
Open Access, Volume 9
Complete reversal of arrhythmia-induced cardiomyopathy: Case report
Radu Darciuc1*; Irina Boiciuc1; Anatolie Cazacu2; Hakan Eraslan1; Erdem Diker1,3
1Department of Cardiology, Medpark International Hospital, Chisinau, Republic of Moldova.
2Department of Radiology, German Diagnostic Center, Chisinau, Republic of Moldova.
3Department of Cardiology, Bayındır Sogutozu Hospital, Ankara, Turkey.
Radu Darciuc
Cardiologist, Medpark International Hospital, 24 Andrei Doga street, MD-2024, Chișinău, Republic of
Moldova.
Email: rdarciuc@yahoo.com
Received : March 09, 2023,
Accepted : April 19, 2023
Published : April 21, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Several published data confirm the fact that arrhythmias could induce dilated cardiomyopathy referred as arrythmia-induced cardiomyopathy (AiCMP). It could be caused either by incessant supraventricular tachycardias, atrial fibrillation, atrial flutter, incessant ventricular tachycardias or premature ventricular contractions. Reversal of cardiomyopathy by elimination of the arrhythmia confirms the diagnosis of AiCMP. We present a case of a patient with AiCMP caused by incessant Right Ventricular Outflow Tract (RVOT) tachycardia who was cured by radiofrequency ablation.
Keywords: Ablation; Heart failure; Radiofrequency; Ventricular tachycardia.
Abbreviations: AiCMP: Arrythmia-Induced Cardiomyopathy; LBBB: Left Bundle Branch Block; LVEF: Left Ventricular Ejection Fraction; MRI: Magnetic Resonance Imaging; PVC: Premature Ventricular Contractions; RF: Radiofrequency; RVOT: Right Ventricular Outflow Tract; TTE: Transthoracic Echocardiography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Darciuc R (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Darciuc R, Boiciuc I, Cazacu A, Eraslan H, Diker E. Complete reversal of arrhythmia-induced cardiomyopathy. Case Report. Open J Clin Med Case Rep. 2023; 2023.
Introduction
Tachycardia-induced cardiomyopathy was first described by Gossage et all in 1913 in a patient with atrial fibrillation with rapid ventricular response [1]. In the last years several published data confirm the fact that arrhythmias could induce dilated cardiomyopathy referred as arrythmia-induced cardiomyopathy (AiCMP) [2-4]. It could be caused either by incessant supraventricular tachycardias, atrial fibrillation, atrial flutter, incessant ventricular tachycardias or premature ventricular contractions (PVC) burden ≥10%.
The landmark of AiCMP is the presence of ventricular dysfunction in a patient with an arrhythmia and its recovery once the arrhythmia is eliminated.
Case Presentation
We present a case of a 44-years-old man who was admitted in 2017 to Medpark International Hospital, Chisinau, Republic of Moldova for radiofrequency ablation.
The patient has started to feel palpitations in 2005 with a duration of minutes. A paroxysm with a regular wide complex tachycardia with Left Bundle Branch Block (LBBB) morphology, inferior axis and transition in V4 was documented by ECG (Figure 1). The patient was evaluated by Transthoracic Echocardiography (TTE) with no heart chamber enlargement and normal left ventricular ejection fraction (LVEF) (57%). Latterly, the tachycardia became more frequent and longstanding.
In 2014 he was admitted for additional investigations in a tertial center. A 24 hours Holter ECG monitoring was performed that recorded a ventricular tachycardia with the heart rate of 130-152 b/min, solitary sinus captured beats and a short episode of sinus rhythm (from 4:17 PM till 4:30 PM). The patient was evaluated by TTE with the detection of the decreased LVEF - 25% (Table 1). The coronarography shoved normal coronary arteries. He was also evaluated by cardiac magnetic resonance imaging (MRI) with the detection of a dilative cardiomyopathy pattern, without any changes suggestive for arrhythmogenic right ventricle dysplasia (Figure 2).
In March 2015 an invasive electrophysiological study was performed in the same tertiary center, that confirmed the presence of a ventricular tachycardia and the daily treatment with amiodarone 200mg, aspirin 75mg, spironolactone 25mg and ramipril 5mg was recommended. Nevertheless, he continued to complain palpitations and progression of the dyspnea.
In September 2017 he was admitted to our center for Radiofrequency (RF) ablation of the ventricular tachycardia. During the electrophysiological study the tachycardia with origin in the right anterior area of the right ventricular outflow tract (RVOT) was easily induced. The RF currents were applied in that region with the disappearance of the tachycardia (Figure 3) and no recurrence after 15 minutes waiting period.
At the discharge we recommended the treatment with daily bisoprolol 2.5 mg, aspirin 75 mg and spironolactone 25 mg.
After 6 months the patient was reevaluated by 24 hours Holter ECG monitoring with the detection of only 16 PVC with both right bundle branch block and LBBB morphology. On TTE there were complete normalization of the LVEF and the heart chambers size (Table 1). The medical therapy was discontinued.
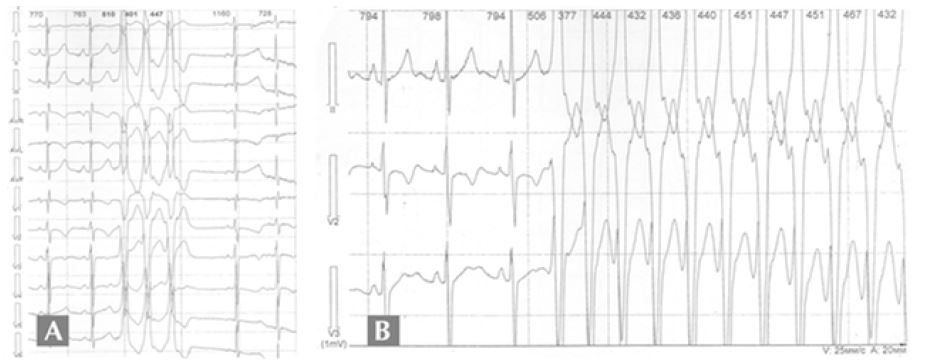
Figure 1: Electrocardiogram
A. Ventricular triplet with Left Bundle Branch Block morphology, inferior axis and transition in V4.
B. Onset of the ventricular tachycardia.
A. Ventricular triplet with Left Bundle Branch Block morphology, inferior axis and transition in V4.
B. Onset of the ventricular tachycardia.

Figure 2: Cardiac magnetic resonance imaging. Cardiac magnetic resonance demonstrating an absence of scars with late-gadolinium enhancement.
Table 1: Transthoracic echocardiography parameters before and after ablation of the ventricular tachycardia. The ablation was performed in September 2017.
| Date | LA | LV | LVEF | RA | RV | MVI |
|---|---|---|---|---|---|---|
| (mm) | (mm) | (%) | (mm) | (mm) | (degree) | |
| 13.12.2005 | 30 | 49 | 57 | 32 | 23 | I |
| 08.07.2014 | 52 | 65 | 25 | 57 | 30 | III |
| 23.03.2015 | 48 | 68 | 30 | 40 | 30 | III |
| 24.04.2018 | 38 | 54 | 60 | 39 | 25 | II |
LA: Left Atrium; LV: Left Ventricle; LVEF: Left Ventricular Ejection Fraction; MVI: Mitral Valve Insufficiency; RA: Right Atrium; RV: Right Ventricle.
Discussion
In a patient with persistent or paroxysmal arrythmia and ventricular dysfunction the AiCMP should be suspected. In our patient there were some clues to the diagnosis of the AiCMP as normal TTE parameters in the onset of the disease and the absence of positive late gadolinium enhancement areas on cardiac MRI.
According to the fact that there was an incessant monomorphic VT from RVOT the best available treatment was RF ablation of the arrythmia. There are huge amount of data starting from the 90’s [5] that confirms the usefulness of the ablation therapy in the management of AiCMP.
Our suspicion that the cardiomyopathy is actually an AiCMP was confirmed by the complete normalization of the LVEF and the dimensions of heart chambers after RF ablation.
Conclusion
PVC and/or VT can induce dilated cardiomyopathy that is reversable if the appropriate treatment is applied. In our patient the AiCMP was cured by radiofrequency ablation of the RVOT tachycardia with the complete normalization of the LVEF and the heart chambers size in the following months after procedure.
With unproper treatment the heart failure would progress leading to marked disability and decrease of the quality of life.
The use of the RF ablation as an optimal treatment has led to complete reversal of the cardiomyopathy and complete withdrawal of cardiac medication.
Declarations
Funding: The authors have no funding to report.
Competing interests: The authors have declared that no competing interests exist.
Acknowledgements: The authors have no support to report.
References
- Gossage AM, Braxton Hicks JA. On auricular fibrillation. Q J Med. 1913; 6: 435-440.
- Jain A, Selvaraj RJ. Arrhythmia-Induced Cardiomyopathy. Indian Journal of Clinical Cardiology. 2021; 2: 90-96.
- Huizar JF, Ellenbogen KA, Tan AY, Kaszala K. Arrhythmia-Induced Cardiomyopathy: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019; 73: 2328-2344.
- Gopinathannair R, Etheridge SP, Marchlinski FE, Spinale FG, Lakkireddy D, Olshansky B. Arrhythmia-Induced Cardiomyopathies: Mechanisms, Recognition, and Management. J Am Coll Cardiol. 2015; 66: 1714-1728.
- Matsuura Y, Chin W, Kurihara T, Yasui K, Asao M, et al. Tachycardia-induced cardiomyopathy: a case report. J Cardiol. 1990; 20: 509-518.
