
Open Access, Volume 9
A pathological autopsy of a case dying from omicron variant of COVID-19
Somnath Das1*; Tushar Kanti Das2; Bhaswati Bandyopadhyay3; Rina Das4
1Department of Forensic Medicine and Toxicology, Bankura Sammilani Medical College, Bankura, India.
2Department of Pathology, R G Kar Medical College, Kolkata, West Bengal, India.
3Department of Microbiology, Virology Unit-In-charge, School of Tropical Medicine, Kolkata, India.
4Department of Forensic Medicine and Toxicology, R G Kar Medical College, Kolkata, India.
Somnath Das
Department of Forensic Medicine and Toxicology, Bankura Sammilani Medical College, Bankura, India.
Email: somnath1976@rediffmail.com
Received : March 21, 2023,
Accepted : May 01, 2023
Published : May 08, 2023,
Archived : www.jclinmedcasereports.com
Abstract
This is a case report on a male patient in his nineties who was admitted with a complaint of fever for three days and was positive for Covid-19. He had a previous history of diabetes with cardiac disease and right-sided hemiplegia. Upon the development of acute respiratory distress syndrome, the patient was put on a ventilator but finally died. The macroscopic findings showed congested and heavy lungs and dilated cardiac chambers with granular contracted kidneys. Histology from the lungs showed alveolar edema with desquamation of epithelial lining and formation of thrombi in the blood vessels. Both kidneys should have tubular necrosis on the proximal convoluted tubules. The genome sequencing showed the VOC- Omicron BA2 variance. Though Omicron BA2 variance was supposed to be less virulent, this case had shown all the features of typical Covid-19 pathological findings.
Keywords: Forensic pathology; Covid-19; Omicron BA2 variance.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Das S (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Das S, Das TK, Bandyopadhyay B, Das R. A pathological autopsy of a case dying from omicron variant of COVID-19. Open J Clin Med Case Rep. 2023; 2030.
Description
The Severe Acute Respiratory Syndrome (SARS)-Coronavirus-2 (CoV-2) outbreaks in Wuhan, China has resulted in a catastrophic pandemic [1]. With time the virus has undergone a number of variations affecting the transmission, diagnosis, and treatment. The latest of them is the omicron variant [2].
Clinical History
A fully vaccinated, male patient in his nineties was admitted with a complaint of fever for three days, and a positive COVID-19 RTPCR report with a background history of hypertension, type 2 diabetes mellitus, and post PTCA (percutaneous trans-luminal coronary angioplasty) status. He had a history of right-sided hemiplegia for which he received conservative medications. After admission, he was started with intrave nous fluids, antibiotics, nebulized steroids, and low molecular weight heparin with moist oxygen inhalation as per requirement. His preliminary investigations showed increased C- reactive protein and increased lactate dehydrogenase with hypoalbuminemia. His oxygen demand showed an increasing trend as he required NRBM (non-rebreather mask), followed by bi-level positive airway pressure, then non-invasive ventilation, and finally by invasive ventilator support. He was started with Remdesivir along with other medications. After two days he became disoriented and drowsy and finally expired following cardio-respiratory arrest. The cause of death was deemed to be due to ARDS (Acute respiratory distress syndrome) in a case of COVID-19 pneumonia with type 2 diabetes mellitus, and hypertension in post-PTCA status.
Autopsy
The chest cavity showed evidence of adhesion between the visceral and parietal pleura. The gross finding of the lungs showed that both the lungs were congested, heavy, and firm in consistency, especially towards the lower zone.
The heart was enlarged and firm. The four chambers were dilated and the walls showed few areas of congestion. The coronary arteries were found to be patent on sectioning except for the right coronary artery where there was a metallic coronary stent present inside the lumen. Both the kidneys showed granulation and contraction. The brain was oedematous and farm-to-soft in consistency. Some areas of congestion were noticed in both hemispheres.
Histology
Sections were taken from -
• Parts of both lungs show focal interstitial and alveolar edema, inflammation with desquamation of alveolar lining epithelium, and hyaline membrane formation. There is congestion and thrombi formation in the small to medium-sized vessels. The histomorphological features are in favor of Diffuse Alveolar Damage (DAD) (Figure 1).
• Sections from different areas of the heart including the left coronary artery show unremarkable histology. The right coronary artery and root of the aorta show the presence of atheromatous plaques.
• Sections from both kidneys show tubular necrosis of mainly proximal convoluted tubules. Glomeruli are uninvolved (Figure 2).
• Sections from the liver showed microvesicular steatosis and centrilobular congestion.
• Histomorphological features from sections from parts of the brain showed normal architecture. Meningeal vessels showed the presence of thrombi and congestion
Genome sequence
SARS CoV-2 positive RNA (Ct value of E gene-24, RdRp-27) from the referring laboratory was received at Virology Unit. About 50 μl RNA was aliquoted and transported in dry ice to the reference laboratory for whole genomic sequencing. Sequenced data was analyzed using Dragen RNA pathogen detection software (version 9) in Base Space (Illumina Inc, USA). VOC – Omicron BA.2 was reported to be found by whole genome sequencing (WGS) of the RNA sample.
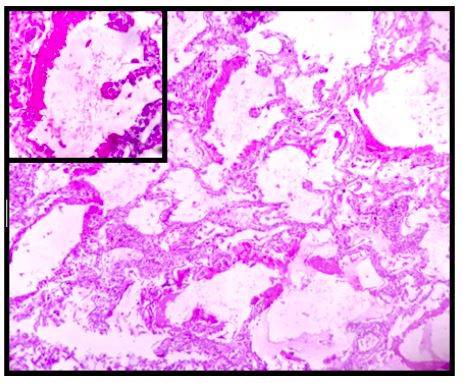
Figure 1: Photomicrograph of diffuse alveolar damage. (H&E stain, Mag 100x). Inset: Hyaline Membrane, (H&E stain, Mag 400x).

Figure 2: Photomicrograph of proximal tubular necrosis with normal-looking glomerulus and distal tubules. (H&E stain, Mag 400x).
Discussion
An insufficient number of Autopsy examinations for understanding the pathogenesis of covid-19 disease have been done throughout the world in the last two years. To date, the underlying mechanism of severe Covid-19 infection remains obscure [3].
Most of the deaths were due to severe lung involvement [4]. Diffuse Alveolar Damage (DAD) was a preliminary finding in this case along with the presence of thrombi in small and medium-sized vessels which are consistent with the findings of most the autopsy-based studies globally [4-8]. The presence of hyaline membrane and microvessel thrombosis which was a predominant finding, in this case, was suggestive of an early Acute Respiratory Distress Syndrome (ARDS) [9]. The virus is believed to infect the epithelial lining cells of the respiratory tract using the ACE2 enzyme as a viral receptor leading to DAD, edema, and a marked increase in lung weights at autopsy which was evident in this case [10]. On several sections of histology, the pulmonary parenchyma demonstrated a range of findings from patchy exudative hyaline membrane disease to organizing pneumonia.
The predominant histologic finding of the kidney was tubular necrosis, which was direct evidence of Acute Kidney Injury (AKI). AKI is common amongst hospitalized patients with COVID-19 infection, which alone contributes to a major proportion of deaths [11]. Our current knowledge regarding the proposed mechanism for kidney injury by the coronavirus is limited [12,13], but a chronic kidney disease in the background could have played a supplemental role as was evidenced in our case. Thus, the plausible role of SARS-CoV-2 as a direct injurious agent in kidney pathology or secondary to aggressive fluid management and immunologic effect is yet to be explored [13].
Among the sublineages of omicron, the most common ones are BA.1, BA.1.1 (or Nextstrain clade 21K) and BA.2 (or Nextstrain clade 21L). BA.2 differs from BA.1 in genetic sequences of some amino acids in the spike protein and other proteins. Studies have shown that BA.2 has a growth advantage over BA.1. Moreover, BA.2 appears inherently more transmissible than BA.1, which currently remains the most common Omicron sublineage reported as has happened in this case [14]. This difference in transmissibility appears to be much smaller than the difference between BA.1 and Delta [14].
Highlights
Omicron was the variant of concern (VOC) circulating globally.
Diffuse Alveolar damage (DAD) of the lungs and proximal tubular necrosis in the Kidney are the most common histopathological changes associated with deaths resulting from the Omicron variant with BA.2 sub linkage.
Covid-19 infection in the background of the pre-existing disease remains the most common cause of death among the elderly.
References
- Choudhary OP, Priyanka Mohammed TA, Singh I. Intranasal COVID-19 vaccines: is it a boon or bane? Int J Surg. 2021; 94: 106119.
- Gao SJ, Guo H, Luo G. Omicron variant (B.1.1.529) of SARS-CoV-2, a global urgent public health alert. J Med Virol. 2022; 94: 1255-1256.
- Layne SP, Walters KA, Kash JC, Taubenberger JK. More autopsy studies are needed to understand the pathogenesis of severe COVID-19. Nat Med. 2022; 28: 427-428.
- Wells AU, Devaraj A, Sujal R. Desai Interstitial Lung Disease after COVID-19 Infection: A Catalog of Uncertainties. Radiology. 2020; 299: E216-E218.
- Samsonova MV, Mikhaleva LM, Chernyaev AL. Pathology of COVID-19: Atlas. Moscow: Research Institute for Healthcare Organization and Medical Management, Moscow Healthcare Department; 2020. Brief Statistics (2000 autopsies of COVID-19 cases in Moscow).
- Barton LM, Duval EJ, Stroberg E, Ghosh S, Mukhopadhyay S. COVID-19 Autopsies, Oklahoma, USA. Am J Clin Pathol. 2020; 153: 725‐733.
- Menter T, Haslbauer JD, Nienhold R, Savic S, Hopfer H, et al. Post-mortem examination of COVID19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings of lungs and other organs suggesting vascular dysfunction. Histopathology. 2020; 77: 198-209.
- Hanley B, Lucas SB, Youd E, Swift B, Osborn M. Autopsy in suspected COVID-19 cases. J Clin Pathol. 2020; 73: 239‐242.
- Zhang Y, Gao Y, Qiao L, Wang W, Chen D. Inflammatory Response Cells During Acute Respiratory Distress Syndrome in Patients With Coronavirus Disease 2019 (COVID-19). Ann Intern Med. 2020; 173: 402.
- Elsoukkarya SS, Mostykaa M, Dillarda A, Bermana DR, Maa LX, et al. Autopsy Findings in 32 Patients with COVID-19: A Single-Institution Experience, Pathobiology. 2021; 88: 56-68.
- Santoriello D, Khairallah P, Bomback AS, Xu K, Kudose S, et al. Postmortem Kidney Pathology Findings in Patients with COVID-19. Journal of the American Society of Nephrology: JASN. 2020; 31: 2158-2167.
- Maiese A, Manetti AC, La Russa R, Di Paolo M, Turillazzi E, et al. Autopsy findings in COVID-19-related deaths: a literature review. Forensic science, medicine, and pathology. 2021; 17: 279-296.
- Parmar MS. Acute kidney injury associated with COVID-19-Cumulative evidence and rationale supporting against direct kidney injury (infection). Nephrology. 2021; 26: 239-247.
- Statement on Omicron sublineage BA.2. Who.int.
