
Open Access, Volume 9
An open lower extremity degloving injury
Keith Henry1*; Rachel Nordby2; Kristi gradually2; Bradly Hernandez2
1Director of Medical Student Education, Department of Emergency Medicine, University of Minnesota Medical School, Minneapolis Minnesota, USA.
2Resident Physician, HealthPartners Institute for Medical Education, Emergency medicine Residency, St Paul, MN, USA.
Keith Henry
Director of Medical Student Education, Department of Emergency Medicine, University of Minnesota Medical School, Minneapolis Minnesota, USA.
Email: kdhenrymd@comcast.net
Received : April 11, 2023,
Accepted : May 25, 2023
Published : May 31, 2023,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Henry K (2023).
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Henry K, Nordby R, Grall K, Hernandez B. An open lower extremity degloving injury. Open J Clin Med Case Rep. 2023; 2046.
Case Summary
A 25 year old male presents by EMS to the Emergency Department following a work related crush injury to his right thigh. The patient preforming manual labor at a nearby factory warehouse. His right thigh was accidentally pinned between the rear end of a forklift and a large stationary structural support pole. He was trapped for approximately 30 seconds as his co-workers forcefully pulled him out and away from the injury site. He complained of severe right thigh pain, limited range of motion of the right leg secondary to pain, and inability to bear weight. EMS was dispatched to the scene and the patient was transported to the Emergency Department for evaluation. Vital signs were stable at the time of arrival. Upon completion of a full physical exam, discoloration, tenderness, and soft tissue swelling was noted to the right thigh (Figure 1). The right lower extremity was otherwise neurovascularly intact and no alternate injury was identified.
Plain film imaging of the right thigh was obtained to evaluate for any evidence of fracture or bony injury. The image (Figure 2) was notable for a radiolucent linear finding that was compatible with soft tissue gas; highly suggestive of an open soft tissue injury.
Follow up CT imaging (Figure 3) confirmed extensive air and fluid throughout the subcutaneous soft tissues of the right thigh consistent with a high energy crush mechanism.
Patient care was expedited to the operating room the following day for incision and drainage. A wound vacuum dressing was placed and the patient endured a lengthy recovery with several additional visits to the operating room for irrigation, debridement, and closure.

Figure 1: A photo of the patients right thigh upon his initial presentation. To the Emergency Department (printed with permission).

Figure 2: A plain film image of the right thigh. Red arrow denotes a linear area of radio-lucency indicating a traumatic separation of epidermis from deeper subcutaneous tissues.
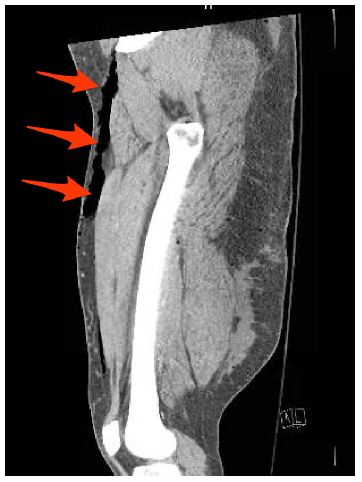
Figure 3: Coronal CT image of the right thigh. Red arrows confirm the Morel-Lavalee lesion noted on plain film imaging.
Discussion
A degloving injury is when a sudden and forceful shearing force separates the superficial tissue-skin or subcutaneous tissue- from the deeper layers-fascia or muscle. Most commonly seen in motor vehicle trauma, degloving injuries can also occur secondary to crush injury or other mechanistically high energy trauma [1]. When the space between the two layers is exposed to the environment the degloving injury is classified as open, while often these injuries are closed and therefore designated as a Morel Lavelle lesions [2]. Where the superficial tissue separates from the deeper tissue, a potential space is created which fills with blood and possibly gas and can quickly expand as the cellular membranes become more permeable and the tissues swell. The overlying skin is no longer connected to blood supply and quickly becomes ischemic [3]. Depending on the size of the injury, adjacent fractures, and the anatomy of the specific location of the injury, as the potential space expands the outward pressure on the skin increases. As the pressure builds, the already tenuous tissue can quickly go from possibly viable to necrotic. These lesions are commonly complicated by bacterial infection, compartment syndrome, and delayed wound healing. If the superficial layer has been completely removed, there is little to no risk for this to occur.
Internal degloving injuries are often underestimated as the lesion is not visible to the eye and frequently occurs as a part of a polytrauma in the setting of other distracting injuries. Such as seen in our patient, the skin appears swollen and bruised, but gives little indication as to the time sensitive expanding injury below. Fluctuance, crepitus, ecchymosis and decreased sensation on initial exam should raise the providers suspicion for an internal degloving injury however the lack of these on exam does not rule it out [4]. Special attention to a rapidly changing exam should also clue one in to the possibility of a worsening internal degloving injury [5].
These lesions can vary in size and depth and there is no standardized classification system to assist in delineating the severity of the injury. The lesion will appear similar to a necrotizing soft tissue infection on diagnostic imaging. X-rays can reveal gas and fluid collection along the fascial plane and ultrasound can be used to identify this potential space. CT scans will likely demonstrate both, however, just like an NSTI, the lack of these findings does not rule this diagnosis out. The gold standard of imaging is relegated to the MRI; this would often be obtained later in the disease course.
References
- Scolaro, John A. MD, MA; Chao, Tom MD; Zamorano, David P. MD. The Morel-Lavallée Lesion: Diagnosis and Management. Journal of the American Academy of Orthopaedic Surgeons. 2016; 24: 667-672, October 2016.
- Hakim S, Ahmed K, El-Menyar, A. et al. Patterns and management of degloving injuries: a single national level 1 trauma center experience. World J Emerg Surg 11, 35 (2016).
- Lin HL, Lee WC, Kuo LC, Chen CW. Closed internal degloving injury with conservative treatment. Am J Emerg Med. 2008; 26: 254.e5-6.
- Muneer M, El-Menyar A, Abdelrahman H, Murad MA, Al Harami SM, Mokhtar A, Khawar M, Awad A, Asim M, Latifi R, Al-Thani H. Clinical Presentation and Management of Pelvic Morel-Lavallee Injury in Obese Patients. J Emerg Trauma Shock. 2019; 12: 40-47.
