
Open Access, Volume 9
A tale of multiple primaries: Primary neuroendocrine carcinoma, vaginal vault and renal cell carcinoma in a 52 years old female
More Shilpi; Yadav Alka; Raychaudhuri Sujata; Pujani Mukta; Chatterjee Tathagata*
Department of Pathology, ESIC Medical College and Hospital, NH3, NIT–3, Faridabad, Haryana, India.
Chatterjee Tathagata
Department of Pathology, ESIC Medical College and Hospital, NH3, NIT–3, Faridabad, Haryana, India.
Tel: 8551910936;
Email: ctathagat@gmail.com
Received : March 20, 2023,
Accepted : April 26, 2023
Published : April 27, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Cancer patients have 15-25% higher risk of second malignancy compared to general population. We hereby describe an extremely unusual case of 52-years-old-female with Neuroendocrine Carcinoma (NEC) of vaginal vault developing 4 years after undergoing nephrectomy for Renal Cell Carcinoma (RCC). Patient presented with bleeding per vaginum and vaginal vault mass. Clinical diagnosis was metastatic RCC. Papanicolauo smears were suggestive of small round cell tumour and not a metastatic RCC. Vaginal vault biopsy revealed tumour cells arranged in sheets and nests which were positive for synaptophysin on immunohistochemistry. CK and CD10 were negative rendering the final diagnosis as NEC, vaginal vault. NEC, vaginal vault is rare, more so in the present setting. The etiology of multiple primary carcinomas is perplexing and multifactorial. Complete evaluation of the patient presentation and clinical follow-up may provide important insight into the etiopathogenesis of multiple primaries and help in elucidating new horizons for diagnosis and management of such patients.
Keywords: Second primary carcinoma; Dual malignancy; Renal cell carcinoma (RCC); Neuroendocrine carcinoma (NEC); Vaginal vault.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Tathagata C (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Shilpi M, Alka Y, Sujata R, Mukta P, Tathagata C. A tale of multiple primaries: Primary neuroendocrine carcinoma, vaginal vault and renal cell carcinoma in a 52 years old female. Open J Clin Med Case Rep. 2023; 2029.
Introduction
Multiple primary malignancies in a single patient was first described by Billroth in 1879 [1]. The incidence of Second Primary Cancers (SPC) is on a rising trend owing to the recent improvements in patient care, diagnostic modalities and improved therapeutic regimens [1,2]. The frequency of multiple primary malignant tumors is expected to increase as the population age. The risk of SPC in cancer patients is 15-25% higher compared to general population [3], which can be a synchronous malignancy or metachronous. Synchronous is defined as a primary occurring within 6months of the first primary cancer and metachronous is defined as primary occurring 6 months or more after the first [4].
We hereby describe an extremely unusual case of 52-years-old-female with neuroendocrine carcinoma of vaginal vault developing four years after undergoing nephrectomy for Renal Cell Carcinoma (RCC).
Case Report
A 52-years-old-female presented with bleeding per vaginum and foul smelling vaginal discharge since 2 months. On examination she was found to have a 3 x 3cm vaginal vault mass. Total abdominal hysterectomy and bilateral salpingo-oopherectomy was done 4 years back for fibroid uterus. Patient was a known case of clear cell carcinoma, Left kidney and underwent left sided nephrectomy for the same in June 2016.
Ultrasound whole abdomen revealed a mixed echogenic area measuring 3.9 x 3.8 cm in place of uterus. MRI revealed a lobulated expansile enhancing mass of vault with mild parametrial stranding. There was no evidence of bladder or bowel involvement. A clinical diagnosis of metastatic RCC was suspected and a pap smear was sent to Department of Pathology.
Papanicolaou stained smears were highly cellular comprising of singly scattered, small round cells with high nucleo-cytoplasmic ratio, finely granular/stippled chromatin, and inconspicuous nucleoli. A diagnosis of small round cell tumour of vaginal vault was given and excision biopsy was adviced (Figure 1).
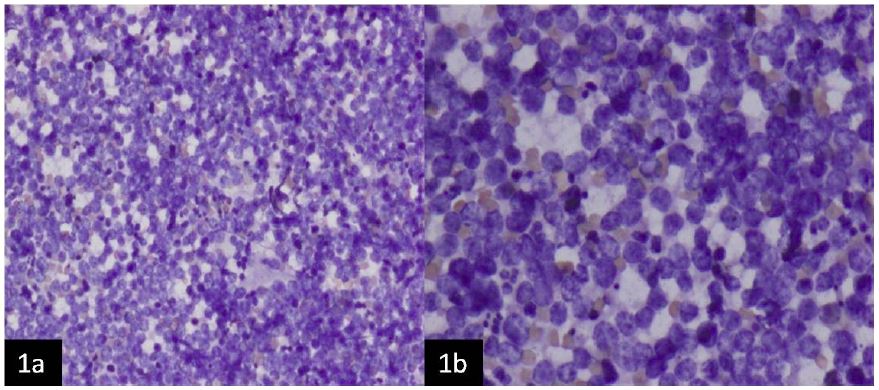
Figure 1: Papaniculao stained smears (a): (100x) and (b): (200X) are highly cellular comprised of singly scattered small round cells with high nucleo-cytoplasmic ratio, finely granular/stippled chromatin and inconspicuous nucleoli.
Vault biopsy revealed tumour cells arranged in sheets and nests. The cells exhibited high nucleo-cytoplasmic ratio with brisk mitoses, powdery nuclear chromatin and inconspicuous nucleoli (Figure 2).
On immunohistochemistry (Figure 3), tumor cells were positive for synaptophysin. CK and CD10 were negative ruling out metastasis from RCC.

Figure 2: (a): H&E, 40X: Section shows multiple tissue bits showing small round cells arranged in sheets & nests with large areas of necrosis. (b): H&E, 200X: Showing high power view with nuclear details and inconspicuous nucleoli.
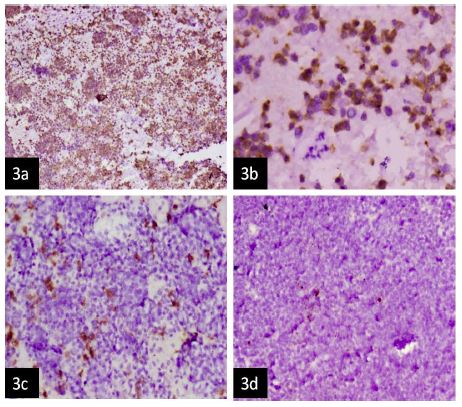
Figure 3: (a): On immunohistochemistry, tumor cells showing positivity for Synaptophysin, 40X (b): High power view (400X) showing tumor cells demonstrating membranous positivity for Synaptophysin. Cells were diffusely negative for (c): CD10 (100X); (d): CK (100X).
Final diagnosis given was neuroendocrine carcinoma, vaginal vault.
Patient was started on adjuvant chemotherapy with Carboplatin and Etoposide. A PET CT was done after one month which did not reveal definite evidence of any abnormal hypermetabolic focus/lesion. Follow up Papanicolaou smears were negative for intraepithelial lesion or malignancy.
The patient underwent Radical Radiation therapy with External Beam Radiation Therapy followed by Vaginal SORBO Brachytherapy.
Discussion
The occurrence of multiple malignancies in a single patient has been reported since almost 10 decades now [1]. The neoplasms may be limited to a single solid organ or multiple organs may be invloved or there can be a hematopoietic malignancy [3]. Warren and Gates gave the criteria used for diagnosis of dual malignancies, which are as follows [1]:
α) Histological confirmation of malignancy in both the index and secondary tumors.
β) There should be at least 2 cm of normal mucosa between the tumors. If the tumors are in the same location, then they should be separated in time by at least five years.
χ) The probability of one being the metastasis of the other must be excluded.
The pathogenesis of dual malignancies has not been fully elucidated in the literature. Multiple factors are believed to have a role in the pathogenesis of dual malignancies such as family history of cancers, genetic susceptibility, intensive exposure to chemotherapeutic agents and radiotherapy [5]. Genomic instability has been found to occur more frequently in cases of multiple primary malignancies than in sporadic cancers [6].
A markedly increased risk of second primary malignancy has been well established in patients with head and neck squamous cell carcinoma. Patients with squamous cell carcinoma have been reported to have approximately 36% cumulative life time risk of developing SPC over a period of 20 years [7].
Ten percent of RCC have been reported to be associated with SPC as per Surveillance Epidemiology and End Results (SEER) database [8]. However a study in Norway reported this incidence to be 47% [9]. This difference could be attributed to environmental and genetic differences. The most common sites of second malignancies after RCC are the male genital system, gastrointestinal system and respiratory system, together constituting 58% of SPCs in cases of RCC. The incidence of SPC in female genital system after RCC is found to be less than 2% [8]. A thorough literature search did not reveal even a single case of neuroendocrine carcinoma, that too of vaginal vault after RCC.
Primary small cell neuroendocrine carcinoma of vault is extremely rare with paucity of literature. The Papanicolauo smears helped us clinch the diagnosis where the clinical suspicion was a metastatic RCC. It being seen as a metachronous SPC after RCC makes this case extraordinarily exceptional. The etiology of multiple primary carcinomas is perplexing and includes multiple factors. Complete evaluation of the patient presentation and clinical follow up might help in elucidating new horizons for diagnosis and management of such patients.
Conclusion
The study of metachronous malignancies may provide important insight into the etiopathogenesis and future management of cancers including development of effective screening and surveillance protocols, with the goal to treat patients effectively.
References
- Warren S, Gates D. Multiple primary malignant tumor: A survey of the literature and a statistical study. Am J Cancer. 1932; 51: 1358-1414.
- Agrawal R. Synchronous dual malignancy: Successfully treated cases. J Cancer Res Ther. 2007; 3: 153-156.
- Sung H, Hyun N, Leach CR, Yabroff KR, Jemal A. Association of First Primary Cancer With Risk of Subsequent Primary Cancer Among Survivors of Adult-Onset Cancers in the United States. JAMA. 2020; 324: 2521-2535.
- Suzuki T, Takahashi H, Yao K, Inagi K, Nakayama M, et al. Multiple primary malignancies in the head and neck: A clinical review of 121 patients. Acta Otolaryngol Suppl. 2002; 547: 88-92.
- Escobar PA, Smith MT, Vasishta A, Hubbard AE, Zhang L. Leukaemia-specific chromosome damage detected by comet with fluorescence in situ hybridization (comet-FISH). Mutagenesis. 2007; 22: 321-327.
- Horii A, Han HJ, Shimada M, Yanagisawa A, Kato Y, et al. Frequent replication errors at microsatellite loci in tumors of patients with multiple primary cancers. Cancer Res. 1994; 54: 3373-3375.
- Morris LG, Sikora AG, Hayes RB, Patel SG, Ganly I. Anatomic sites at elevated risk of second primary cancer after an index head and neck cancer. Cancer Causes Control. 2011; 22: 671-679.
- Chakraborty S, Tarantolo SR, Batra SK, Hauke RJ. Incidence and prognostic significance of second primary cancers in renal cell carcinoma. Am J Clin Oncol. 2013; 36: 132-142.
- Beisland C, Talleraas O, Bakke A, Norstein J. Multiple primary malignancies in patients with renal cell carcinoma: a national population-based cohort study. BJU Int. 2006; 97: 698-702.
