, Kepten E, Miron O, Perchik S, et al. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N Engl J Med. 2021; 384: 1412-1423.
- Chen Y, Xu Z, Wang P, Li XM, Shuai ZW, Ye DQ, et al. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology. 2022; 165: 386-401.
- Oster ME, Shay DK, Su JR, Gee J, Creech CB, Broder KR, et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA. 2022; 327: 331-340.
- Tabatabaee S, Rezania F, Alwedaie SMJ, Malekdar E, Badi Z, et al. Post COVID-19 vaccination Guillain-Barre syndrome: three cases. Hum Vaccin Immunother. 2022; 18: 2045153..
- Molina-Rios S, Rojas-Martinez R, Estévez-Ramirez GM, Medina YF. Systemic lupus erythematosus and antiphospholipid syndrome after COVID-19 vaccination. A case report. Mod Rheumatol Case Rep. 2023; 7: 43-46..
- Almazrouei O, Alalawi F, Albrashdi S, Alsharqi H, Alsaadi A, et al. A 46-Year-Old Woman with a 4-Year History of Graves Disease, with Severe Corticosteroid-Unresponsive Thyroid Eye Disease, Successfully Treated with Tocilizumab. Am J Case Rep. 2023; 24: e938487.
- Albrashdi S, Alsharqi H, Habroosh F, Eatamadi H. Tocilizumab use in pediatric thyroid eye disease: First documented case. Am J Ophthalmol Case Rep. 2022; 25: 101387.
- Perez-Moreiras JV, Gomez-Reino JJ, Maneiro JR, Perez-Pampin E, Romo Lopez A, et al. Tocilizumab in Graves Orbitopathy Study Group. Efficacy of Tocilizumab in Patients With Moderate-to-Severe Corticosteroid-Resistant Graves Orbitopathy: A Randomized Clinical Trial. Am J Ophthalmol. 2018; 195: 181-190.
- Bartalena L, Baldeschi L, Boboridis K, Eckstein A, Kahaly GJ, Marcocci C, et al. The 2016 European Thyroid Association/European Group on Graves’ Orbitopathy Guidelines for the Management of Graves’ Orbitopathy. Eur Thyroid J. 2016; 5: 9-26.
- Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). Treasure Island (FL): StatPearls Publishing; 2022.
- Mansoor O. Immunization Safety Surveillance: Guidelines for Immunization Programme Managers on Surveillance of Adverse Events Following Immunization. 3rd ed. Geneva, Switzerland: World Health Organization, Western Pacific Region; 2016.
- Gracia-Ramos AE, Martin-Nares E, Hernández-Molina G. New Onset of Autoimmune Diseases Following COVID-19 Diagnosis. Cells. 2021; 10: 3592.
- Pujol A, Gómez LA, Gallegos C, Nicolau J, Sanchís P, González-Freire M, et al. Thyroid as a target of adjuvant autoimmunity/inflammatory syndrome due to mRNA-based SARS-CoV2 vaccination: from Graves’ disease to silent thyroiditis. J Endocrinol Invest. 2022; 45: 875-882.
- Jafarzadeh A, Nemati M, Jafarzadeh S, Nozari P, Mortazavi SMJ. Thyroid dysfunction following vaccination with COVID-19 vaccines: a basic review of the preliminary evidence. J Endocrinol Invest. 2022; 45: 1835-1863.
- Salvi M, Girasole G, Pedrazzoni M, Passeri M, Giuliani N, Minelli R, et al. Increased serum concentrations of interleukin-6 (IL-6) and soluble IL-6 receptor in patients with Graves’ disease. J Clin Endocrinol Metab. 1996; 81: 2976-2979.
- Costela-Ruiz VJ, Illescas-Montes R, Puerta-Puerta JM, Ruiz C, Melguizo-Rodríguez L. SARS-CoV-2 infection: The role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020; 54: 62-75.
- Moi L, Hamedani M, Ribi C. Long-term outcomes in corticosteroid-refractory Graves’ orbitopathy treated with tocilizumab. Clin Endocrinol (Oxf). 2022; 97: 363-370.
- Kumar S, Schiefer R, Coenen MJ, Bahn RS. A stimulatory thyrotropin receptor antibody (M22) and thyrotropin increase interleukin-6 expression and secretion in Graves’ orbital preadipocyte fibroblasts. Thyroid. 2010; 20: 59-65.
- Antonelli A, Ferrari SM, Ragusa F, Elia G, Paparo SR, et al. Graves’ disease: Epidemiology, genetic and environmental risk factors and viruses. Best Pract Res Clin Endocrinol Metab. 2020; 34: 101387.
- Park KS, Fung SE, Ting M, Ozzello DJ, Yoon JS, Liu CY, et al. Thyroid eye disease reactivation associated with COVID-19 vaccination. Taiwan J Ophthalmol. 2022; 12: 93-96.
- Watad A, De Marco G, Mahajna H, Druyan A, Eltity M, Hijazi N, et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination. Vaccines (Basel). 2021; 9: 435.
- Vera-Lastra O, Ordinola Navarro A, Cruz Domiguez MP, Medina G, Sánchez Valadez TI, et al. Two Cases of Graves’ Disease Following SARS-CoV-2 Vaccination: An Autoimmune/Inflammatory Syndrome Induced by Adjuvants. Thyroid. 2021; 31: 1436-1439.
- Gupta RK, Ellis BK. Concurrent Antiglomerular Basement Membrane Nephritis and Antineutrophil Cytoplasmic Autoantibody-Mediated Glomerulonephritis After Second Dose of SARS-CoV-2 mRNA Vaccination. Kidney Int Rep. 2022; 7: 127-128.
- Bartalena L, Krassas GE, Wiersinga W, Marcocci C, Salvi M, Daumerie C et al. European Group on Graves’ Orbitopathy. Efficacy and safety of three different cumulative doses of intravenous methylprednisolone for moderate to severe and active Graves’ orbitopathy. J Clin Endocrinol Metab. 2012; 97: 4454-4463.
- Hamed Azzam S, Kang S, Salvi M, Ezra DG. Tocilizumab for thyroid eye disease. Cochrane Database Syst Rev. 2018; 11: CD012984.
- Sy A, Eliasieh K, Silkiss RZ. Clinical Response to Tocilizumab in Severe Thyroid Eye Disease. Ophthalmic Plast Reconstr Surg. 2017; 33: e55-e57.
- Pérez-Moreiras JV, Varela-Agra M, Prada-Sánchez MC, Prada-Ramallal G. Steroid-Resistant Graves’ Orbitopathy Treated with Tocilizumab in Real-World Clinical Practice: A 9-Year Single-Center Experience. J Clin Med. 2021; 10: 706.
