
Open Access, Volume 9
Thyroid-like intrahepatic cholangiocarcinoma: An easily misdiagnosed case and molecular features analysis
Pengfei Xu1; Lifang Fan1; Junqiu Yue1; Lei Li2; Fang Guo1*
1Department of Pathology, Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei 430079, China.
2Department of Nuclear Medicine, Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei 430079, China.
Fang Guo
Department of Pathology, Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei 430079, China.
Tel: +8618995611330;
Email: 542495649@qq.com
Received : March 16 2023,
Accepted : April 24, 2023
Published : April 27, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Thyroid-like intrahepatic cholangiocarcinoma is a rare and easily misdiagnosed malignant neoplasm. Five cases in surgical specimen have been reported in the English literature while lack comprehensive gene mutations analysis. We recently encountered a case of this tumor in biopsy tissues that histologically highly resembles thyroid follicular tumor and harbors PIK3CA, TP53, CDK12, MAP3K13 and SDHC mutations.
Keywords: Thyroid-like intrahepatic cholangiocarcinoma; Intrahepatic cholangiocarcinoma; Pathologic diagnosis; Morphology; Follicular; Gene mutation.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Guo F (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Xu P, Fan L, Yue J, Li L, Guo F. Thyroid-like intrahepatic cholangiocarcinoma: An easily misdiagnosed case and molecular features analysis. Open J Clin Med Case Rep. 2023; 2026.
Introduction
Thyroid-like intrahepatic cholangiocarcinoma (ICCA) is a rare variant composed of small ducts mimic with morphologic characteristics of thyroid follicular tumor. The unusual morphologic variant is not included in the latest version of world Health Organization classification of ICCA [1]. Five cases [2-6] have been reported and all patients were diagnosed after received operation. The molecular features of this tumor have been described by one case report, and the molecular analysis revealed frameshift mutations in 2 chromatin-remodeling genes, CREBBP and KMNT2A [6]. The molecular alterations of this tumor remain to be fully elucidated. However, for advanced patients who have lost the surgical opportunity, needle biopsy is the only effective method to clarify diagnosis and develop a proper therapy strategy, especially for targeted therapy or immunotherapy. Embarrassingly, to diagnose thyroid-like ICCA in needle biopsy tissue and detect gene variants further is a big challenge for pathologist basic on the limited tissue. Herein, we present a case of thyroid-like ICCA of a 21-year-old man who received needle biopsy and gene variation analysis.
Case Report
Clinical Summary
A 21-year-old man presented with a 11-month history of abdominal distension, abdominal pain and occasional vomiting. Positron emission tomography–computed tomography (PET-CT) revealed a 12.9 × 15.1 cm, well-encapsulated, low-density and heterogeneous enhanced lesions with necrosis and calcification in the right lobe of the liver (Figure 1). Furthermore, multiple low-density nodules and the largest one was about 16.2 × 6.9 cm were also detected in the left lobe of the liver. No mass lesions were detected in other organs, including the thyroid gland, kidneys, breast, prostate and cervical lymph nodes. Radiological diagnosis were primary liver cancer with intrahepatic metastasis. Viral markers were non-reactive. Serum alpha fetoprotein (AFP) was 5.80 IU/ml (normal limit was < 5.5 IU/ML) and carbohydrate antigen 199 (CA199) was 81.89 U/ML (normal limit was < 27 U/ML). Thyroid function tests were normal. The patient underwent needle biopsy of the mass in the right lobe of liver, then received transcatheter arterial chemoembolization and protective liver treatment. At the final follow-up 8 months after the initial tumor puncture, the patient was alive without tumor development or new metastasis.
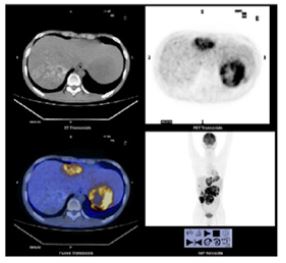
Figure 1: The volume of the liver is obviously increased. Multiple slightly low-density nodules and masses are seen in the liver. The density is uneven, with necrosis and calcification in some parts. The larger one is located in the right lobe of the liver, and the maximum cross-section size is about 12.9 cm × 15.1 cm.
PET showed increased partial radioactivity uptake at corresponding sites, with SUV max of about 12.7. Many calcifications in the tumor are showed and the metabolism of the lesion is different.
Pathological Findings
Three pieces of tumor tissues with 1.5 cm to 2 cm in lengths and 0.2 cm in wide were showed in pathological sections. Microscopically, The residual liver showed non-hepatitis and non-cirrhotic. The tumor has many follicles that vary in size. The tumor follicles, filled with eosinophilic colloid-like material within the lumens and lined with goiter-like vacuolation around the edge that highly resembles thyroid follicular tumor (Figure 2A). Macro and micro follicles grow in diffuse, nested or solid growth pattern. Inconsistent with reported literature, no clear nuclei, nuclear grooves or nuclear pseudo inclusions were present in the tissue and no papillary components were observed. Different from classical ICCA, dilated follicles in thyroid-like ICCA invade and destroy local hepatocytes but without desmoplasia surrounding. Lympho-vascular invasion was absent in the limited tumor tissue. In the solid areas, cells arranged cords or trabecular (Figure 2B). Some of them had obviously atypia, necrosis and mitotic figures (Figure 2C).
Immunohistochemically, all the tumor cells diffusely and strongly expressed cytokeratin 7 (CK7) (Figure 3A). Approximately 90% of tumor cells were strongly positive of Cytokeratin 19 (CK19) (Figure 3B) and the lest 10% of tumor cells were weakly positive almost limited in the solid areas and showed higher cell proliferation index (Ki67)comparing with other area (Figure 3C). Beside these, thyroid transcription factor 1 (TTF1), paired-box gene 8 (PAX8), human hepatocyte marker 1 (hepar1), Glypican-3, alpha fetoprotein (AFP), cluster of differentiation 10 (CD10), chromogranin (CgA), synaptophysin (Syn), neural cell adhesion molecule 1 (NCAM1/CD56) and sal-like protein-4 (Sall4) were all performed and stained negatively.
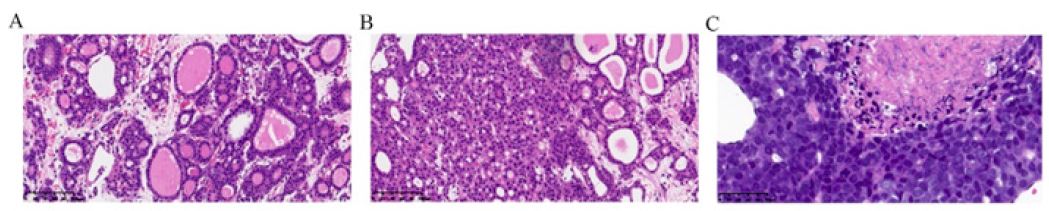
Figure 2: The morphological characteristics of Thyroid-like intrahepatic cholangiocarcinoma (HE stain). Nests of tumor cells arranged in cystically dilated glands with thin fiber spacing but without desmoplasia. Those glands contain colloid-like and brightly eosinophilic secretions reminiscent of thyroid follicles (A, x 200). Broad trabaculae of tumor cells were showed in the solid areas (B, x 200). High-grade tumor cells showed obvious atypia, including hyperchromatic and enlarged nuclei, scant cytoplasm, increased mitotic figures and extensive necrosis (C, x 400).

Figure 3: The immunohistochemical profile of Thyroid-like intrahepatic cholangiocarcinoma. Tumor cells were diffusely and strongly positive for CK7 (A, x400) and CK19 (B, x400) in cytoplasm. The carcinoma had a higher Ki-67 proliferation index (approximately 10% to 20%) in the solid areas comparing with the other area (C, x400).
Variation analysis of 520 genes was performed in next generation sequencing. Interesting, many genes were found harbored mutations (Figure 4), including PIK3CA (10 exon, p.E545K missense mutation c.1633G>A,p.Glu545Lys), TP53 (5 exon, p.K132N missense mutation, c.396G>T, p.Lys132Asn), CDK12 (missense mutation c.298C>G, c.233C>A), MAP3K13 (missense mutation c.1605G>C) and SDHC (nonsense mutation c.61C>T). However, no mutation was detected in genes related to targeted drugs, such as ALK, BRAF, BRCA1/2, EGFR, ERBB2, KIT, KRAS, MET, NRAS, NTRK1/2/3, PDGFRA, RET and ROS1. Moreover, no pathogenic or possibly pathogenic germline variation was detected. The tumor mutation burden was 3.99 mutation / MB and the micro-satellite instability (MSI) test results were stabilized.

Figure 4: The genes variation of thyroid-like intrahepatic cholangiocarcinoma by next generation sequencing. Missense mutation c.1633G>A (p.E545K) of PIK3CA gene (A), missense mutation c.396G>T (p.K132N) of TP53 gene (B), missense mutations c.298C>G (p.Arg100Gly) and c.233C>A (p.Ser78Tyr) of CDK12 gene (C, D), missense mutation c.1605G>C (p.Arg535Ser) of MAP3K13 gene (E) and nonsense mutation c.61C>T (p.Gln21*) of SDHC gene (F) were identified.
Discussion
Microscopically, it is extremely useful clues to diagnose thyroid-like ICCA in liver if the tumor cells contain characteristics of a thyroid neoplasm, especially in small biopsy sample. In our case, 70% tumor cells formed micro or macro follicles that filled with full of eosinophilic colloid-like material. The follicles clustered together closely and the interfollicular tissue showed scanty fibrous connective tissue without microcalcifications. Most of follicles had bland appearance and lack of features of thyroid papillary carcinoma nucleus and only 10% tumor cells of focus area had evident cellular atypia and mototic figures. Basing on mophological features, the diagnosis of metastatic well-differentiated thyroid carcinoma was the first consideration. Because ectopic thyroid gland in the porta hepatis was described in few reports [7-9], malignant transformation derived from ectopic thyroid gland was another possibility. But absence of a primary thyroid tumor and negative TTF1 and PAX8 immunohistochemical staining excluded the initial consideration and favored the description of ICCA. Being the new morphological variant of ICCA, thyroid-like ICCA often lack of significantly desmoplastic stroma which is common in conventional ICCA. The small glands (follicles) dilate roundly in thyroid-like ICCA but always are pinched by desmoplastic stroma into slit shape or strip shape in conventional ICCA. Immunohistochemical staining serves no useful purpose to identify thyroid-like ICCA from conventional ICCA.
Well-differentiated hepatocellular carcinoma with acinar pattern or neuroendocrine tumor/carcinoma should be considered in the differential diagnosis. Though the expression pattern of CD34 (not shown) mimicked the hepatocellular carcinoma, the lack reactivity of hepar1, Glypican-3, AFP and CD10 while high expression of CK7 and CK19 ruled out the diagnosis of hepatocellular carcinoma [10] and supported the diagnosis of ICCA. The neuroendocrine markers, including CgA, Syn and CD56 were negative that excluded the possibility of neuroendocrine tumor/carcinoma [11-13]. Likewise, negative expression of germ cell marker (Sall4) also excluded the diagnosis of germ cell tumor.
In this case, IHC staining had been a marvelous help in ascertaining the tissue origin and avoiding erroneous classification. Molecular biology of this newly recognized variant of ICCA is still unclear. A series of previously published English studies [14-16] have confirmed a variety of gene mutations in ICCA, including the genes within the RAS and PI3K pathways, the genes related to cell-cycle control proteins (CDKN2A/CDKN2B, CDK4/6) and the genes of TP53, IDH1 and IDH2. Gene fusions (FGFR2 and NTRK1) and gene amplifications (EGFR and MET) have been observed in ICCA. Similar to ICCA, variation analysis of 520 genes in this case also showed PIK3CA, TP53, CDK12, MAP3K13 and SDHC mutations. The PI3K/PTEN/AKT pathway, one of the two major EGFR-mediated pathways, is involved in a cascade of cell survival and anti-apoptotic signals [17] PIK3CA gene mutations were rare but were found more frequent than BRAF gene mutations in Chinese ICCA patients and were always detected positively at those patients with a early stage [18]. The limited researches inferred that patients with PIK3CA mutations had a significantly longer median progression-free survival [19]. However, in this case, the tumor tissue also harbored TP53 gene mutations which were always associated with lower Overall Survival (OS) and higher tumor recurrence [20]. At the final follow-up 7 months after the initial tumor puncture, the patient was alive and received two times of transcatheter arterial chemoembolization (TACE) according to the treatment strategy of ICCA. No new metastases to lymph nodes or distant sites were found.
Conclusions
In conclusion, we report the fifth case while the first small biopsy sample of thyroid-like ICCA. Furthermore, we firstly explore its molecular characteristics by analyzing 520 gene mutations. Though one case is not sufficient to draw a conclusive interpretation, the molecular findings in the case confirmed again this tumor’s ICCA origin.
Declarations
Author contributions: All authors have made significant contributions, and all authors agree with the content of the manuscript. Lifang Fan and Junqiu Yue anticipated this case discussion and gave more suggestion. Lei Li evaluated the radiographical images and provided the figures with PET-CT scans. Fang Guo analyzed the molecular profiling data. Fang Guo and Pengfei Xu wrote the paper and Fang Guo reviewed the literature.
Acknowledgments: The authors are grateful to the patient for agreement to publication of the report.
Funding: This research was funded by the Hubei science and technology program (2020CFB869).
Conflict of Interest: No potential conflict of interest relevant to this article was reported. The authors declare no conflict of interest.
References
- WHO Classification of Tumours Editorial Board. Digestive system tumors. 5th ed. Lyon, France: IARC Press, 2019; 254-259.
- Fornelli A, Bondi A, Jovine E, Eusebi V. Intrahepatic cholangiocarcinoma resembling a thyroid follicular neoplasm. Virchows Arch. 2010; 456: 339-342.
- Mittal N, Bal M, Ramadwar M, Patkar S, Goel M. Pathologic Doppelgänger: Thyroid-like intra-hepatic cholangiocarcinoma with synchronous primary thyroid carcinoma in a young woman. Ann Hepatobiliary Pancreat Surg. 2020; 24: 182-187.
- Chablé-Montero F, Shah BSA, Montante-Montes de Oca D, Angeles-Ángeles A, Henson DE, et al. Thyroid-like cholangiocarcinoma of the liver: an unusual morphologic variant with follicular, trabecular and insular patterns. Ann Hepatol. 2012; 11: 961-965.
- Chen SH, Zheng ZY, Wang HL, Yu YH, Zeng DH, et al. Thyroid-Like Intrahepatic Chol-angiocarcinoma: Report of a Case and Review of the Literature. Int J Surg Pathol. 2018; 26: 649-654.
- Hissong E, Chiu K, Park H, Solomon J, Song W, et al. Thyroid-Like Cholangiocarcinoma: Histopathological, Immunohistochemical, In-Situ Hybridization and Molecular Studies on an Uncom-mon Emerging Entity. Int J Surg Pathol. 2021; 29: 920-925.
- Chooah O, Ding J, Fei JL, Xu FY, Yue T, et al. Radiological insights of ectopic thyroid in the porta hepatis: A case report and review of the literature. World J Clin Cases. 2021; 9: 3432-3441.
- Ghanem N, Bley T, Altehoefer C, Högerle S, Langer M. Ectopic thyroid gland in the porta hepatis and lingua. Thyroid. 2003; 13: 503-507.
- Sekine S, Nagata M, Hamada H, Watanabe T. Heterotopic thyroid tissue at the porta hepatis in a fetus with trisomy 18. Virchows Arch. 2000; 436: 498-501.
- Durnez A, Verslype C, Nevens F, Fevery J, Aerts R, et al. The clinicopathological and prognostic rele-vance of cytokeratin 7 and 19 expression in hepatocellular carcinoma. A possible progenitor cell origin. Histopathology. 2010; 49: 138-151.
- Jin M, Zhou X, Yearsley M, Frankel WL. Liver Metastases of Neuroendocrine Tumors Rarely Show Overlapping Immunoprofile with Hepatocellular Carcinomas. Endocrine Pathology. 2016; 27: 1-6.
- Lloyd RV . Practical markers used in the diagnosis of neuroendocrine tumors. Endocrine Pathology. 2003; 14: 293-301.
- Pavel M, Berg K, Falconi M, Frankel WL. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology. 2020; 3: 844-860.
- Ross JS, Wang K, Gay L, Al-Rohil R, Rand JV, et al. New routes to targeted therapy of intrahepatic cholangiocarcinomas revealed by next-generation sequencing. Oncologist. 2014; 19: 235-242.
- Churi CR, Shroff R, Wang Y, Rashid A, Kang HC, et al. Mutation pro-filing in cholangiocarcinoma: prognostic and therapeutic implications. PLoS One. 2014; 9: e115383.
- Lowery MA, Ptashkin R, Jordan E, Berger MF, Zehir A, et al. Comprehensive Molecular Profiling of Intrahepatic and Extrahepatic Cholangiocarcinomas: Potential Targets for Intervention. Clin Cancer Res. 2018; 24: 4154-4161.
- Yuan TL, Cantley LC. PI3K pathway alterations in cancer: variations on a theme. Oncogene. 2008; 27: 5497-5510.
- Xu RF, Sun JP, Zhang SR, Zhu GS, Li LB, et al. KRAS and PIK3CA but not BRAF genes are frequently mutated in Chinese cholangiocarcinoma patients. Biomed Pharmacother. 2011; 65: 22-26.
- Trachu N, Sirachainan E, Larbcharoensub N, Rattanadech W, Detarkom S, et al. Molecular alterations and clinical prognostic factors for cholangiocarcinoma in Thai population. Onco Targets Ther. 2017; 10: 4955-4968.
- Nepal C, O’Rourke CJ, Oliveira DVNP, Taranta A, Shema S, et al. Genomic perturbations re-veal distinct regulatory networks in intrahepatic cholangiocarcinoma. Hepatology. 2018; 68: 949-963.
