
Open Access, Volume 9
Macroscopic and microscopic features in a fatal case of hypertrophic obstructive cardiomyopathy after myectomy
Tambuzzi Stefano; Gentile Guendalina*; Boracchi Michele; Sollennità Luca; Zoja Riccardo
Laboratorio di Istopatologia Forense e Microbiologia Medico Legale - Sezione di Medicina Legale e delle Assicurazioni - Dipartimento di Scienze Biomediche per la Salute - Università degli Studi di Milano, Via Luigi Mangiagalli, 37 - 20133 Milano, Italy.
Guendalina Gentile
Section of Forensic Medicine, Department of Biomedical Sciences for Health, University, via Luigi Mangiagalli, 37- 20133 Milan, Italy.
Tel: +39-0250315720; Email: guendalina.gentile@unimi.it
Received : April 06, 2023,
Accepted : May 12, 2023
Published : May 16, 2023,
Archived : www.jclinmedcasereports.com
Keywords: Cardiomyopathy; Hypertrophic; Cardiac surgical procedures; Autopsy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gentile G (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Stefano T, Guendalina G, Michele B, Luca S, Riccardo Z. Macroscopic and microscopic features in a fatal case of hypertrophic obstructive cardiomyopathy after myectomy. Open J Clin Med Case Rep. 2023; 2038.
Introduction
Hypertrophic Obstructive Cardiomyopathy (HOCM) is an autosomal dominant genetic disorder that results in interstitial fibrosis and ventricular hypertrophy. There is severe and asymmetric enlargement of the wall of the left ventricle and especially the septum, which may be localized or diffuse [1]. This is associated with Left Ventricular Outflow Tract Obstruction (LVOT), with a resting gradient greater than 30 mmHg [2]. Ventricular arrhythmia and heart failure are the main threats and may also be the first clinical presentation of the disease [3]. Once diagnosed, HOCM can be treated with various strategies: pharmacological, septal dissection, implantation of a cardioverter defibrillator, or transplantation in case of end-stage heart disease [4]. Septal Myectomy (SM) according to Morrow, which can also be performed by thermal ablation, is now considered the therapeutic gold standard. In this procedure, the cardiac septum is partially removed at the level of the papillary muscle bases to reduce the obstruction of the ventricular outflow [5]. In this report, we present the interesting macroscopic and microscopic findings of a case of HOCM with fatal outcome after myectomy surgery.
Case History
A 22-year-old girl who was symptomatic for recurrent syncope was diagnosed with HOCM, with increased mean ventricular gradient (48 mmHg), diastolic dysfunction, and mitral regurgitation (NYHA functional class III). Genetic testing revealed mutations in genes encoding the beta-myosin heavy chain (7-MYH7) and myosin C3 binding protein (MYBPC3). The patient underwent SM according to Morrow by thermal ablation, which removed 3.7 g of the anterior and posterior septum, and mitral valve repair. However, the surgery was complicated by sudden left ventricular dysfunction with severe mitral regurgitation, which required pharmacological support and the use of an aortic counter pulsation. Left ventricular ejection fraction was 30%, and pulmonary hypertension and multiorgan failure occurred. Two days after surgery, bradycardia led to cardiac arrest, which did not respond to resuscitative efforts and resulted in the patient’s death.
Autopsy findings
At autopsy, the heart (450 g; longitudinal diameter = 12 cm, transverse diameter = 9 cm and anteroposterior diameter = 7 cm) was hypertrophic with the following thicknesses of the left ventricle (Figure 1A, Table 1).
Table 1: Thicknesses of the upper, medium, and lower third of the left ventricle (front wall, septum and back wall).
| Front wall | Septum | Back wall | |
|---|---|---|---|
| Proximal third | cm 1.4 | cm 1 | cm 1.6 |
| Medium third | cm 2.1 | cm 1.6 | cm 1.5 |
| Distal third | cm 1.4 | cm 1.6 | cm 1.8 |
| Cardiac apex | cm 1.3 | cm 1.6 | cm 2.1 |
The myocardium appeared woody in consistency and showed an overall marked reduction in the size of the left ventricular lumen, which was even more pronounced in the mid-apex region. The septal endocardium appeared brownish, which was due to heat damage during surgical thermal ablation (Figure 1B).
Histological examination
Histological analyses was performed on extensive cardiac sampling (mapping), on three levels (proximal, medium, and distal thirds), taking samples from both the anterior and posterior portions of the septum. Overall, there was large areas of myocardial fibers disarray, associated with a marked increase in interstitial connective tissue and significant fibrous proliferation, with hypertrophic myocardial cells and muscle bundles of irregular shape, size, and orientation (Figure 2). There were also structural heat changes with foci of charred muscle tissue associated with deposits of blackish granular pigment and diffuse areas of loss of dyeing affinity (Figure 3). Details by specific cardiac site are given in Table 2.
Table 2: Distribution pattern of pathologic and thermal changes at different levels of the interventricular septum.
| Septum | Fibrotic replacement | Heat changes | |
|---|---|---|---|
| Proximal third | Front wall | 30% | moderate |
| Back wall | 20% | ||
| Medium third | Front wall | 30-40% | moderate |
| Back wall | |||
| Distal third | Front wall | 70% | severe |
| Back wall | 60% | ||
Microscopic findings of the remaining viscera indicated widespread ischemic disorder. The cause of death was therefore identified as multiple organ failure in a HOCM carrier, with left ventricular failure secondary to SM.
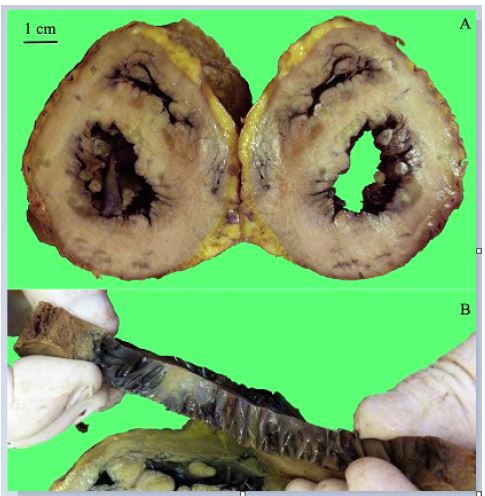
Figure 1: In A, macroscopic view of the two coronal sections of the heart in the medium third with marked ventricular and septal hypertrophy (upper left, metric reference); in B, heart strip with diffuse brownish myocardium and ligneous consistency.
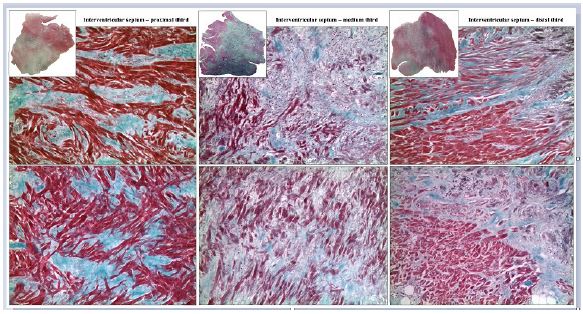
Figure 2: Microscopic views of interventricular septal sections at three levels: proximal, medium, and distal. The upper row shows sections from the anterior part of the septum with relative overviews (3X), and the lower row shows sections from the posterior part. All are stained with Masson’s trichrome technique according to Goldner (100X) and show marked fibrotic replacement of myocardial tissue.
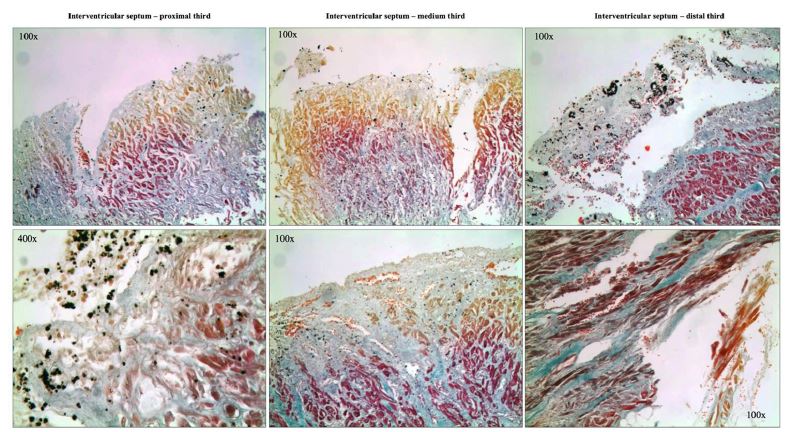
Figure 3: Microscopic views of interventricular septal sections at three levels: proximal, medium, and distal. All are stained with Masson’s trichrome technique according to Goldner (100X-400X) and show the presence of charred tissue and widespread loss of dyeing affinity, consistent with heat damage induced by thermal ablation.
Discussion
SM surgery is associated with an early surgical mortality rate of 5% to 10% and a high incidence of significant complications such as heart block, valve regurgitation, and ventricular septal defect [6]. Thus, overall, it is not a completely risk-free procedure, with patient death as a complication statistically possible [7]. Moreover, HOCM is the main cause of sudden cardiac death in young people, especially in those under 25 years of age [8], so a comprehensive understanding of the anatomical-pathological features of this pathology is necessary. And it is precisely from this point of view that we found it interesting to report on the macroscopic and histological findings of the autopsy case presented, pursuing a two fold aim. First, we wanted to present a thorough picture of the pathology after comprehensive cardiac mapping, showing how infiltrative and widespread fibrotic replacement of the cardiac septum can be in severe HOCM. At the same time, this was the first time in the literature that the direct effects of thermal septal ablation on the myocardium have been demonstrated and described. These findings usually go completely unnoticed because patients survive or, if they die, a complete autopsy is not performed. However, because any surgical procedure results in anatomic-pathologic changes in the affected tissue, it is important for both clinicians and forensic pathologists to know the final cardiac outcomes after septal myectomy with thermal ablation.
Declarations
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicts of interest/competing interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval: This article does not contain any studies with (living) human participants or animals performed by any of the Authors. The subjects involved in this study underwent a judicial autopsy at the Institute of Legal Medicine of Milan in order to identify the cause of death. Data collecting, sampling and subsequent forensic analysis were authorized by the public prosecutor. Therefore data were acquired as part of a forensic judicial investigation and in accordance to Italian Police Mortuary Regulation.
Consent to participate: The authors declared that all the investigations were carried out accordingly to the Italian Law.
Consent for publication: All the authors agree for publication
Availability of data and material: All the data have been reported in the manuscript.
Code availability (software application or custom code) : Not applicable.
Authors' contributions: TS and GG equally contributed to this work. They devised the project and the main conceptual idea of the article, collected data, drafted the manuscript and performed literature research. BM and SL contributed to the samples collection, investigation and methodology, analyses interpretation, literature research and editing. RZ guarantor of the project and directed the study, devised the main conceptual idea of the article.
References
- Maron BJ, Mackey-Bojack S, Easy E, Duncanson E, Rowin EJ, et al. Hypertrophic cardiomyopathy and sudden death initially identified at autopsy. Am J Cardiol. 2020; 127: 139-141.
- Ferrazzi P, Spirito P, Iacovoni A, Calabrese A, Migliorati K, Simon C, et al. Transaortic chordal cutting: mitral valve repair for obstructive hypertrophic cardiomyopathy with mild septal hypertrophy. J Am Coll Cardiol. 2015; 66: 1687-1689.
- Veselka J, Anavekar NS, Charron P. Hypertrophic obstructive cardiomyopathy. Lancet. 2017; 389: 1253-1267.
- Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, et al. 2011 ACCF/AHA Guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Developed in collaboration with the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2011; 58: E212-60.
- Morrow AG, Brockenbrough EC. Surgical treatment of idiopathic hypertrophic subaortic stenosis: technic and hemodynamic results of subaortic ventriculomyotomy. Ann Surg. 1961; 154: 181-89.
- Ghavidel AA, Alizadehasl A, Khalilipur E, Amirghofran A, Nezhadbahram H, Azarfarin R. Surgical septal myectomy for hypertrophic cardiomyopathy. The Iranian experience. Asian Cardiovasc Thorac Ann. 2022; 30: 64-73.
- Panaich SS, Badheka AO, Chothani A, Mehta K, Patel NJ, et al. Results of ventricular septal myectomy and hypertrophic cardiomyopathy (from nationwide inpatient sample [1998–2010]). Am J Cardiol. 2014; 114: 1390-1395.
- Maron BJ. Clinical course and management of hypertrophic cardiomyopathy. N Eng J Med. 2018; 379: 655-668.
