
Open Access, Volume 9
Intraoperative hysteroscopy and transrectal ultrasound to facilitate genital reconstruction in a female patient with clitoromegaly due to congenital adrenal hyperplasia: A case report
Gonzalo Mezquita
Hospital Universitario Ramony Cajal, Spain.
Email: gonzalo.mezquita@salud.madrid.org
Received : March 11, 2023,
Accepted : April 17, 2023
Published : April 21, 2023,
Archived : www.jclinmedcasereports.com
Abstract
We present the case of a 29-year-old female who had atypical genitalia due to congenital adrenal hyperplasia secondary to 21-hydroxylase deficiency who underwent reconstructive surgery. We performed a hysteroscopy and intraoperative ultrasound to facilitate the procedure as we consider that this approach could reduce the risk of complications.
Keywords: CAH; DSD; Vagina; Anatomy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Mezquita G (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Mezquita G. Intraoperative hysteroscopy and transrectal ultrasound to facilitate genital reconstruction in a female patient with clitoromegaly due to congenital adrenal hyperplasia: A case report. Open J Clin Med Case Rep. 2023; 2021.
Introduction
Classic Congenital Adrenal Hyperplasia (CAH) is the most common Disorder of Sex Development (DSD), presenting with atypical genital appearance and a 46 XX karyotype in the newborn period [1].
More than 90% of all cases are secondary to 21-hydroxylase deficiency [2]. This group of patients present in the newborn period with atypical genital due to endogenous virilization and without palpable gonads.
Prevalence varies according to geographic area and race, affecting approximately 1 in 15.000 livebirths [3].
Patients with 46 XX CAH and virilization will have a common urogenital sinus and different degrees of clitoral hypertrophy, with normal vagina, cervix, uterus, and ovaries. The aim of the surgical treatment is not only to restore anatomy but to achieve a functional and cosmetic outcome [4].
The optimal timing of surgery is challenging and requires shared decision-making with the family [5].
We report the case of a female with clitoromegaly and low confluence Urogenital Sinus (UGS) due to CAH who underwent genital reconstruction.
Case Presentation
A 29-year-old patient was referred to our department from her local hospital to consider the possibility of genital reconstructive surgery.
She was diagnosed with CAH after birth. Karyotype analysis was 46 XX. She underwent clitoroplasty and labiaplasty at the age of 2 and she had menarche at the age of 13.
On examination there was a small pseudopenis of 3 cm with a narrow orifice just below it (Figure 1). There was no palpable gonad. Other appearances of female secondary sexual features were normal. Further evaluation of the patient did not find other gynaecological or systemic disorders.

Figure 1: Drawings in 6 to 9 months after UCBC therapy.
Gynaecological ultrasound showed a cystic lesion bellow the normal uterus, compatible with a hydrocolpos. The ovaries were normal. The internal genital organs examination revealed the common channel 1.5 cm in length, as a distal unification of the vagina and urethra.
Patient was discussed in our multidisciplinary meeting, and the decision was to perform feminizing genitoplasty with clitoroplasty and vaginoplasty as the procedures of choice.
The procedure started with cysto-vaginoscopy to confirm the anatomy seen preoperatively on MRI and USS, verify the length of the vagina, the connection with the cervix and the location of the bladder neck.
After visualising the anatomy, a bladder catheter was installed in the bladder.
The upper part of her vagina was not connected to the introitus. The rectal ultrasound was used to facilitate the visualization of the hydrocolpos (Figure 2). Therefore, the upper vaginal space was opened under ultrasound guidance and clear liquor drained from it. Methylene blue was used to rule out a bladder connection.
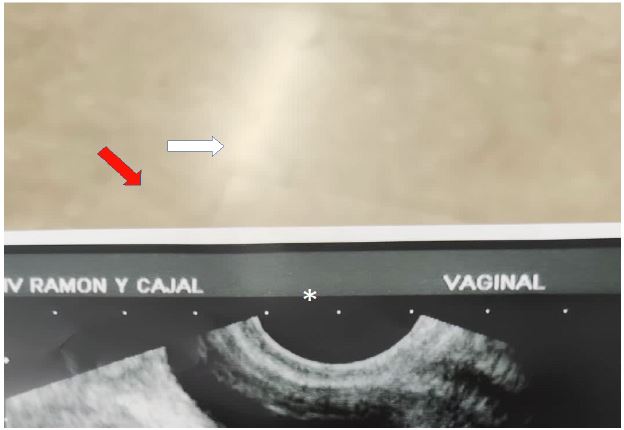
Figure 2: Intraoperative USS showing hydrocolpos (white arrow), bladder (red arrow) and uterus (white asterisk).
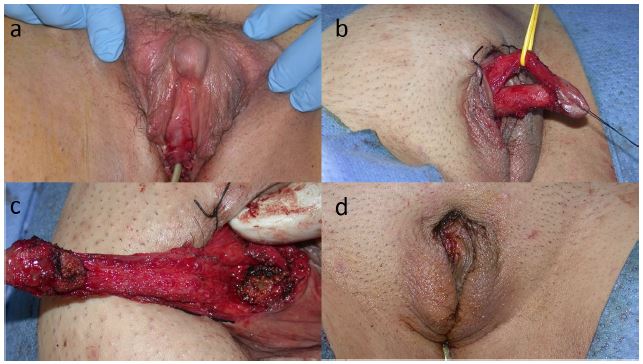
Figure 3: (a) Clinical appearance after vaginoplasty. (b) Traction on the loop separating the neurovascular pedicle from the corpora cavernosa. (c) Removal of the corpora cavernosa. (d) Postoperative appearance.
Vaginoscopy was then performed, and the cervix was visualised. The next step was creating the lower part of the vagina and the detachment of the vagina from the confluence of the common urogenital sinus. A vertical incision was created on the perineum and the separated vagina was then brought out as a separate opening bellow the urethra. Both were then separated and connected to the introitus (Figure 3a).
Clitoral reduction was then performed. The skin of the shaft was mobilised down to the base of the corpora cavernosa by a coronal incision. The next step was the dissection of the neurovascular bundle from the corpora cavernosa finding an avascular plane with a longitudinal incision at 9 and 3 o’clock. The pedicle was separated proximally from the tunica albuginea and a loop was passed through the hole created which facilitated the rest of the dissection of the pedicle from distal to proximal (Figure 3b). Once the corpora were dissected from the dorsal NV pedicle, until their bifurcation under the symphysis pubis, the corpora cavernosa were removed (Figure 3c). Then we had a dorsal strip containing dorsal arteries, nerves, and deep dorsal vein of clitoris under Buck’s fascia supplying the glans. Afterwards, one third of the lateral aspect of the clitoroideal skin was removed to reduce the size of the gland. Finally, the clitoris was reattached to the corporeal stumps near the lower edge of the pelvis with absorbable sutures (Figure 3d).
Discussion
In 46, XX CAH, the vaginal cavity opens into the posterior wall of the urethra at a variable distance from the bladder neck but not higher than where the veru montanum (mullerian structure) is normally located in the male urethra. This confluence is also at variable distance from the perineum depending on the development of the urethra and the increased thickness of the pelvic floor muscles [6]. Prader classification suggested the height of the urethro-vaginal confluence was related to the degree of external masculinization, but we now know this is incorrect. The sagittal fusion of the genital folds is variable from an almost feminine vulva to a complete scrotal-like appearance. In all cases, the gonads are not palpable in the genital folds [7].
Centralization of care is extremely important as genitoplasty procedures are rare. The Chicago Consensus Statement state that only those surgeons experienced in the surgery of DSD should perform these procedures [8].
Optimal timing for surgery is controversial, as it is the surgical technical of choice. Some authors claim the psychological benefits of early surgery, whereas other colleagues prefer surgery at a later stage due to the need for further reconstructive surgery and the inability to obtain signed consent in childhood [8,9].
Sturm and colleagues, in 2015 [1], evaluate the surgical treatment in patients with CAH and found that approximately 90% of feminizing genitoplasty procedures include a vaginoplasty.
Leslie and colleagues [4] state every reconstructive procedure should always begin with a cystovaginoscopy to confirm the anatomy seen with genitography, verify the presence of a single cervix and measure the location of the confluence relative to the introitus and the bladder neck.
In 2016, Lindert et al [10], compared ultrasound findings with the results of endoscopy performed before surgery. From 2006 to 2012, 11 girls had perineal ultrasound and endoscopy. They measured the length of the urogenital sinus, the distance to the vaginal opening into the urogenital sinus, and the length of the bladder neck. They showed that the entrance point of the vagina into the urogenital sinus could be identified in 10 of these girls. The length of the bladder neck and the length of the urogenital sinus could be measured by ultrasound in 10 of 11 girls and were subsequently confirmed by endoscopy. They concluded that widespread use of this technique had the potential to reduce costs and morbidity associated with endoscopy and genitography.
Blanco and colleagues [11] performed a transrectal ultrasound in three patients with CAH and concluded it is ideal to visualize the vagina and the pelvic floor.
In our patient, we decided to perform both a transrectal ultrasound and a cysto-vaginoscopy as this helped us confirm the anatomy and perform the reconstructive procedure.
In this particular case the hydrocolpos was drained under USS guidance after and the vagina was then connected to the introitus.
Clitoroplasty was finally performed, based on the technique described by Kumar et al [12] who emphasized the importance to preserve the nerves and vessels leading to the clitoris while removing the erectile tissue. This procedure preserves the physiological function of the clitoris while removing a variable segment of the corpora cavernosa.
References
- Sturm RM, Durbin-Johnson B, Kurzrock EA. Congenital Adrenal Hyperplasia: Current Surgical Management at Academic Medical Centers in the United States. J Urol. 2015; 193: 1796-1801.
- Speiser PW, Arlt W, White PC, Auchus RJ, Baskin LS, et al. Congenital Adrenal Hyperplasia Due to Steroid 21-Hydroxylase Deficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018; 103: 4043-4088.
- Therrell BL. Newborn Screening for Congenital Adrenal Hyperplasia. Endocrinol Metab Clin North Am. 2001; 30: 15-30.
- Cain M, Rink R, Leslie J. Feminizing genital reconstruction in congenital adrenal hyperplasia. Indian J Urol. 2009; 25: 17.
- Lee PA, Houk CP, Ahmed SF, Hughes IA, in collaboration with the participants in the International Consensus Conference on Intersex organized by the Lawson Wilkins Pediatric Endocrine Society and the European Society for Paediatric Endocrinology. Consensus Statement on Management of Intersex Disorders. Pediatrics. 2006; 118: e488-e500.
- Mouriquand PDE, Gorduza DB, Gay CL, Meyer-Bahlburg HFL, Baker L, et al. Surgery in disorders of sex development (DSD) with a gender issue: If (why), when, and how? J Pediatr Urol. 2016; 12: 139-149.
- Gorduza D, Tardy-Guidollet V, Robert E, Gay CL, Chatelain P, et al. Late prenatal dexamethasone and phenotype variations in 46,XX CAH: Concerns about current protocols and benefits for surgical procedures. J Pediatr Urol. 2014; 10: 941-947.
- Hughes IA, Houk C, Ahmed SF, Lee PA. Consensus statement on management of intersex disorders. J Pediatr Urol. 2006; 2: 148-162.
- Yankovic F, Cherian A, Steven L, Mathur A, Cuckow P. Current practice in feminizing surgery for congenital adrenal hyperplasia; A specialist survey. J Pediatr Urol. 2013; 9: 1103-1107.
- Lindert J, Hiort O, Tüshaus L, Tafazzoli-Lari K, Wünsch L. Perineal ultrasound offers useful information in girls with congenital adrenal hyperplasia. J Pediatr Urol. 2016; 12: 427.e1-427.e6.
- Blanco JA, Pérez C, Jiménez M, Castellví A, Isnard RM, et al. La utilidad de la ecografía transrectal en el diagnóstico de las anomalías de los estados intersexuales. Cir Pediatr. 2003; 16: 4.
- Kumar H, Kiefer JH, Rosenthal IE, Clark SS. Clitoroplasty: Experience during a 19-Year Period. J Urol. 1974; 111: 81-84.
