
Open Access, Volume 9
Effect of Chinese Traditional Medicine enema recipe on tight junction of intestinal epithelial cells in rats with chronic renal failure
Wenbin Tang1#; Xiao Liu2#; Yuanyuan Cui2; Wenmin Dai2; Dilixiati Alimu2; Weiwei Song2; Qianqian Qian2; Zhiwu Lu3; Hong Jiang4*; Zhanjun Shu5*
1Department of Nephrology, Xiangya First Affiliated College of Central South University, Changsha 410000, Hunan Province, China.
2Infectious Diseases and Nephropathy, The Fourth Clinical College of Xinjiang Medical University, Urumqi 830000, China.
3Infectious Diseases and Nephropathy, The Eighth Affiliated Hospital of Xinjiang Medical University, Urumqi 830000, China.
4Department of Nephrology, The People`s Hospital of Xinjiang Uygur Autonomous Region. Urumqi 830000, Xinjiang Province, China.
5National Clinical Research Base of Traditional Chinese Medicine, The Fourth Clinical College of Xinjiang Medical University, Urumqi 830000, China.
#These authors contribute equally to this work.
Hong Jiang
Department of Nephrology, the People’s Hospital of Xinjiang Uygur Autonomous Region, No. 91, Tianchi Road, Tianshan District, Urumqi 830001, Xinjiang, China.
Zhanjun Shu, National Clinical Research Base of Traditional Chinese Medicine, The Fourth Clinical College of Xinjiang Medical University, Urumqi 830000, China.
Tel: +86- 0991-5572210; +86- 0991-8562574;
Email: shu5857872@163.com & 2328207223@qq.com
Received : April 05, 2023,
Accepted : May 17, 2023
Published : May 23, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Purpose: The aim of this study was to observe the changes in structure and function of tight junction in intestinal epithelial cells after Traditional medicine treatment.
Methods: Models of chronic renal failure were established, and then divided based on operation and Chinese medicine intervention. The levels of BUN and Cr in blood samples, and urea nitrogen and creatinine in feces samples were determined by automatic biochemical analyzer. RT-PCR, Western blot and Immunohistochemistry assay were processed to detect the expression level of Claudin-1, Occludin and ZO-1. Hematoxylin-eosin staining assay, Periodic Acid-Silver Metheramine (PASM) staining assay and Masson staining assay were processed to determine the structure and function of tight junction in intestinal epithelial cells.
Results: Compared with the sham operation group, the expression of Claudin-1, Occludin and ZO-1 in the ascending colon of the surgical group model animals was significantly reduced. However, the expression of tight junction-associated genes in the operation + Chinese medicine intervention group was increased. In operation group, more glomerular volume was reduced, and some glomerular structures were destroyed and disappeared. Partially proximal tubules were with severe vacuolar degeneration and epithelial atrophy, and brush-like edges were disappeared. Unstructured protein tube type and more red blood cells were found in partial lumen. Renal interstitial granules were infiltrated in more chronic inflammatory cells with fibrous tissue hyperplasia. After Chinese medicine intervention, the lesion has a certain degree of improvement.
Conclusion: Chinese medicine intervention could increase the expression of Claudin-1 and Occludin, and also restored the histomorphological changes of CKD.
Keywords: Traditional medicine; Chronic renal failure; Tight junction; Intestinal epithelial cells.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Jiang H (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Tang W, Liu X, Cui Y, Dai W, Alimu D, Jiang H, Shu Z, et al. Effect of Chinese Traditional Medicine enema recipe on tight junction of intestinal epithelial cells in rats with chronic renal failure. Open J Clin Med Case Rep. 2023; 2041.
Introduction
Chronic Kidney Disease (CKD) is one of the public health problems of concern worldwide [1]. The incidence of CKD in Western countries has reached 11%-15%, and the situation in China is not optimistic [2]. A large number of studies have confirmed that 5% of CKD patients will eventually enter Chronic Kidney Failure (CRF) [3]. In the development of Phase 1 to Phase 5, there are fewer current clinical interventions [4]. In the fifth phase of CRF, it can only be treated by hemodialysis, peritoneal dialysis and kidney transplantation [5].
At present, hemodialysis and peritoneal dialysis treatments are costly [6]. Especially in countries and regions with underdeveloped economy, patients are unable to bear the economic burden. Moreover, there are still many medical problems that are difficult to solve in dialysis treatment. In United States, the dialysis patients have a 3-year mortality rate of 50% [7]. Due to legislative reasons in various countries, the tight supply and demand of kidney source has brought great difficulties to kidney transplantation.
Therefore, it is particularly important to delay the development of Phase 1 of CRF patients to Phase 5. Contemporary Chinese medicine has made many beneficial attempts in clinical application of intestinal tract, colon dialysis, anal sphincter, anal drip and other intestinal routes to delay the progression of CRF [8]. In modern medical research, Traditional medicine is treated with intestinal tract CRF based on the following theoretical basis. The concentration of solute in the body depends on the regulation between the clearance and production of the solute [9]. As the glomerular filtration rate decreases, the solute removal in the blood tends to decrease [10]. This adjustment is largely done in the intestines. There are more than one hundred kinds of common uremic toxins. When the renal excretion function declines, most of the toxins in the blood will spread directly into the intestine through the intestinal mucosa [11]. At the same time, some toxins enter the body after being produced in the intestine, such as glycation end products, bismuth, phenols, etc [12]. Studies have shown that Traditional medicine could reduce the levels of toxins such as urea, creatinine and molecular substances in patients with CRF [8]. Traditional medicine shows a certain effect on the progress of CRF, but its mechanism and therapeutic targets are not clear.
In our early study of Traditional medicine in the intestinal model of chronic renal failure, a significant change occurred in the intestinal flora (Figure 1). From the perspective of Division, the distribution of thick-walled bacteria, Bacteroidetes, Proteobacteria, and actinomycetes in intestinal flora were with meaningful changes after the intervention of traditional Traditional medicine. In the renal failure group, the thick-walled bacteria had an increasing trend after intervention, and even recovered to a level similar to or higher than normal, while the Bacteroides, Proteobacteria, and actinomycetes were reduced to normal levels or even lower. Studies have shown that thick-walled bacteria have a role in malnutrition in patients with chronic renal failure, and actinomycetes have an effect on the nitrogen cycle. At the taxonomic level of the genus, it can be seen that after the intervention of traditional Chinese medicine, the lactic acid bacteria, the genus Streptococcus, the genus Bacteroides, the Bacteroides, the Bifidobacterium, the rumen bacteria have meaningful changes. These above genus have important effects on nutrient absorption, control of toxins in the body, liver protection and immune regulation. The above results allow us to see a glimmer of light in the intervention of traditional Chinese medicine in the intestinal intervention of chronic renal failure, but whether this method has an impact on intestinal structure and function remains to be further studied and explored.
In this study, traditional Chinese medicine intestine treatment was performed to CRF rat model, Real-time PCR, Western blot, laser scanning and renal pathological examination were used to observe the changes in structure and function of tight junction proteins in intestinal epithelial cells, and also changes in renal pathology before and after treatment. In-depth study of Traditional medicine intervention in intestinal epithelial cell tight junctions may provide new mechanisms of action and therapeutic targets for delaying the progress of CRF.
Materials and methods
Establishment of a model of chronic renal failure and grouping of experimental animals
A total of 40 Spragua-Dawley rats (6 weeks of age, male or female, weighted 200-220g) were provided by Animal Laboratory of Xinjiang Medical University, and randomly divided into 4 groups: sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4). Four groups of rats were fed normally, and the feeding methods and food were consistent.
The surgical procedure is briefly introduced as follows: For sham operation, only anesthesia, renal capsule peeling and exposure were processed, bilateral kidneys are not removed. The rats were anesthetized by intraperitoneal injection of 10% chloral hydrate. A 2 cm longitudinal incision was cut on the lower third of the left back, the left kidney was exposured, and the renal capsule was separated. The upper and lower 1/3 of the left kidney were ligated and removed, and the adrenal gland was reserved. Gelatin sponge was used to stop bleeding, and layer suture was processed. After 4 weeks, the right kidney was excised and a 5/6 nephrectomized rat model was prepared. The excised kidney tissue was weighed, and the resection rate was calculated by the ratio of the left kidney tissue to the right kidney weight. The average resection rate of the kidney in this experimental group was about 70%. After operation, the rats were injected with penicillin 2-3 million u/day for 3 days to prevent infection.
Traditional medicine intervention was produced as follows. The Chinese medicine contained Liquor rhubarb (20 g), dandelion (15 g), calcined oyster (15 g) and blood charcoal (15 g). The above drugs were decocted, filtered and concentrated to 2.6 g crude drug per ml, and stored in a refrigerator at 4°C. The Traditional medicine was provided and uniformly decoctioned by Department of Pharmacy, Affiliated Hospital of Xinjiang Medical University. Traditional medicine enema were processed, the amount of rats was 10 g/kg and once/day for 4 weeks.
Acquisition and measurement of blood and feces samples
After the intervention, blood and feces specimens of all rats were taken in the morning at 1, 2 and 4 weeks. Under sterile conditions, 1 g feces samples was weighted with an electronic weighing device, dissolved and mixed well by 10 ml of distilled water, and centrifuged at 3000 rpm for 10 minutes at room temperature. 0.4 ml of the supernatant were taken and stored in a refrigerator at -70°C for testing. 2 ml of blood was collected from the tail vein at 1, 2 and 4 weeks, and divided into three tubes each time. Each tube was centrifuged at 3000 rpm for 10 minutes at room temperature, and 1.0 ml of serum was taken and placed in a refrigerator at -80°C for testing.
Determination the level of Blood Urea Nitrogen (BUN) and creatinine (Cr)
The levels of BUN and Cr in blood samples, and urea nitrogen and creatinine in feces samples were determined by Hitachi 7170A automatic biochemical analyzer.
RT-PCR detection for the expression level of Claudin-1, Occludin and ZO-1
The small intestine was taken and total RNA was extracted according to the Trizol reagent instructions. Reverse transcription was performed with standard steps, and the obtained cDNA was subjected to real-time quantitative PCR experiments. The total PCR reaction system was 25 μl, which included 9.5 ul of double distilled water, 2 ul of cDNA, 12.5 ul of SYBR Green dye, and 0.5 ul of upstream and downstream primers. Primer sequences are shown as follows: claudin-1, (upstream) 5’ATGGCAATAGAATCGTT3’, (downstream) 5’-TTGGTGTTGGGTAAGAG-3’; Occludin, (upstream) 5’-AATAAAGAACTCTCCCG-3’, (downstream) 5’-CATAGTCTCCAACCATC-3’; ZO-1, (upstream) 5’- TGGTGTCCTACCTAATTCAACTCA-3’, (downstream) 5’-CGCCAGCTACAAATATTCCAACA-3’; β-actin, (upstream) 5’-ACTCTTCCAGCCTTCCTTCC-3’, (downstream) 5’-GAGGAGCAATGATCTTGATCTTC-3’.
Western blot for protein levels of Claudin-1, Occludin and ZO-1
The small intestine was taken, total protein was extracted by RIPA lysis and protein concentration was determined using the BCA protein assay kit. 20 μg denatured protein were added to each well, and electrophoresed using 20% SDS-PAGE gel. The protein was transferred to PVDF membrane under constant pressure, and 3% bovine serum albumin was used to block for 2 h. Primary antibodies (claudin-1, ccludin, ZO-1, β-actin) were separately added and incubated at 37°C for 2 h or 4°C overnight. The membrane was washed 3 times with PBST, and the corresponding HRP-labeled IgG was added and incubated for 1 hour. The membrane was washed 3 times with PBST, developed with ECL solution, exposed and imaged, and the results were analyzed. β-actin was used as internal reference.
Immunohistochemistry assay
The intestine samples were taken to make paraffin specimens. Paraffin sections were dewaxed by xylene, hydrated by gradient alcohol, and incubated at 3% H2O2 for 5-10 minutes to eliminate endogenous peroxidase activity. Then, the antigen was heat-immobilized by immersing in 0.01 M citrate buffer (pH 6.0). After cooled, normal goat serum was added and incubated at room temperature for 20 minutes. Immunohistochemical reaction was processed with avidin-biotin-peroxidase complex method, Claudin-1, ccludin, ZO-1 antibody were added. The corresponding biotin-labeled secondary antibody IgG was added and incubated at 37°C for 30 min. Finally, the color was developed by glucose oxidase diaminobenzidine (DAB) nickel sulfate amine method, and the degree of color development was grasped under the microscope. Hematoxylin is mildly counterstained and rinsed with running water. It was sequentially dehydrated with 75%-80%-95%-100% alcohol, transparented by xylene, sealed by neutral gum, and observed by light microscopy. Ten visual fields were randomly observed in each group. The image density of positive target and the percentage of positive area in each field of view were analyzed by Image-Pro P1uS Version 6.0 image analysis system, and the average optical density (IOD/area) was used to represent the expression level.
Hematoxylin-Eosin (HE) staining assay
3 μm thick paraffin section was routinely dewaxed and hydrated by ethanol with various concentrations. Nucleus was stained by Hematoxylin for 7 minutes at room temperature, washed with tap water for 30-60 seconds, and differentiated by 1% hydrochloric acid alcohol. After rinsed for 1 minute, the sample was stained by eosin for 2 minutes at room temperature. Then, the sample was dehydrated by gradient alcohol, transparent by xylene for 1 minute, and sealed by the neutral gum. The nuclear was stained in blue and cytoplasm was stained in red.
Periodic Acid-Silver Metheramine (PASM) staining assay
3 μm thick paraffin section was routinely dewaxed and hydrated by ethanol with various concentrations. Then, the sample was processed as following steps: oxidated by 0.5% periodate for 30 minutes, oxidized by 10% chromic acid for 20 min, treated by 0.5% partial sodium sulfite for 30 s, and put into the hexamine silver solution for 20-30 min. After washed by distilled water, microscopic examination was processed. Then, the sample was toned by 0.1% gold chloride aqueous solution for 30 seconds, dyed by hematoxylin for 3 minutes, dyed by 0.5% eosin was dyed for 3 minutes, and processed for conventional dehydration and transparent sealing.
Masson staining assay
3 μm thick paraffin section was routinely dewaxed and hydrated by ethanol in various concentrations. The sample was dyed by hematoxylin, Xylidine Ponceau 2R, 1% phosphomolybdic acid and 2% aniline blue in turn. The section was washed by water, dehydrated by gradient alcohol, transparented by xylene for 1 minute, and sealed with neutral gum. As a result, the collagen fibers were stained as blue.
Statistical Analysis
SPSS 11.0 software was used for statistical analysis. Values were expressed as mean ± standard deviation. Variance analysis was processed to determine the difference between two groups. P< 0.05 was considered statistically significant.
Results
The level of blood urea nitrogen and creatinine
As shown in Figure 2, compared with the sham operation group, the serum levels of BUN and Cr in the two operation group were significantly increased, indicating that the modeling was successful. Compared with the operation + non- Chinese medicine intervention group, the serum levels of BUN and Cr in the operation + Chinese medicine intervention group did not change, indicating that the model of chronic renal failure was successfully established, but the drug did not play a significant role in the model. At the same time, it could be seen that with the increase of time, the urea nitrogen level in the serum gradually decreased, while there was no obvious rule of creatinine change.
The expression level of Claudin-1, Occludin and ZO-1
Compared with the sham operation group, the expression of tight junction-associated genes (Claudin-1, Occludin and ZO-1) in the ascending colon of the surgical group model animals was significantly reduced. However, the expression of tight junction-associated genes in the ascending colon of the operation + Chinese medicine intervention group was increased, but the different was not significant (Figure 3). It also indicated that the chronic renal failure model was successfully established. However, the drug did not play a significant role in the intestinal intervention model, and there was no significant difference in the three genes among the four groups.
The protein level of Claudin-1, Occludin and ZO-1
The protein level of Claudin-1, Occludin and ZO-1 was similarly with the results of RT-PCR. As shown in figure 4, compared with the sham operation group, the expression of tight junction-associated proteins (Claudin-1 and Occludin) in operation group was significantly decreased. Compared with the operation group, the expression of Occludin in the ascending colon was significant elevated in the operation + Chinese medicine intervention group. The other two proteins were elevated but without significant difference.
Immunohistochemistry assay
The immunohistochemistry assay was similarly with the results of RT-PCR and western blot (Figure 5). Compared with the sham operation group, the expression of tight junction-associated proteins (Claudin-1 and Occludin) in operation group was significantly decreased. After Traditional medicine intervention, the expression of Claudin-1 and Occludin in the ascending colon was significant elevated. However, The ZO-1 proteins were elevated but without significant difference.
HE staining assay
In two sham operation groups, the glomerular structure was normal, while some tubular epithelial epithelium was mildly edematous and vacuolar degeneration. Part of the renal interstitial was scattered in a small amount of chronic inflammatory cells. However, in operation group, more glomerular volume was reduced, and some glomerular structures were destroyed and disappeared. Partially proximal tubules were with severe vacuolar degeneration and epithelial atrophy, and brush-like edges were disappeared. Unstructured protein tube type and more red blood cells were found in partial lumen. Renal interstitial granules were infiltrated in more chronic inflammatory cells with fibrous tissue hyperplasia. After Traditional medicine intervention was processed, the lesion has a certain degree of improvement (Figure 6).
PASM staining assay
As shown in Figure 7, there were no clear abnormalities in the glomerular capsule basement membrane, capillary basal membrane, renal tubular epithelial basement membrane and mesangium in two sham- operation groups. However, after operation, partial glomerular basement membrane was uneven thickening companying with mesangial proliferation. In addition, the number of cells in some glomeruli decreased, the local renal capillary basal membrane was broken, and the tubular structure was disordered. Traditional medicine intervention restored the above damage, but the difference was not significant compared with surgery group.
Masson staining assay
Microscopic examination results displayed that a small proportion of renal interstitial fibrous tissue was slightly hyperplasia in two sham-operation group. However, a large number of fibrous tissue hyperplasia were observed in some renal interstitial companying with some glomeruli and renal tubules atrophy and disappear in operation + Chinese medicine intervention group and operation+ non- Chinese medicine intervention group (Figure 8).
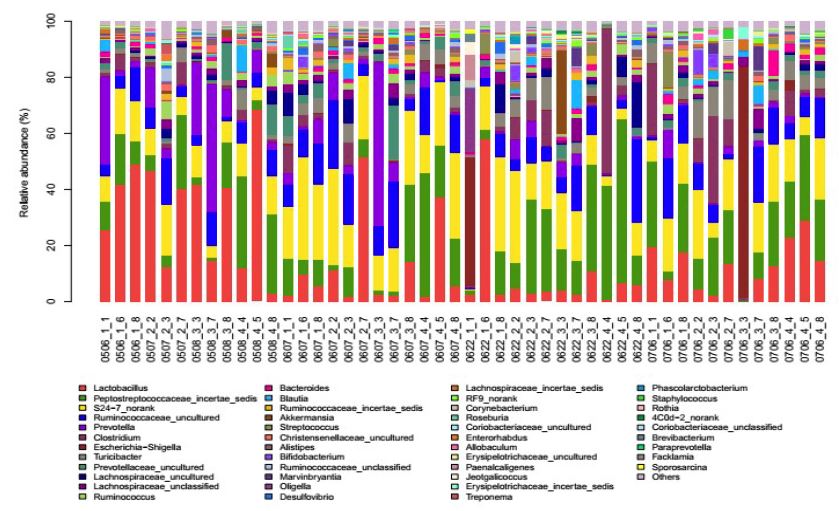
Figure 1: The distribution of thick-walled bacteria, Bacteroidetes, Proteobacteria, and actinomycetes in intestinal flora.
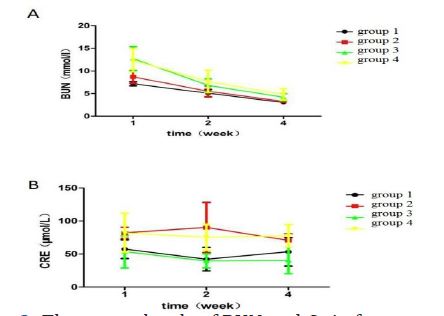
Figure 2: The serum levels of BUN and Cr in four groups.
Note: A. The serum levels of BUN, B. The serum levels of Cr
Sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4).

Figure 3: The expression level of Claudin-1, Occludin and ZO-1.
Note: The expression of Claudin-1, Occludin and ZO-1 in ascending and descending colon were determined by RT-PCR. sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4). *compared with group 1, p< 0.05, # compared with group 2, p< 0.05.
Note: The expression of Claudin-1, Occludin and ZO-1 in ascending and descending colon were determined by RT-PCR. sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4). *compared with group 1, p< 0.05, # compared with group 2, p< 0.05.

Figure 4: The protein level of Claudin-1, Occludin and ZO-1.
Note: The protein of Claudin-1, Occludin and ZO-1 in ascending and descending colon were determined by western blot. sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4). *compared with group 1, p< 0.05, # compared with group 2, p< 0.05, & compared with group 3, p< 0.05.
Note: The protein of Claudin-1, Occludin and ZO-1 in ascending and descending colon were determined by western blot. sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4). *compared with group 1, p< 0.05, # compared with group 2, p< 0.05, & compared with group 3, p< 0.05.

Figure 5: The immunohistochemistry assay level of Claudin-1, Occludin and ZO-1 (×400).
A. Ascending colon. B. Descending colon
Sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4).
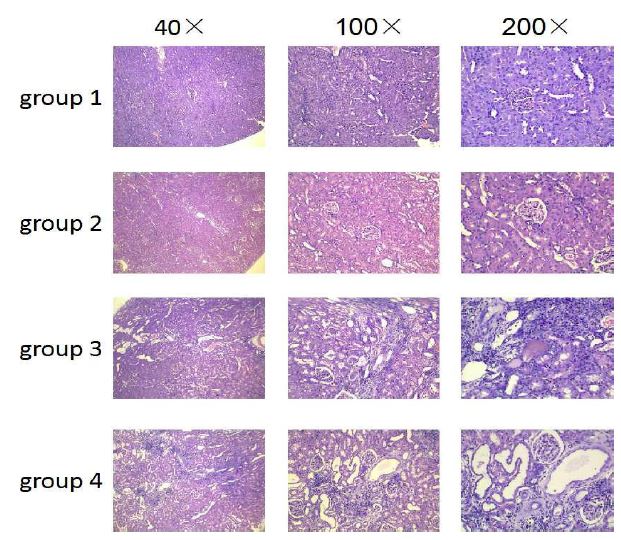
Figure 6: HE staining assay for kidney sample.
Note: sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4).
Note: sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4).
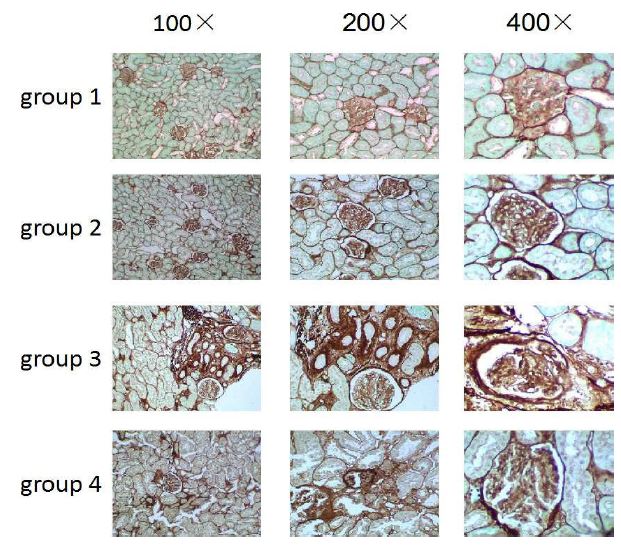
Figure 7: PASM staining assay for kidney sample.
Note: sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4).
Note: sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4).

Figure 8: Masson staining assay for kidney sample.
Note: sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4).
Note: sham operation+ non- Chinese medicine intervention group (group 1), sham operation+ Chinese medicine intervention group (group 2), operation+ non- Chinese medicine intervention group (group 3) and operation+ Chinese medicine intervention group (group 4).
Discussion
Chronic kidney disease is one of the public health concerns of the world [13]. About 5% of patients with chronic kidney disease will eventually enter CRF), but there is no effective intervention in the progression of chronic kidney disease. Contemporary Traditional medicine has applied various traditional Chinese medicines to delay the progression of CRF via intestinal treatment [14]. Previous studies have shown that except to reduce the levels of toxins such as urea, creatinine and molecular substances in patients with CRF, the progress of this disease was still delayed [15]. However, the mechanism and therapeutic targets were not clear. In this study, CRF rat model was treated by Traditional medicine through the intestine. In addition, Realtime PCR, Western blot, laser scanning and renal pathology were processed to determine the expressions of tight junction-associated genes and histomorphological changes. Interestingly, Traditional medicine intervention via intestine was found to increase the expression of Claudin-1 and Occludin, and also restored the histomorphological changes. However, the BUN and Cr levels were with significantly difference.
The main components of the prescription in this study were rhubarb and dandelion. Rhubarb had anti-inflammatory, anti-proliferative effects, which could also reduce the toxins in uremic patients [16]. Other studies have confirmed that rhubarb could improve the degree of glomerular sclerosis in chronic renal failure models [17]. Besides, dandelion was a traditional Chinese medicine widely used in intestinal diseases [18]. It had the effect of promoting intestinal smooth muscle peristalsis and accelerating intestinal emptying [19]. At the same time, dandelion also had the effect of reducing the expression of pro-inflammatory factors [20]. Moreover, oral activated carbon could significantly alleviate the bismuth sulfate and p-cresol sulfate in plasma, and these uremic toxins were produced by intestinal bacteria [21]. More importantly, Traditional medicine was always tolerated by intestinal treatment [22]. Thereby, the above information provided a sufficient theoretical basis for this study.
As a barrier, the intestine had the function of resisting microorganisms, bacterial toxins, digestive enzymes, food degradation products, antigens and other harmful substances from the intestinal lumen into the blood circulation [23]. In a patient with CRF, destruction of the intestinal epithelial barrier structure and function might lead to local and systemic inflammation of the intestine, and increase permeability of the intestinal mucosa, thereby causing the above harmful substances to enter the internal environment [24]. Tight junctions were composed of transmembrane proteins, cellular matrix proteins, and pre-binding proteins [25]. Among them, the transmembrane protein family included the occludin and claudin families, which connected the plasma membranes of adjacent cells and formed a barrier against the dispersion of liquids and solutes [26]. Cellular matrix proteins regulated the permeability of cell bypass by altering the structure and function of tight junction [27]. The tight junction formed an effective barrier that prevents bacteria, bacterial toxins, antigens, digestive enzymes, food degradation products and other toxic substances from entering the bloodstream from the intestinal lumen [28]. Similarly results were also observed in this study, Traditional medicine intervention via intestine increased the expression of Claudin-1 and Occludin, and also restored the histomorphological changes. Normally.
The gut was also the main channel for absorbing nutrients and removing waste [29]. Normally, 75% of the metabolite urea nitrogen should be excreted from the kidneys and 25% into the colon [30]. However, in CRF patients, the intestinal tract became an important way to remove toxins [31]. A large amount of urea nitrogen was secreted into the intestine, which might cause the proliferation of bacteria in the colon [32]. The urease in bacteria broke it into carbon dioxide and excess ammonia, and provided more raw materials for the synthesis of urea [33]. As a result, the increased nitrogenous compounds in the gut provided adequate nutrition for the growth and reproduction of various intestinal bacteria. However, the BUN and Cr levels were not decreased after Traditional medicine intervention in this study [34]. This will be one of the important indicators for us to improve our prescriptions in the future.
In conclusion, Traditional medicine intervention could increase the expression of Claudin-1 and Occludin, and also restored the histomorphological changes of CKD. Though the efficacy needed to be further improved, the study provided new ideas for delaying CRF.
Highlights
1. Traditional medicine intervention could increase the expression of Claudin-1 and Occludin.
2. Traditional medicine intervention restored the histomorphological changes of CKD.
3. BUN and Cr levels were not decreased after Traditional medicine intervention.
References
- Weiner DE. Public health consequences of chronic kidney disease. Clinical Pharmacology & Therapeutics. 2009; 86: 566.
- Kearns B, Gallagher H, Lusignan SD. Predicting the prevalence of chronic kidney disease in the English population: a cross-sectional study. BMC Nephrology. 2013; 14: 49-49.
- Nissenson AR, Pereira BJ, Collins AJ, Steinberg EP. Prevalence and characteristics of individuals with chronic kidney disease in a large health maintenance organization. American Journal of Kidney Diseases. 2001; 37: 1177-1183.
- Chantrel F, Enache I, Bouiller M, Kolb I, Kunz K, et al. Abysmal prognosis of patients with type 2 diabetes entering dialysis. Nephrology, dialysis. 1999; 14: 129.
- Purnell TS, Auguste P, Crews DC, Lamprea-Montealegre J, Olufade T, et al. Comparison of life participation activities among adults treated by hemodialysis, peritoneal dialysis, and kidney transplantation: a systematic review. American Journal of Kidney Diseases the Official Journal of the National Kidney Foundation. 2013; 62: 953-973.
- Wu AW, Fink NE, Marsh-Manzi JVR, Meyer KB, Finkelstein FO, et al. Changes in Quality of Life during Hemodialysis and Peritoneal Dialysis Treatment: Generic and Disease Specific Measures. Journal of the American Society of Nephrology. 2004; 15: 743-753.
- Karkar A. Caring for Patients with CRF: Rewards and Benefits. Int J Nephrol. 2011; 2011: 639840-639840.
- Huang HJ, Chen YC. A possible solution for hair loss by inhibiting corticotropin-releasing factor (CRF) receptor from traditional Chinese medicine. Journal of Biomolecular Structure & Dynamics. 2014; 32: 1613-1623.
- Tzamaloukas AH, Murata GH, Piraino B, Malhotra D, Bernardini J, et al. The relation between body size and normalized small solute clearances in continuous ambulatory peritoneal dialysis. Journal of the American Society of Nephrology Jasn. 1999; 10: 1575-1581.
- Tost H, A. Nizet. Reduction of the glomerular filtration rate by the efferent blood from a kidney taken from a previously dehydrated dog. Pflügers Archiv European Journal of Physiology. 1973; 345: 327.
- Lambert G, Amar MJA, Guo G, Brewer HB, Gonzalez FJ, et al., The Farnesoid X-receptor Is an Essential Regulator of Cholesterol Homeostasis. Journal of Biological Chemistry. 2003; 278: 2563-2570.
- Vitetta L, G. Gobe. Uremia and chronic kidney disease: The role of the gut microflora and therapies with pro‐ and prebiotics. Molecular Nutrition & Food Research. 2013; 57: 824-832.
- Saran R, Hedgeman E, Huseini M, Stack A, Shahinian V. Surveillance of chronic kidney disease around the world: tracking and reining in a global problem. Advances in Chronic Kidney Disease. 2010; 17: 271-281.
- Wang L, Wang MZ. A survey on experimental studies on traditional Chinese medicine treatment of chronic renal failure. Chinese Journal of Integrated Traditional & Western Medicine. 1996; 2: 232-235.
- Lekawanvijit S, Kompa AR, Wang BH, Kelly DJ, Krum H, et al. Cardiorenal syndrome: the emerging role of protein-bound uremic toxins. Circulation Research. 2012; 111: 1470-1483.
- Wang Q, Zhang NN, Li HY, Jiang M, Gao J, et al. Active ingredients in rhubarb with anti-proliferative effects on scar fibroblasts]. Acta Pharmaceutica Sinica. 2012; 47: 1618.
- Khan IA, Nasiruddin M, Haque SF, Khan RA, et al. Evaluation of Rhubarb Supplementation in Stages 3 and 4 of Chronic Kidney Disease: A Randomized Clinical Trial. International Journal of Chronic Diseases. 2014; 2014: 1-6.
- Lin L. Mechanism of Traditional Chinese Medicine on Intestinal Mucosal Immunity in Chronic Intestinal Diseases. 2017; 3: 20-23.
- Ling WF, Ming C, Qiang YG. The Purgative Effect and Pharmacokinetics Rhubarb’s Combined Anthraquinone. Chinese Journal of Experimental Traditional Medical Formulae. 1999.
- Davaatseren, M. Dandelion leaf extract protects against liver injury induced by methionine- and choline-deficient diet in mice. Journal of Medicinal Food. 2013; 16: 26.
- Savira F, Cao L, Wang I, Yang W, Huang K, et al. Apoptosis signal-regulating kinase 1 inhibition attenuates cardiac hypertrophy and cardiorenal fibrosis induced by uremic toxins: Implications for cardiorenal syndrome. Plos One. 2017; 12: e0187459.
- Sgadari C. Pharmacological management of Kaposi’s sarcoma. Expert Opinion on Pharmacotherapy. 2011; 12: 1669-1690.
- Bjarnason I. The Pathogenesis and Consequence of Non Steroidal Anti-Inflammatory Drug Induced Small Intestinal Inflammation in Man. Acta Rheumatologica Scandinavica. 1987; 16: 55-62.
- Overman EL. Intestinal CRF Receptor Subtypes Mediate Divergent Roles in Stress-Induced Intestinal Epithelial Barrier Dysfunction. Dissertations & Theses – Gradworks. 2011.
- Harhaj NS, Antonetti DA. Regulation of tight junctions and loss of barrier function in pathophysiology. International Journal of Biochemistry & Cell Biology, 2004; 36: 1206-1237.
- Akimoto T. Analysis of the expression and localization of tight junction transmembrane proteins, claudin-1, -4, -7, occludin and JAM-A, in human cervical adenocarcinoma. Histology & Histopathology. 2016; 31: 11729.
- Li CX, Poznansky MJ. Effect of FCCP on tight junction permeability and cellular distribution of ZO-1 protein in epithelial (MDCK) cells. Biochim Biophys Acta. 1990; 1030: 297-300.
- Singh AK, Jiang Y, Gupta S. Effects of bacterial toxins on endothelial tight junction in vitro: a mechanism-based investigation. Toxicology Methods. 2008; 17: 331-347.
- Troyer K. Diet selection and digestion in Iguana iguana: the importance of age and nutrient requirements. Oecologia. 1984; 61: 201-207.
- Jonker JS, Kohn RA, Erdman RA. Using milk urea nitrogen to predict nitrogen excretion and utilization efficiency in lactating dairy cows. Journal of Dairy Science. 1998; 81: 2681-2692.
- Taché Y. Brain and gut CRF signaling: biological actions and role in the gastrointestinal tract. Current Molecular Pharmacology. 2018; 10.
- Dai ZL, Wu G, Zhu WY. Amino acid metabolism in intestinal bacteria: links between gut ecology and host health. Frontiers in Bioscience. 2011; 16: 1768.
- Varel VH, Wells JE, Miller DN. Combination of a urease inhibitor and a plant essential oil to control coliform bacteria, odour production and ammonia loss from cattle waste. Journal of Applied Microbiology. 2010; 102: 472-477.
- MichihikoYatazawa, NorioKurihara, Katsuhisa Furuhashi. Availability of several kinds of nitrogenous compounds for the growth of callus tissues from Daucus Carota L., Datura Stramonium L., Pelargonium Inquinans Ait., and Oryza Sativa L. Soil Science & Plant Nutrition. 2012; 14: 147-152.
