
Open Access, Volume 9
General trends in the prevention and treatment of cerebrovascular disease in the XXI century
Valentin Reutov1*; Elena Sorokina2
1Institute of Higher Nervous Activity and Neurophysiology Russian Academy of Sciences, Moscow 117485 Butlerova Str. 5a.
2National Medical Research Center for Children’s Health, Ministry of Health of the Russian Federation, 119991, Moscow, Lomonosovsky Prospekt, 2.
Valentin Palladievich Reutov
Institute of Higher Nervous Activity and Neurophysiology Russian Academy of Sciences, Moscow 117485 Butlerova Str. 5a
Email: valentinreutov@mail.ru
Received : March 21, 2023,
Accepted : May 19, 2023
Published : May 23, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Cerebrovascular disease has reached epidemic proportions worldwide. They are the leading cause of death in developed countries. These diseases account for more than a quarter of reported deaths worldwide. The main causes of cerebrovascular disease are: hypertension, diabetes mellitus, dyslipidemia and Atrial Fibrillation (AF). Behavioral risk factors are added to them: traumatic brain injuries in everyday life and sports, smoking and alcohol abuse. The population of different countries of the world is in need of knowledge about the main signs of stroke. This knowledge will contribute to the fact that transient ischemic attacks and pre-stroke conditions can be considered as a neurological emergency. There is reason to believe that research advances in the 21st century will provide new and more effective strategies for the treatment of acute stroke. However, a global lifestyle change is needed to prevent strokes, improve health and increase life expectancy.
Keywords: Reactive forms of nitrogen and oxygen; Hemorrhagic stroke; Ischemic stroke; Nitrosative and oxidative stress; Regulatory cycles of nitric oxide and superoxide anion radical; Dysregulatory pathology.
Copy right statement: Content published in the journal follows Creative Commons Attribution License. (http://creativecommons.org/licenses/by/4.0). © Reutov VP (2023).
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Reutov VP, Sorokina E. General trends in the prevention and treatment of cerebrovascular disease in the XXI century. Open J Clin Med Case Rep. 2023; 2043.
Introduction
A stroke is a violation or a sharp failure in the circulatory system of the brain, leading to the defeat of its various departments. Together with the violation of blood flow and the cessation of oxygen supply to certain parts of the brain, energy mechanisms are violated in them. In this case, nerve cells lose their energy-dependent functional abilities, which primarily provide energy-intensive ion homeostasis [1,2]. Hypoxia/ischemia, inflammation, and the development of immune/autoimmune reactions are universal and key elements of the ischemic cascade in cerebral ischemia and strokes [3-5]. An analysis of literature data (1948–2010) showed that hypothermia, artificial coma, drug-induced sleep, or transfer of the body to a state of “sedation”, characterized by a complete absence or decrease in the level of consciousness (from Latin sedatio - “sedation”) leads to a decrease in damage and death of nerve cells. Further search for ways to protect the brain and prolong life during stroke, which is one of the most expensive diseases, is an urgent biomedical problem. Violation of cerebral circulation and strokes significantly reduce the average life expectancy, and, like no other disease, worsen its quality. In connection with the change in the age structure of the population, there is reason to believe that with the aging of people - the inhabitants of our planet - the number of cases of strokes in the world will increase if the lifestyle is not modified in a timely manner and the population is not trained to identify signs of cerebrovascular accident and strokes [6-8].
Problems of education, prevention and treatment at the level of the whole organism
Notable advances in the diagnosis and treatment of ischemic stroke have been made over the past two decades. During the 20th century (especially from 1990 to 2000), the total number of deaths from strokes declined in populations where preliminary work was done to educate people about the signs of acute cerebrovascular accident (ACI). However, the proportion of deaths that occur before a patient is hospitalized has increased to nearly 50% of all stroke deaths [6–9]. One of the national health goals in the United States for 2010-2025 was to increase the number of people who are able to recognize the signs of a stroke at the first symptoms [6]. The Centers for Disease Control and Prevention (CDCP) was established to assess public awareness and knowledge of an appropriate response to emergencies and analyzed data from the Behavioral Risk Surveillance System in 17 states and the US Virgin Islands. (USVI) [6]. An analysis of these results showed that the awareness of the white population in the United States about some signs of cerebrovascular accident that precedes a stroke is quite high. These signs include severe and persistent headache, drowsiness and apathy, severe weakness. Acute cerebrovascular accident can occur in the form of a transient ischemic attack, microstroke or stroke. It is considered that a stroke occurs if neurological symptoms persist for more than a day. In the presence of a transient disorder of cerebral circulation, as with a microstroke, signs of impaired body functions disappear on their own within 24 hours. After them, morphological changes in the brain cells are absent. As a result of a microstroke, foci of necrosis of the substance of the brain are formed. With a stroke, there are: a) impaired speech (slurred, too slow, meaningless); b) nausea and vomiting; c) severe headache (occurs suddenly); d) violation of coordination; e) vision problems (double vision, blindness in one or both eyes); e) weakness in the limbs; g) violation of the sensitivity of one half of the body. Possible: h) loss of consciousness; i) increased sensitivity up to the complete rejection of bright light and loud sounds; j) paresis of limbs on one side of the body and impaired coordination of movements; k) the appearance of facial asymmetry. If these symptoms persist for 24 hours or worsen, it is a stroke. Sometimes the symptoms of a microstroke can be confused with a reaction to stress or chronic fatigue. However, the ability to recognize the main signs of stroke is low on average among the general US population. In this regard, educational campaigns are needed to raise public awareness about the signs of a stroke and the need to call 911 in case of cerebrovascular accident and the possible occurrence of a stroke [7-9]. The number of 24-hour ambulance service in China is 120 people.
If necessary, you can also call the emergency number 110 or the police station - the operator will transfer you to the right line. In order to increase public awareness and knowledge about recognizing the signs of a stroke in China (Shanghai), a special program “Stroke 1-2-0” was developed - an adapted recognition tool “Face, Hand, Speech” for prompt response to the onset of a stroke [8-14]. To do this, two communities with a population of at least 100,000 people were selected in the same area of Shanghai. They have been included in the “Public Education Program Evaluation System” to reduce the incidence of strokes in adults compared to conventional treatments. The studies were carried out for 1 year. The primary outcomes were the time from symptom onset to hospital arrival (“start-to-door time”, ODT) and the frequency of arrival at the hospital within 3 hours. The conventional intention-to-treat approach was used as a control. Studies have shown that such an educational program led to an increase in the number/proportion of patients admitted to the hospital within the first 3 hours after the onset of a stroke [10-12]. The Disease, Injury, and Risk Factors (GBD) study aimed to provide a standardized and comprehensive assessment of efficacy at global, regional, and national levels [15, 16]. These large-scale studies showed that high body mass index remained the fastest growing risk factor for stroke between 1990 and 2019. Thus, the older a person becomes, the more difficult it is for him to maintain body weight. A decrease in the intensity of metabolism in humans begins after 20-25 years. On average, metabolism slows down by 0.5-1% per year. This process is especially active after 40 years. By the age of 45, calories are burned 10-20% slower than 20 years ago. Moreover, every decade the rate of metabolic decline increases. In this case, the replacement of muscle tissue with fat mass occurs. There is reason to believe that this factor will only increase in low-income countries with irregular meals. Therefore, if special effective strategies for metabolic correction and primary prevention of stroke are not implemented, then a high body mass index may remain one of the fastest growing risk factors as the population ages [16-18]. In high-income countries, age-standardized mortality from stroke was 3–4 times lower than in low-income countries (data from the World Bank) [16-18]. According to statistics, stroke is more common in men over 55 years of age and in women over 65 years of age. However, according to the CDCP, 25% of stroke survivors are under 45 years of age. According to the world’s leading neurologists, there are no people with a zero risk of stroke. Violations of cerebral circulation most often occur against the background of arterial hypertension, atherosclerosis and diabetes mellitus. The latter - diabetes mellitus - serves as a catalyst for the first two diseases. Other risk factors: age (after age 50, the risk approximately doubles with every decade lived), increased blood viscosity, overweight, lack of physical activity, atrial fibrillation, smoking, alcohol abuse. A person can influence only some of the above risk factors. According to the World Health Organization (WHO), 15 million people worldwide suffer a stroke each year. Of these, more than 6 million die and another 5 million remain disabled. How to deal with this phenomenon?
Stroke prevention
In light of recent evidence that 85% of all strokes are preventable, stroke prevention strategies are coming to the fore in stroke management. The risk of stroke can be substantially reduced with medical interventions that have been proven in many studies, combined with effective lifestyle changes. At the same time, almost all scientists and doctors note that global lifestyle modification is more beneficial for health than the treatment of individual risk factors [1,3,15–20]. The objective of this review was to summarize and analyze the experimental and clinical literature data, as well as the results of our own studies on experimental models, which made it possible to speak about the existence of typical disorders of neurons and glial cells against the background of pathological changes in cerebral circulation. These changes, disturbances and damage occur in the first minutes of stroke development, and, ultimately, affect long-term functional outcomes. Due to the inhibitory effect on the final stages of the ischemic cascade (oxidative and nitrosative stress) and the development of reactions associated with inhibition of metabolism, hypothermia, artificial coma or drug-induced sleep, as well as intravenous thrombolysis were introduced as neuroprotective strategies [4-10]. An analysis of the available clinical data has shown that intravenous thrombolysis can minimize disability if patients present to the emergency department for treatment within 3-4.5 hours of the onset of stroke and circulatory disorders. This is also evidenced by the facts that the inhabitants of the United States, who have full or partial descent from Africans, and Latin Americans are Hispanic and Portuguese-speaking peoples, widely represented in the United States, Spain, Canada, Portugal, Italy, Great Britain and other countries due to economic and political emigration, more likely to die and become disabled from a stroke than Americans of English and European descent. This is partly due to late hospitalization and the inability to perform intravenous thrombolysis in acute stroke. Poor knowledge of stroke symptoms and when to call 911 may contribute to a significant difference in acute stroke outcomes among these US populations [7-16]. Particular attention in the review is paid to local damage to cell membranes and subcellular structures in the cerebellum under glutamate (Glu) exposure against the background of oxidative and nitrosative stress. The analysis of these studies made it possible to show that any cellular system in living organisms, although it functions according to its own laws, in pathological conditions exhibits common non-specific features of damage associated with a violation of regulatory mechanisms that can be influenced, and thereby reduce the negative consequences of strokes.
Global lifestyle modification
It has long been noted that physical activity provides the energy function of the mitochondria of body tissue cells. Constant intellectual work is a factor that ensures an increase in average life expectancy, efficient brain function with a healthy lifestyle. Hippocrates (about 460 BC - about 370 BC) - an ancient Greek healer, doctor and philosopher lived for 90 years. I. Kant (1724-1804), who did not have good health from birth, lived to almost 80 years. In every country in the world, you can find that successful people in the creative professions reach the age of 90 more often than the rest of the population. In the last 30 years, the average life expectancy of such people has reached the life expectancy of known centenarians living in the mountains under conditions of moderate hypoxia. The constant physical activity of the highlanders is associated with a difference in height in the highlands, which the inhabitants of these regions must regularly overcome. Classical music (especially regular playing of a musical instrument), the study of new foreign languages, the preparation of lecture courses, as well as the recitation of highly artistic works of prose and poetry can make an additional contribution to protecting the brain from degenerative age-related changes in people living in urban areas [16-19]. It has been established that listening to vocal music is an effective and easily applicable tool for supporting cognitive recovery after a stroke. The rehabilitative effects of vocal music are due to both structural and functional changes in plasticity in the temporo-parietal lobes/networks, which are critical for processing emotions, language, and memory [19–29]. Why did moderate hypoxia, physical activity and constant intellectual work become the factors that protect the brain? What is the main factor of influence, including the compensatory-adaptive and adaptive mechanisms of the body,which, under the same conditions, increase the average life expectancy by 25-30%? The answers to these questions are very promising for developing strategies to prevent brain damage. They can also be used in the treatment of cognitive impairment.
General trends in the prevention and treatment of strokes in the world
In the last 20th century (especially at the end of it), preclinical studies were still practically unable to predict the course of stroke and poorly predicted possible clinical therapy. However, over the past 30 years, conferences have been held almost annually in Europe and the USA [30–50]. The research materials presented at these conferences have made a huge contribution to the understanding of post-stroke pathology. The first International Stroke Conference was held in Switzerland (Geneva, May 30 - June 1, 1991) [30]. Modern clinical trials (www.strokecenter.org/trials), as mentioned above, provide for a wide range of approaches: from hypothermia to cell therapy and neuroprotection [31–51]. However, the treatment of strokes and hemorrhages still leaves much to be desired. There are differences in the risk of stroke, the frequency of stroke and in its treatment. Currently, scientists and physicians have come to the conclusion that stroke is a heterogeneous disease with multiple additive risk factors and causes. Primary prevention of stroke, aimed at modifying risk factors, plays an important role in reducing the severity of stroke in the aging population. Secondary prevention of recurrent strokes depends on evaluation and individualized treatment aimed at the mechanisms responsible for the occurrence of stroke or transient ischemic attack [32-57]. As stated above, stroke is the second leading cause of death and the leading cause of disability in the adult population worldwide. Already at present, acute cerebrovascular accident (ACV) and strokes/infarctions of the brain are recorded up to 3 times more often than myocardial infarctions. Over the past decades (1990–2020), the absolute number of stroke cases has increased by 70%, patients after stroke have increased by 85%, stroke mortality has increased by 43%, and DALY (Disability Adjusted Life Years) is an integral medical and economic indicator that characterizes consequences of a stroke increased by 32% [1–10]. In Russia, the number of cases of stroke in recent decades has amounted to 340 people. per 100 thousand population per year [21–29]. This means that approximately every 1.5 minutes a Russian develops this disease, and the mortality rate from it remains one of the highest in the world. More than 1 million stroke survivors live in the Russian Federation (RF). After a stroke in the Russian Federation, almost every second patient dies by the end of the first year, and after 7 years, almost 80% of patients die [21–29].
Epidemiology and prevention of ischemic stroke
As part of the European Stroke Symposium in 2005, the Stroke Research Priorities for the Next Decade - A Representative Opinion of the European Scientific Community were published, recommending research into various treatments that have a neuroprotective effect [27-57]. Heart Disease and Stroke Statistics conferences were held annually in the USA. Update: A Report From the American Heart Association [27]. In 2010, the Consensus Conference in Brussels adopted the document “Hypothermia in Stroke: A Call to Action 2010” [28], which established a research program on the use of hypothermia in patients with acute ischemic stroke, which was updated in 2015–2016 [31,34,41-43]. In January 2018, the American Heart Association (AHA) and the American Stroke Association (ASA) updated guidelines for the early management of patients with acute ischemic stroke, which were presented at the International Stroke Conference 2018 on January 24–26 in Los Angeles [45]. The AHA/ASA recommendations were based on an analysis of data from more than 400 peer-reviewed articles published in highly rated journals. The main works have been reviewed by a panel of stroke management experts and are currently the most comprehensive recommendations for the treatment of ischemic stroke published since 2013 [45]. An unchanging, but extremely important recommendation remains the need for quick pre-hospital action when the first symptoms of a stroke appear. In April 2022, the American Academy of Neurology Guidelines for the Treatment of Symptomatic Intracranial Atherosclerotic Stenosis were published [56].
Basic recommendations
Clinicians should recommend: a) aspirin up to 300–350 mg for long-term prevention of stroke and death, and b) in patients with severe (70%–99%) symptomatic stenosis, if the risk of hemorrhagic transformation is low, co-administration should also be recommended. the appointment of clopidogrel 75 mg with aspirin for 90 days; c) high-intensity statin therapy should be recommended to achieve LDL-C < 70 mg/dl; d) to achieve the target blood pressure < 140/90 mmHg. prescribed antihypertensive therapy; and, e) at least a moderate level of physical activity. What recommendations are contraindicated? Should not be recommended: a) routine angioplasty as monotherapy or b) indirect shunting for stroke prevention in patients with symptomatic stenosis outside of clinical trials; c) direct shunting for stroke prevention in patients with symptomatic atherosclerotic stenosis. [58]. Over the past decades, changes have been made in the primary prevention of stroke. There is information about the lack of a preventive effect from taking vitamins, antioxidants, and hormone replacement therapy in women (the same information applies to secondary prevention). Changes were also made about the possibilities of antiplatelet therapy in the primary prevention of stroke. New recommendations have been made for the treatment of sleep disorders such as sleep apnea using continuous positive airway pressure equipment.
Standards of medical care in the USA and Europe for acute cerebrovascular accident (ACV)
At the earliest (before the hospital stage), the standards for providing medical care for strokes are reduced to stabilizing the condition and reducing the time of transporting the patient to the hospital. Currently, there are special stroke recognition scales. At the hospital stage, such patients are shown basic and specific therapy. In the case of ischemic stroke, “basic stroke therapy” is a therapy primarily aimed at restoring blood flow to the brain and increasing the functional activity of neurons in the area around the infarction – penumbra. These activities include: a) maintaining respiratory and circulatory functions; b) correction of metabolic and volemic disorders; c) control of blood pressure; d) prevention and treatment of conditions such as epileptic seizures; e) venous thrombosis, dysphagia, aspiration pneumonia and other infectious complications; f) correction of increased intracranial pressure. The purpose of these measures is to normalize the rheological properties of blood, improve perfusion of brain tissue under normal temperature conditions, and improve blood circulation when the problem area is cooled (hypothermia with a target temperature of 33°C) [53-58].
Damage to the brain in ischemia/hypoxia, stroke, or injury involves the formation of an infarction core, where alterations are irreversible and blood supply is extremely low. The penumbra, or ischemic half-shadow, is an area that surrounds the damage focus, is characterized by metabolic alterations and lower blood supply, lacks spontaneous or evoked electrical potential, but preserves ion homeostasis. Thus, the updated version of the guidelines expanded the indications for the administration of alteplase (t-PA), a thrombolytic drug used to treat acute ischemic stroke during the first 4.5 hours after the onset of a stroke. Alteplase acts in a manner similar to the normal human plasminogen activator produced in vascular endothelial cells and used to dissolve a clot. The drug may also be used in some patients with mild stroke. However, physicians are advised to weigh the risks and benefits before initiating therapy in this group of patients [53,55–58].
In the Specific Therapy section, emphasis was placed on thrombolytic, antiplatelet, and early anticoagulant therapy. In the neuroprotective program, according to the text of the 2008 recommendations, which demonstrated a significant improvement in the outcome of the disease, no further effective action was found [59]. The results of a randomized control trial (RCT), which aims to reduce sources of bias by randomly assigning subjects, including a placebo control group, showed that free radical scavengers, antioxidants, and magnesium sulfate were not effective.
In accordance with the recommendations of the European Stroke Organization, the American Heart Association and the American Stroke Association, as well as the Russian National Clinical Guidelines, intravenous thrombolysis is the most effective medical treatment for ischemic stroke in the first 4.5 hours from the onset of symptoms (level of evidence 1, grade of recommendation A) [3,8,27,31]. Currently, due to the greater effectiveness of thrombolytic therapy compared to other methods of treatment in the acute period of stroke, as well as based on pharmacoeconomic data, significant efforts are being made all over the world to use one or another method of reperfusion as often as possible [32,33].
According to a review of recent studies, the indications for thrombectomy have been expanded: in some patients with a major stroke: mechanical thrombectomy can be safely performed up to 16 hours after a stroke. Under certain conditions, based on advanced brain imaging data, the interval may be extended up to 24 hours in some patients. In previous manuals, the limit was only six hours. The indications for neuroimaging have also been expanded in certain aspects, as well as the timing of its implementation has been reduced. The section on recommendations for prescribing antiplatelet therapy was supplemented with information that in patients with small stroke, dual antiplatelet therapy (aspirin and clopidogrel) for 21 days, which was started within 24 hours of symptom onset, may be useful for early secondary prevention of stroke up to 90 days from the onset of symptoms [4-6,53-58].
Neuroprotection in ischemic strokes in Russia
The «Vyshkovsky Index» is a leading market indicator that allows real-time evaluation of the effectiveness of advertising campaigns and forecasting changes in drug sales volumes, but also influencing these indicators. Since 2000, the information portal www.rlsnet.ru has been supporting the Russian Medicines Register (RMR), which is intended for a wide range of professionals in the field of healthcare and drug circulation. The resource contains only official information about medical products approved for use in Russia, as well as a number of unique services and opportunities for obtaining complete and reliable information about drugs. According to Yandex, site traffic is more than 18 million user visits per month. Thus, the idea of the «Wyshkovsky Index» is simple: before buying or prescribing a medicine, information is collected about it. Consequently, the fall in the index of information demand indicates that after some time its sales will also decrease. Rapid monitoring of demand, made possible by Internet technologies, allows you to see trends in demand in advance and provide the necessary marketing influences.
An analysis of the information portal www.rlsnet.ru shows that at present there is no universally recognized neuroprotection program that has proven effective in improving the outcome of the disease. In the Russian Federation, there is a large empirical experience in the use of neurocytoprotectors in ischemic stroke [23-29]. For most drugs in this group, the safety of their use has been successfully demonstrated [9-25]. New technologies of reperfusion therapy in the first hours of ischemic stroke are being actively introduced in the Russian Federation, qualitatively changing approaches to patient management, significantly improving disease outcomes and causing a decrease in mortality and a highly significant increase in the number of people with a good recovery of impaired neurological functions. In the Russian Federation, the methods of systemic and selective intra-arterial thrombolysis were first introduced in the clinic of the Research Institute of Cerebrovascular Pathology and Stroke of the Russian State Medical University. N.I. Pirogov on the basis of City Clinical Hospital No. 31 in 2005–2006. Since 2008, thrombolysis has been an integral part of providing medical care to patients with stroke in the conditions of regional and primary vascular departments. As part of the implementation of a set of measures to reduce mortality from vascular diseases, it is included in the current “Clinical guidelines for the management of patients with cerebral infarction (ischemic stroke) and transient ischemic attacks (2015)”. Intravenous thrombolytic therapy for patients with verified ischemic stroke is indicated if the time from the onset of the first symptoms of the disease to the start of treatment does not exceed 4.5 hours, and the patient’s age is in the range from 18 to 80 years [23–29].
In addition to the above, the updated Clinical guidelines for the management of patients with ischemic stroke and transient ischemic attacks, developed in 2015 jointly with the National Stroke Association, the All-Russian Society of Neurologists, the Association of Neurosurgeons of Russia, the interregional public organization “Association of neuroanesthesiologists and neuroresuscitators”, and also by the Union of Rehabilitologists of Russia, special attention is paid to neuroprotection [26–29]. The current edition highlights two areas, one of the mechanisms of neuroprotection is aimed at interrupting the rapid processes of necrotic cell death associated with the activity of the glutamate-calcium cascade. The second direction of neuroprotection is to reduce the severity of the “long-term consequences” of ischemia: oxidative stress, excessive NO synthesis, microglia activation, cytokine imbalance, immune changes, local inflammation, microcirculation disorders, trophic dysfunction and apoptosis, which underlie the delayed death of nervous tissue cells.
The widespread use of thrombolysis in clinical practice is hampered by a significant number of restrictions and contraindications, as well as the high cost of treatment. For example, in the United States, thrombolysis for stroke has been used for a longer time than in Europe, and American neurologists lead the world in terms of the absolute number of procedures performed. However, the share of patients treated by this method accounts for a little more than 4% of the total number of patients with cerebral infarction. Currently, in the Russian Federation, thrombolysis is performed in approximately 2.5% of patients with a confirmed diagnosis of ischemic stroke. The territorial feature of Russia is the large extent of the country and the uneven distribution of the population over a large area - low population density and its concentration in large and small administrative centers, such as in Siberia and the Far East, which does not favor the delivery of stroke patients to a vascular center within «therapeutic window» that allows for thrombolytic therapy.
As a neuroprotective therapy in the Russian Federation, Mexidol (ethylmethylhydroxypyridine succinate, NPK Farmasoft LLC, RF), Actovegin (deproteinized calf blood hemoderivative, RU: Takeda Pharmaceuticals LLC, Austria), Cerebrolysin (International non-proprietary name (INN) - no, RU: EVER Neuro Pharma GmbH, Austria), and “Citicoline” (INN - ceraxon, RU: Ferrer International S.A., Spain). Ethylmethylhydroxypyridine succinate, cerebrolysin and ceraxon are included in the current standards for managing patients with ischemic stroke (Order of the Ministry of Health of the Russian Federation dated December 29, 2012 No. 1740n “On approval of the standard for specialized medical care for cerebral infarction”). All of the above drugs are included in the Clinical Guidelines for the Management of Patients with Transient Ischemic Attacks and Cerebral Infarction, valid in the Russian Federation, with varying degrees of evidence, including the highest in this group - the level of persuasiveness B, the level of significance 2A. Despite the fact that the “historical homeland” of actovegin and cerebrolysin is Austria, where, among other things, production sites are currently located, and Spain is the “homeland” of citicoline, these drugs, for various reasons, are not widely prescribed in Europe, are not included in the European and American clinical guidelines for the management of patients with stroke and are not approved for use by the FDA (USA). Thus, the management of patients with cerebral infarction has a territorial specificity. Pharmacological neuroprotection of patients with stroke has not found wide distribution in other countries and refers to the so-called RSD (Russian Specific Drugs), prescribed in the Russian Federation at all stages of medical care for patients with ischemic stroke: pre-hospital, hospital and rehabilitation, which is enshrined in the regulatory legal framework – Standards and Clinical Guidelines. The same RSD group includes neuroprotective drugs from foreign manufacturers, for which the territory of the Russian Federation and the CIS countries is the main market. Neuroprotection in the Russian Federation is a local original history, formed by the empirical experience of many generations of specialists. At the same time, this does not exclude the formation of an evidence base for drugs with a neuroprotective effect, taking into account the requirements of evidence-based medicine, the specifics of the mechanism of action of neuroprotectors, and taking into account their role in the pathogenesis of ischemic brain lesions.
Hemorrhagic stroke and cerebral hemorrhage
General approaches in the treatment of hemorrhagic stroke and cerebral hemorrhage. Hemorrhagic stroke accounts for about 20% of all strokes, with intracerebral hemorrhage (ICH) being the most common type. The frequency of ICH increases in the absence of treatment of arterial hypertension. The ICH, in particular, has a disproportionate risk of early mortality and long-term disability. Until recently, studies on hemorrhagic stroke and hemorrhage were insufficient to analyze and evaluate the effectiveness of various methods for preventing early death in ICH, including urgent correction of blood pressure, elimination of coagulopathy, and surgical evacuation of the hematoma. However, evidence-based guidelines exist for ICH and they form the basis of treatment. Current approaches emphasize the control of extremely high blood pressure in the acute phase, rapid withdrawal of vitamin K antagonists, and surgical evacuation of the hemorrhage. Unresolved issues, many of which are the subject of ongoing clinical research, include the optimization of individual blood pressure targets, strategies for stopping new anticoagulants, and the role of minimally invasive surgery [61]. In medicine, the term stratification is used to divide patients with different risks of developing a particular complication into different groups. In the case of ICH, there are risk stratification models that are based on the results of clinical examination and neuroimaging. However, virtually all physicians have been warned to be careful to avoid a self-fulfilling prophecy of poor outcomes resulting from inadequate treatment.
A preselected “poor prognosis” may affect the outcome of treatment of patients with ICH [61]. Cerebral venous thrombosis is an additional subtype of hemorrhagic stroke that has a unique set of causes, natural course, and treatment. Other common causes include cerebral amyloid angiopathy, overuse of pharmaceutical sympathomimetic drugs, and underlying cerebral vascular abnormalities. Validated baseline predictors of clinical outcome after ICH include Glasgow Coma Scale score, hematoma volume, presence and number of intraventricular hemorrhage, infratentorial ICH location, and advanced age [59]. There is currently no proven effective treatment for ICH. However, several recent large clinical trials have demonstrated the feasibility of surgical and medical treatment of ICH. Clinical studies of the mechanisms of brain injury have shown that hematoma expansion is common even in patients without coagulopathy. It has been established that damage to the perihematoma is most likely associated with the toxicity of serum albumin and iron in the brain (“neurohemo-inflammation”) [59,60], and not with primary ischemic damage. Current recommendations for the treatment of ICH focus on blood pressure control, urgent and rapid correction of coagulopathy, and surgery for cerebellar ICH. Clinical trials are also investigating surgical evacuation of lobar hemorrhage, minimally invasive surgical evacuation of hematoma, and aggressive blood pressure reduction [60]. Spontaneous intracerebral hemorrhage (SICH) in the absence of trauma or surgery often results from a blood clot in the brain parenchyma. This condition accounts for 10 to 15% of all strokes and is associated with a higher mortality rate than ischemic stroke or subarachnoid hemorrhage. Common causes include hypertension, amyloid angiopathy, coagulopathy, vascular abnormalities, tumors, and various drugs. However, arterial hypertension remains the most significant modifiable risk factor for SIMV. Computed tomography is the initial diagnostic method of choice for this type of disease. Therefore, angiography should be considered in all cases except those that include elderly patients with preexisting hypertension due to thalamic, putamenial, or cerebellar hemorrhage. Medical treatment includes prevention of venous thrombosis, gastric cytoprotection, and aggressive rehabilitation. The choice of surgical or conservative treatment for patients with spontaneous intracerebral hemorrhage is controversial. Several minimally invasive treatments have been used to evacuate the hematoma and may improve prognosis to some extent. However, there is still insufficient research on minimally invasive surgery in patients with spontaneous intracerebral hemorrhage.
Anticonvulsants should be prescribed for supratentorial spontaneous intracerebral hemorrhage - Spontaneous Intracerebral Hemorrhage (SICH), while the treatment of arterial hypertension remains controversial [62,63]. To date, nine prospective, randomized controlled trials have been conducted to compare surgical and medical treatments for SICH. Although there is no definitive evidence in favor of surgery, there is a good theoretical rationale for early surgery. Surgery should be considered in patients with moderate to large hemorrhages in the lobes or basal ganglia, and in patients with progressive neurological deterioration. Elderly patients with a Glasgow Coma Score less than 5, patients with brainstem bleeds, and patients with minor bleeds usually do not benefit significantly from surgery. Patients with cerebellar hemorrhage greater than 3 cm, with brainstem compression and hydrocephalus, or with neurological impairment should have a thrombus removed surgically [62-64].
Operate or treat conservatively: that is the question? In the treatment of famous people, the entire arsenal of tools that can prolong the life of a patient is used, and medicine receives invaluable data for the treatment of patients in a borderline condition. The occurrence of spontaneous intracerebral hemorrhage in Israeli Prime Minister Ariel Sharon attracted close attention of local and international media to neurosurgeons who made decisions: to operate or treat conservatively. In the public debate that followed, it was suggested that the emergency measures (surgical treatment) were taken only because of the fame of the patient.
Brief history of the medical problem in A. Sharon. On January 4, 2006, Israeli Prime Minister Ariel Sharon collapsed while inside the Government Chancellery. He was urgently hospitalized at the Hadassah Medical Center - Hebrew University in Jerusalem due to severe intracranial hemorrhage. In the hospital, A. Sharon came to his senses. After the tests, he was diagnosed with a microstroke. Ariel Sharon was then diagnosed with a massive hemorrhagic stroke. After many hours of neurosurgical surgery, during which the doctors managed to stop the bleeding, Sharon was hospitalized in the intensive care unit. His condition was assessed as “stably serious”[65]. After that, he required intensive care for 5 months and additional procedures. The medical problem that arose with the VIP was fraught with organizational and administrative difficulties.
Delivering emergency care to a major government official requires medical staff to handle many administrative issues while providing the VIP patient with appropriate intensive medical care. The papers [66–68] present a strategy for solving these problems. It includes all possible approaches, including surgical methods and conservative treatment. Therefore, if possible, then there should be no question: operate or treat conservatively. For 8 years, doctors fought for the life of Israeli military, political and statesman Ariel Sharon. In early January 2014, the condition of the 85-year-old former politician deteriorated significantly. Against the background of renal failure, doctors began to record the failure of other vital organs. At this time, the former prime minister reacted to the recording of the voices of relatives and to touch, and special tests revealed increased activity of his brain. Ariel Sharon died on January 11, 2014.
Ischemic and hemorrhagic stroke at the cellular level
Previously, recent biomedical advances have been reviewed that may provide new and more effective strategies for the treatment of acute stroke. It was also pointed out that global lifestyle modification to prevent strokes, improve health and increase life expectancy should be the main strategy in the 21st century. Below, an analysis of the main changes at the cell level in the modeling of ischemic and hemorrhagic stroke will be given and a general concept of the development of pathological processes will be proposed, which can be the main component of a typical pathological process.
Ischemic stroke is, first of all, a massive focal death of nerve cells by the mechanism of necrosis or apoptosis. It is not by chance that it is called a cerebral vascular catastrophe. A hallmark of a stroke is the irreversible nature of the damage or “loss” of brain functions associated with the affected area. Epidemiological studies of recent decades indicate that acute ischemic cerebrovascular accidents continue to dominate in the structure of all cerebrovascular disorders, and develop approximately 4 times more often than cerebral hemorrhage. The treatment of ischemic stroke is much more complex than the treatment of hemorrhagic stroke. This is primarily due to the significant heterogeneity of the pathogenetic mechanisms underlying it. Early detection of the leading mechanism of cerebral ischemia is of fundamental importance for creating the right strategy for treating the patient.
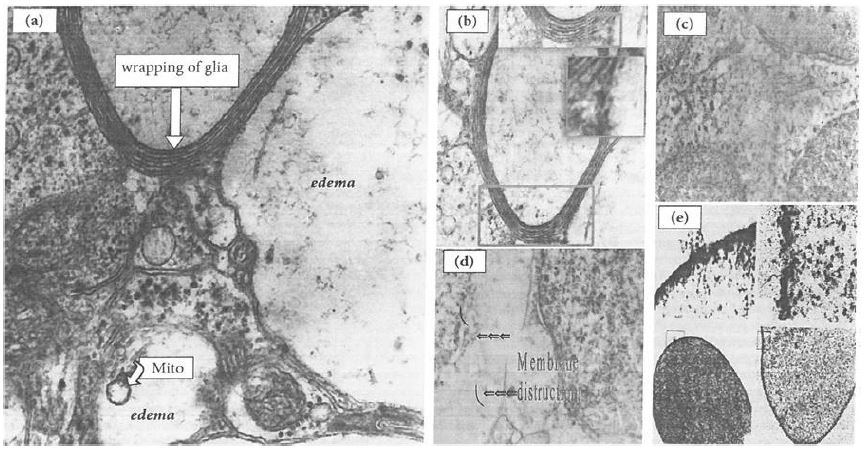
Figure 1: Nonspecific disorders and lesions in cells and subcellular structures.
(a) edema and (b–e) local membrane lesions: (b) alterations in glial cells, which form multilayer wrappings around the areas of edema and neuronal damage (damage areas are shown in insets); (c, d) alterations in a layer of cerebellar granule cells (from local lesions to cell fusions); (e) a redistribution of proteins from a soluble state to a membrane-associated state in erythrocytes and local damage to erythrocyte membranes [81,82].
Currently, it has been revealed that these events are caused by a cascade of the following main reactions and mechanisms: a) cessation or a sharp reduction in blood supply; b) an increase in the content of glutamate (Glu-neurotoxicity); c) violation of the energy mechanisms of a part of the brain tissue and ion homeostasis, primarily the content of Ca2+ and Na+ ions; nitrosative and oxidative stress (a sharp increase in the content of active forms of nitrogen (ANS) and oxygen (AOS)); conditions of acute oxygen starvation (hypoxia / ischemia); d) the development of inflammatory processes (against the background of the activation of inducible NO-synthase and the formation of NO2 and OH-radicals); intoxication with metabolic products, irreversible changes in the core of a stroke/infarction that occur during the first 15-30 minutes or become so massive that it always affects neurons, glial cells, the totality of the main functioning elements of the brain specialized for performing any tissue tasks [69-71]. The leading role in the protection of nerve cells belongs to regulatory mechanisms, and the development of neuronal damage, in addition to reactive forms of nitrogen and oxygen, belongs to mitochondrial dysfunction. Maintaining blood circulation and structural and functional activity of mitochondria of nerve cells is the basis of neuroprotection.
Hemorrhagic stroke is an acute cerebrovascular accident with vascular rupture against the background of impaired cerebral blood flow regulation systems and cerebral hemorrhage [70–77]. The most common cause of hemorrhagic strokes is a violation of the functioning of the walls of blood vessels - endothelium, intima – against the background of arterial hypertension, hypertension, congenital and acquired aneurysms of cerebral vessels. Intracerebral hemorrhage and hemorrhagic stroke are the most common type of stroke, which most often occurs in middle and old age, in people with hypertension, cerebral atherosclerosis, or a combination of these diseases. Hemorrhagic stroke differs from ischemic stroke in that the rupture of the vessel occurs at high blood pressure. With such a stroke, high-pressure blood pushes the brain tissue apart and fills the resulting cavity.
Subarachnoid hemorrhage is a hemorrhage into the subarachnoid space (a cavity between the arachnoid and pia mater), which can occur as a result of a rupture of an arterial aneurysm, a hemorrhagic stroke, or as a result of a traumatic brain injury [78]. In all cases considered, the main pathogenic effect is damage to cell membranes, vessel walls, which are accompanied by hemorrhages, contact of serum albumin with fatty acids that are part of damaged membranes, binding of these fatty acids by serum albumin, and further destruction of the membranes of neurons, glial cells, and subcellular structures (for example, mitochondria) [79]. These damages underlie the disruption of ion homeostasis, lead to the development of edema, and end with the death of neurons and glial cells [78, 79].
Such damages are based on free radical oxidation of unsaturated fatty acids that are part of membrane lipids, local damage to cell membranes and subcellular structures, which culminate in partial necrosis of individual brain structures [78,79].
Ischemia in acute stroke is often incomplete. This is due to the fact that the collateral blood supply enters the affected part of the brain from intact arteries. Irreversible changes in neurons and glial cells occur in the central zone with ischemia/hypoxia, the most pronounced decrease in blood flow (less than 10 ml/100 g per 1 min), impaired glucose and oxygen metabolism [41, 42]. Within a few hours, a central (“point”) infarction occurs, which is surrounded by living tissue in a state of hypoxia / ischemia with a blood flow level above 20 ml / 100 g per 1 min - the zone of “ischemic penumbra” [41-45]. With brain damage caused by hypoxia/ischemia, cerebrovascular accident, stroke or trauma, an irreversibly affected infarct nucleus is also formed, which is characterized by extremely weak blood circulation, and zones with impaired metabolism develop around the damage sites, which, as mentioned above, are called "penumbra".
Conclusions
The very first minutes and hours during strokes, as a rule, remain out of sight of researchers and doctors. However, it is at this time that the irreversible death of nerve cells occurs, which will affect functional outcomes and determine survival after a stroke. Over the past decades (1990-2020), as mentioned above, the absolute number of stroke cases in the world increased by 70%, patients after stroke increased by 85%, stroke mortality increased by 43%, and DALY (Disability Adjusted Life Years) - the integral medical and economic indicator due to stroke increased by 32%. In Russia, the number of cases of stroke in recent decades has amounted to 340 people per 100 thousand population per year. This means that approximately every 1.5 minutes a Russian develops this disease, and the mortality rate from it remains one of the highest in the world. More than 1 million people who have had a stroke live in the Russian Federation. After a stroke in the Russian Federation, almost every second patient dies by the end of the first year, and after 7 years, almost 80% of patients die. In case of inpatient treatment of strokes in Russia, the mortality rate is 20%. Mortality in outpatient treatment can reach 67%. The same indicator in nursing homes is 90%, and in the absence of medical care - 98.8%. For ischemic stroke, this figure averages from 15 to 20%. Mortality in hemorrhagic stroke is much higher – about 60%.
Declarations
Author Contributions: Conceptualization, R.V.; methodology, R.V. and S.E., format analysis R.V. and S.E.; writing – original draft preparation, R.V.; writing – review and editing, R.V. and S.E.
All authors have read and agreed to the published version of the manuscript.
Funding: This work was supported by Russian Academy of Sciences.
Competing interests: The authors have no conflict of interest to declare.
Conflicts of Interest: The authors declare no conflict of interest.
Data Availability Statement: The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- Gállego J, Herrera M, Jericó I, Muñoz R, Aymerich N, et al. Stroke in the XXI century. Emergency care. An Sist Sanit Navar. 2008; 31: 15-29.
- Clark B, Whitall J, Kwakkel G, Mehrholz J, Ewings S, et al. The effect of time spent in rehabilitation on activity limitation and impairment after stroke. Cochrane Database Syst Rev. 2021; 10.
- Ceulemans AG, Zgavc T, Kooijman R, Hachimi-Idrissi S, Sarre S, et al. The dual role of the neuroinflammatory response after ischemic stroke: modulatory effects of hypothermia. J Neuroinflammation. 2010; 7: 74.
- Tobaldini E, Proserpio P, Oppo V, Figorilli M, Fiorelli EM, et al. Cardiac autonomic dynamics during sleep are lost in patients with TIA and stroke. J Sleep Res. 2020; 3: 12878.
- Oddo M, Crippa IA, Mehta S, Menon D, Payen JF, et al. Optimizing sedation in patients with acute brain injury. Crit Care. 2016; 20: 128.
- Centers for Disease Control and Prevention (CDC). Awareness of stroke warning signs-17 states and the U.S. Virgin Islands. 2001; MMWR Morb Mortal Wkly Rep. 2004; 53: 359-362.
- Centers for Disease Control and Prevention (CDC). Awareness of stroke warning symptoms-13 States and the District of Columbia. 2005; MMWR Morb Mortal Wkly Rep. 2008; 57: 481-485.
- Yuan J, Li M, Liu Y, Xiong X, Zhu Z, et al. Analysis of Time to the Hospital and Ambulance Use Following a Stroke Community Education Intervention in China. JAMA Netw Open. 2022; 5: e2212674.
- Wang YJ, Li ZX, Gu HQ, Zhai Y, Jiang Y, et al. China Stroke Statistics 2019 Writing Committee. China Stroke Statistics 2019: a report from the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations. Stroke Vasc. Neurol. 2020; 5: 211-239.
- Zhao J, Liu R. Stroke 1-2-0: a rapid response programme for stroke in China. Lancet Neurol. 2017; 16: 27-28.
- Wang Y, Liu Y, Liu R, Zhao J. Cluster-randomised controlled trial of Stroke 1-2-0 education programme to reduce stroke prehospital delay in China: a study protocol. BMJ Open. 2021; 11: e048064.
- Zhou M, Wang H, Zeng X, Yin P, Zhu J, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2019; 394: 1145-1158.
- Wu S, Wu B, Liu M, Wang W, Anderson CS, et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 2019; 18: 394-405.
- Liu S, Li Y, Zeng X, Wang H, Yin P, et al. Burden of cardiovascular diseases in China, 1990-2016: findings from the 2016 global burden of disease study. JAMA Cardiol. 2019; 4: 342-352.
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021; 20: 795-820.
- Ravenell J, Leighton-Herrmann E, Abel-Bey A, DeSorbo A, Teresi J, et al. Tailored approaches to stroke health education (TASHE): study protocol for a randomized controlled trial. Trials. 2015; 19: 176.
- Caprio, FZ, Sorond FA. Cerebrovascular Disease: Primary and Secondary Stroke Prevention. Med Clin North Am. 2019; 103: 295-308.
- Knight-Greenfield A, Nario JJQ, Gupta A. Causes of Acute Stroke: A Patterned Approach. Radiol Clin North Am. 2019; 57: 1093-1108.
- Sihvonen AJ, Leo V, Ripollés P, Lehtovaara T, Ylönen A, et al. Vocal music enhances memory and language recovery after stroke: pooled results from two RCTs. Ann Clin Transl Neurol. 2020; 7: 2272-2287.
- Sihvonen AJ, Pitkäniemi A, Leo V, Soinila S, Särkämö T, et al. Resting-state language network neuroplasticity in post-stroke music listening: A randomized controlled trial. Eur J Neurosci. 2021; 54: 7886-7898.
- Stakhovskaya LV, Klochikhina OA, Bogatyreva MD, Kovalenko VV. Epidemiology of stroke in the Russian Federation: results of territory’s population registry (2009–2010). Zhurnal Nevrologii i Psikhiatrii imeni S.S. Korsakova. 2013; 113: 410.
- Shamalov NA, Stakhovskaya LV, Klochikhina OA, Polunina OS, Polunina EA. An analysis of the dynamics of the main types of stroke and pathogenetic variants of ischemic stroke. Zhurnal Nevrologii i Psikhiatrii imeni S.S. Korsakova. 2019; 119: 510.
- Suslina ZA, Vereshchagin NV, Piradov MA. Subtypes of ischemic disorders of cerebral circulation: diagnosis and treatment. Consilium Medicum. 2001; 3: 218-221.
- Averochkin AI, Averyanov YuN, Alekseev VV etc. Diseases of the nervous system. M. Medicine. 2001; 480.
- Zaslavsky AS. Clinical-epidemiological and medical-social aspects of acute disorders of cerebral circulation in the Komi Republic. Abstract of thesis. 2022; 24.
- Vereshchagin NV, Piradov MA. Stroke: assessment of the problem. Neurological journal. 1999; 4: 4-7.
- Piradov MA, Maksimova My, Tanashyan MM Stroke, step by step instructions. Guide for doctors M: GEOTAR-Media. 2019; 272.
- Klochikhina OA, Stakhovskaya LV. An analysis of epidemiological indices of stroke based on the data of a regional population register from 2009 to 2012. Zhurnal Nevrologii i Psikhiatrii imeni S.S. Korsakova. 2014; 114: 63-69.
- Gusev EI, Skvortsova VI, Platonova IA. Therapy for ischemic stroke. Consilium Medicum. 2003; 5: 466-473.
- Papers presented at the 1st International Conference on Stroke. Geneva, Switzerland. Neurol Res. 1992; 14: 76-213.
- Ceulemans AG, Zgavc T, Kooijman R, Hachimi-Idrissi S, Sarre S, et al. The dual role of the neuroinflammatory response after ischemic stroke: modulatory effects of hypothermia. J. Neuroinflammation. 2010; 7: 74.
- European Stroke Services: From Evidence to Practice. Proceedings of the satellite symposium to the 11th European Stroke Conference. Geneva, Switzerland, May 29-June 1, 2002; Cerebrovasc Dis. 2003; 15: 1-32.
- Sanossian N, Ohanian AG, Saver JL, Kim LI, Ovbiagele B. Frequency and determinants of nonpublication of research in the stroke literature. Stroke. 2006; 37: 2588-2592.
- Thom T, Haase N, Rosamond W, Howard VJ, Rumsfeld J, et al. Heart disease and stroke statistics-2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006; 113: e85-151.
- Rosamond W, Flegal K, Furie K, Go A, et al. Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008; 117: e25-146.
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, et al. Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009; 119: 480-486.
- Schwamm L, Fayad P, Acker JE, Duncan P, et al, Translating evidence into practice: a decade of efforts by the American Heart Association/American Stroke Association to reduce death and disability due to stroke: a presidential advisory from the American Heart Association/American Stroke Association. Stroke. 2010; 41: 1051-1065.
- Saver JL, Wasiak H. Stroke Council and American Stroke Association update. Stroke. 2011; 42: 830-831.
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, et al. Executive summary: heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013; 127: 143-152.
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation. 2014; 129: 399-410.
- Lees KR, Caso V, Fischer U. Organizational Update: Report From the European Stroke Organisation 2015. Stroke. 2015; 46: e214-215.
- Lees KR, Caso V, Michel P. Organizational update: European stroke organisation. Stroke. 2015; 46: e67-8.
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation. 2015; 131: e29-322.
- Derdeyn CP, Broderick JP, Furie K. Organizational Update: American Stroke Association Stroke Council Update. Stroke. 2016. 47: e16-17.
- Rabinstein AA, How Cool It Is: Targeted Temperature Management for Brain Protection Post-Cardiac Arrest. Semin Respir Crit Care Med. 2016; 37: 34-41.
- Testori C, Sterz F, Behringer W, Haugk M, Uray T, et al. Mild therapeutic hypothermia is associated with favourable outcome in patients after cardiac arrest with non-shockable rhythms. Resuscitation. 2011; 82: 1162-1167.
- Writing Group Members, Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, et al. American Heart Association Statistics Committee; Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016; 133: e38-360.
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation. 2018; 137: e67-e492.
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation. 2019; 139: e56-e528.
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020; 141 (9): e139-596.
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation. 2021; 143: e254-743.
- Dichgans M, Sandset EC, Kelly P. Organizational Update From the European Stroke Organisation. Stroke. 2021; 52: e517-e519.
- Sarikaya H, Ferro J, Arnold M. Stroke prevention – medical and lifestyle measures. Eur Neurol. 2015; 73: 150-157.
- Gibson E, Koh CL, Eames S, Bennett S, Scott AM, Hoffmann TC Occupational therapy for cognitive impairment in stroke patients. Cochrane Database Syst. Rev. 2022; 3: CD006430.
- Caprio FZ, Sorond FA. Cerebrovascular Disease: Primary and Secondary Stroke Prevention. Med Clin North Am. 2019; 103: 295-308.
- Li J, Wang J, Shen Y, Dai C, Chen B, et al. Hyperoxygenation With Cardiopulmonary Resuscitation and Targeted Temperature Management Improves Post-Cardiac Arrest Outcomes in Rats. J Am Heart Assoc. 2020; 9: e016730.
- Johnston SC, Easton JD, Farrant M, Barsan W. Clinical Research Collaboration, Neurological Emergencies Treatment Trials Network, and the POINT Investigators. Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA. N Engl J Med. 2018; 379: 215-225.
- Khaku AS, Tadi P. Cerebrovascular Disease. 2021. In: StatPearls. Treasure Island (FL): Stat. Pearls Publishing; 2022.
- Elijovich L, Patel PV, Hemphill JC. Intracerebral hemorrhage. Semin Neurol. 2008; 28: 657-667.
- Fewel ME, Thompson BG, Hoff JT. Spontaneous intracerebral hemorrhage: a review. Neurosurg Focus. 2003; 15: E1.
- Montaño A, Hanley DF, Hemphill JC. Hemorrhagic stroke. Handb Clin Neurol. 2021; 176: 229-248.
- Hoffman H, Jalal MS, Chin LS. Prediction of mortality after evacuation of supratentorial intracerebral hemorrhage using NSQIP data. J Clin Neurosci. 2020; 77: 148-156.
- de Oliveira Manoel AL. Surgery for spontaneous intracerebral hemorrhage. Crit Care. 2020; 24: 45.
- Dasenbrock HH, Smith TR, Rudy RF, Gormley WB, Aziz-Sultan MA, et al. Reoperation and readmission after clipping of an unruptured intracranial aneurysm: a National Surgical Quality Improvement Program analysis. J Neurosurg. 2018; 128: 756-767.
- Naparstek Y. Ariel Sharon’s illness: should we dedicate a medical journal issue to a single case study? Isr Med Assoc J. 2006; 8: 739-740.
- Weiss YG, Mor-Yosef S, Sprung CL, Weissman C, et. al. Caring for a major government official: challenges and lessons learned. Crit Care Med. 2007; 35: 1769-1772.
- Dubler NN, Kalkut GE. Caring for VIPs in the hospital: the ethical thicket. Isr Med Assoc J. 2006; 8: 746-750.
- Blachar Y, Borow, M. The health of leaders: information, interpretation and the media. Isr Med Assoc J. 2006; 8: 741-743.
- Yaghi S, Willey JZ, Cucchiara B; Goldstein JN et al. American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Council on Quality of Care and Outcomes Research. Treatment and Outcome of Hemorrhagic Transformation After Intravenous Alteplase in Acute Ischemic Stroke: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2017; 48: e343-e361.
- Khodorov BI. Mechanisms of destabilization of Ca2+-homeostasis of brain neurons caused by toxic glutamate challenge. Membr. Cell Biol. 2000; 14: 149-162.
- Efremov YM, Grebenik EA, Sharipov RR, Krasilnikova IA, et al. Viscoelasticity and Volume of Cortical Neurons under Glutamate Excitotoxicity and Osmotic Challenges. Biophys J. 2020; 119: 1712-1723.
- Sorokina EG, Semenova ZB, Reutov VP, Arsenieva EN, et al. Brain Biomarkers in Children After Mild and Severe Traumatic Brain Injury. Acta Neurochir Suppl. 2021; 131: 103-107.
- Sorokina EG, Semenova ZB, Averianova NS, Karaseva OV et al. APOΕ gene polymorphism and markers of brain damage in the outcomes of severe traumatic brain injury in children. Zh Nevrol Psikhiatr Im S S Korsakova. 2020; 120: 72-80.
- Lundberg JO, Gladwin MT; Ahluwalia A, Benjamin N, Bryan NS, et al. Nitrate and nitrite in biology, nutrition and therapeutics. Nat Chem Biol. 2009; 5: 865-869.
- Kuzenkov VS, Krushinskii AL, Reutov VP. Effect of cation type and concentration of nitrates on neurological disorders during experimental cerebral ischemia. Bull Exp Biol Med. 2013; 155: 748-751.
- Menshikova EB, Zenkov NK, Reutov VP. Nitric oxide and NO-synthases in mammals in different functional states. Biochemistry (Mosc). 2000; 65: 409-426.
- Salykina MA, Sorokina EG, Krasilnikova IA, Reutov VP, Pinelis VG. Effects of selective inhibitors of neuronal and inducible NO-synthase on ATP content and survival of cultured rat cerebellar neurons during hyperstimulation of glutamate receptors. Bull Exp Biol Med. 2013; 155: 40-43.
- Samosudova NV, Reutov VP, Larionova NP, Chailakhyan LM. Neuron-glial contacts formed in the cerebellum during electrical stimulation in the presence of an NO-generating compound. Neurosci Behav Physiol. 2008; 38: 363-368.
- Reutov VP, Baĭder LM, Kuropteva ZV, Krushinskiĭ AL, Kuzenkov VS, et al. Experimental hemorrhagic stroke: the effect of the peptide preparation cortexin in the formation of Hb-NO-complexes and other blood paramagnetic centers. Zh. Nevrol. Psikhiatr. Im. S.S. Korsakova. 2011; 111: 56-61.
- Kuropteva ZV, Reutov VP, Baider LM, Krushinsky AL. Complexes of nitric oxide with hemoglobin and paramagnetic metalloenzymes in the brain and blood of mammals after intermittent hypoxia. Zh Nevrol Psikhiatr Im S S Korsakova. 2016; 116: 9-16.
- Reutov VP, Samosudova NV, Sorokina EG. A model of glutamate neurotoxicity and mechanisms of the development of the typical pathological process. Biophysics. 2019; 64: 233-250.
- Samosudova NV, Reutov VP. Ultrastructural changes in the frog brain in the presence of high concentrations of glutamate and an NO-generating compound. Biophysics. 2018; 63: 402-415.
