
Open Access, Volume 9
Flaccid paralysis revealing hyperkalaemia in emergency service in Gabon: A case report and literature review
Edjo Nkilly Ghislain1*; Okoue Ondo Raphael1; Oliveira Stéphane2; Nnang Essone Jean-Fidel3; Mandji-Lawson Jean-Marcel2; Tchoua Romain1
1Department of Anesthesia and Intensive Care and Emergency Unit, Omar Bongo Ondimba Military’s Hospital (HIAOBO), Libreville, Gabon.
2Department of Anesthesia and Intensive Care and Emergency Unit, Akanda Military’s Hospital, Libreville, Gabon.
3Department of Anesthesia and Intensive Care and Emergency unit, Universitary Hospital of Owendo, Libreville, Gabon.
Edjo Nkilly Ghislain
Department of Anesthesia and Intensive Care and Emergency Unit, Omar Bongo Ondimba Military’s
Hospital (HIAOBO), Libreville, Gabon.
Email: edjonkillyghislain@yahoo.fr
Received : March 08, 2023,
Accepted : April 12, 2023
Published : April 17, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Hyperkalaemia is a lethal emergency, which can lead to death by the toxic effect of potassium on myocardial cells. Usual presentation is dominated by cardiac arrhythmias. Flaccid paralysis is a rare presentation of hyperkalaemia in our practice. In Gabon non-traumatic acute flaccid paralysis is often linked to viral attacks. We report the case of a 52-year-old patient admitted to the Emergency Service with a flaccid quadriplegia with progressive evolution. The biologic report showed renal insufficiency (creatinine at 1189 μmol/l) associated with a threatening hyperkalemia (7.8 mmol/l). Complete regression of the clinical picture after the correction of hyperkalemia by renal replacement therapy.
Keywords: Quadriplegia-hyperkalemia; Myocardial cells.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Ghislain EN (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Ghislain EN, Raphael OO, Stéphane O, Jean-Fidel NE, Jean-Marcel ML. Flaccid paralysis revealing hyperkalaemia in emergency service in Gabon: A case report and literature review. Open J Clin Med Case Rep. 2023; 2017.
Introduction
In African daily practice, non-traumatic acute flaccid paralysis is dominated by viral, inflammatory myelitis and polyomyelitis. Progressive paralysis leads to the search for Guillain-Barré disease and often leads to costly examinations (cerebral and spinal cord computed tomography, magnetic resonance imaging, specialized biological examinations). Rarely, severe hyperkalemia is manifested by flaccid paralysis. Myocardial involvement is the most common manifestation of hyperkalaemia. We report the case of a 52-year-old patient who presented with a picture of sudden quadriplegia. The admission assessment revealed renal failure with threatening hyperkalaemia. Clinical picture having evolved favorably with the correction of serum potassium by renal replacement therapy. We conducted a literature review on Pubmed selecting clinical cases.
Case Report
Mr NMH, aged 52, was admitted to the Emergency Reception Service of the Omar Bongo Ondimba Army Instruction Hospital (HIAOBO), in March 2017 for a sudden onset quadriplegia evolving in a non-traumatic context. Her personal history revealed Chronic Renal Insufficiency diagnosed in 2011, and dialysis for 03 years (stopping dialysis sessions since 2014). He benefited from the installation of an arteriovenous fistula and ureteral dilation in 2012, a herniated disc in 2013. There was no alcohol or tobacco intoxication, no toxic intake, long-term nephrotoxic drug.
The patient reported asthenia with anorexia and the sudden tetraparesia and tetraplegia. He consulted at the HIAOBO Emergency Service. Neurological evaluation revealed normal pupils, symmetrical normal bulk and hypotonia in all limbs. Upper limbs had proximal and distal power of 3/5. In lower limbs, proximal and distal power was 2/5 with no sensory deficit. Deep tendon reflexes were absent. Bilaterally the plantar reflexes were mute. There were no lateralizing signs and the cranial nerves were normal. The patient also presented with hyperventilation (respiratory rate 52 cycles/min) without hypoxia (100% SPO2 in ambient air). He was hemodynamically stable (blood pressure 120/60 mmhg) with regular peripheral pulse at 86 beats/min. A biological assessment carried out two days earlier revealed hyperkalaemia at 6.8 mmol/l. The blood ionogram on admission showed hyperkalaemia at 7.8 mmol/L. The rest of the biological assessment objectified hyponatremia (Na + 114.4 mmol/l) with an osmolarity at 303 mOsmol / l, normal chloremia (Cl at 83.1 mmol/l), uremia at 69.0 mmol/l, Creatinine was 1189 μmoL/L (creatinine clearance 6.93 ml/min). Venous blood glucose was 5.2 mmol/L; hemoglobin at 8.9 g/dl; Platelets at 207,000/mm3, leukocytes at 3930/mm3.
The electrocardiogram (ECG) performed on admission showed signs of myocardial involvement (wide, sharp T wave with prolonged RA) (Figure 1).
Immediate management consisted of the administration of calcium gluconate, a bolus of insulin combined with 30% Glucose. He had received a bolus of Furosemide, followed by a session of renal replacement therapy (hemodialysis) before being admitted to intensive care.
The evolution was marked by a complete recovery from quadriplegia and an decrease in renal exam (kaliemia at 5.58 mmol/l, Na + at 117.9 mmol/l; Cl - at 97 mmol/l; Uremia at 47 mmol/l, serum creatinine 878 μmol) after two renal replacement therapy sessions. The post-dialysis ECG had returned to normal (Figure 2). The patient presented with normotonic urine (1500 cc in 24 hours; urine pH 6; negative proteinuria). Complete regression of clinical signs after the second dialysis session, he was transferred to the nephrology service.The other complementary assessments (thyroid assessment, HIV serology) were normal . No morphological exams had been carried out.

Figure 1: Admission ECG.
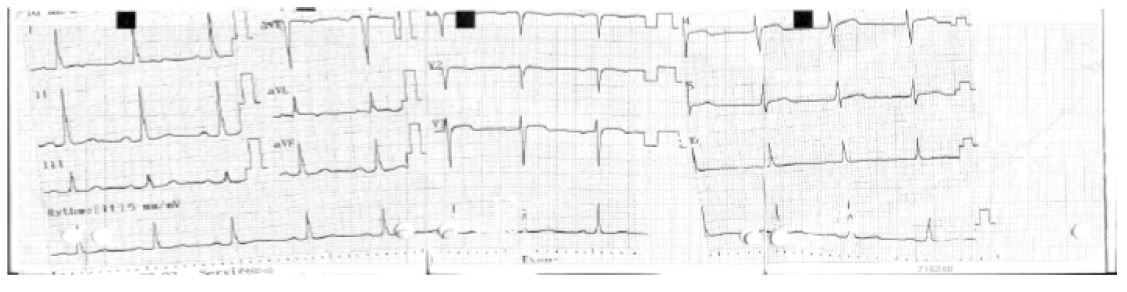
Figure 2: Post-dialysis ECG.
Discussion
The aim of this clinical case was to remind that flaccid paralysis in the emergency department can hide a metabolic etiology in Africa where flaccid paralysis is dominated by polyomyelitis [1], POTT's disease [2], or a rare form of tuberculosis [3]. We must also think of a metabolic etiology, particularly hyperkalaemia, because unlike infectious and inflammatory etiologies, the vital prognosis in the very short term is at stake in the event of hyperkalaemia.
It is not uncommon for hyperkalemia to present with tetra or paraplegia. Indeed, there are motor and sensory neuro-muscular disorders of the type of paresthesia affecting the extremities (limbs, tongue) and/or symmetrical flaccid paralysis with abolition of osteotendinous reflexes evolving in a centripetal manner, with damage to the cranial nerves. Quadriparesis induced by hyperkalemia has been described only in a few case reports.
Kamel KS et al [4] reported the observation of a 73-year-old woman with diabetes, hypertension and hypothyroidism, admitted for progressive flaccid tetraparesis in a context of respiratory failure and threatening hyperkalaemia (9.1μmol/l ). The symptomatology had completely regressed after correction of the hyperkalaemia by non-specific measures (calcium gluconate, insulin-dextrose solution, furosemide, beta-2 agonist nebulization, calcium sulfonate and sorbitol) associated with non-ventilation. invasive (NIV) for his respiratory failure.
Panichpisal K et al [5] report the observation of a 52-year-old man with end-stage chronic renal failure who presented with ascending quadriplegia and dyspnea for 2 days. He had hyperkalaemia (9.0 mEq/L) with electrocardiographic signs. Her symptoms were completely resolved within 5 hours of treatment for hyperkalemia.
Christian T. Braun et al in 2014 [6] reported the observation of a 58-year-old male patient admitted for generalized asthenia with bradycardia at 30 beats per minute. He also presented progressive paraparesis for 3 days leading to quadriplegia without damage to the cranial nerves, all associated with significant hyperkalaemia (9.9mmol/l) in connection with the use of aldosterone antagonists. Here too, symptomatology improved with symptomatic measures against hyperkalaemia and extra-renal purification.
The majority of publications report peripheral neurological damage evolving in a context of hyperkalaemia around 9 mmol/l. The major symptoms being osteotendinous hyporeflexia, quadriparesis/paralysis, more or less associated with respiratory damage and sensory loss. Complete recovery of the neurological deficit occurred after correction of hyperkalaemia by medicinal means, whether or not associated with extra-renal purification [7-10].
The most frequently reported causes of hyperkalemia-induced acute flaccid quadriparesis are renal insufficiency, use of potassium-sparing drugs or a combination of both. Some case was due to tumor lysis syndrome [11]. In these case reports, potassium levels ranged from 8 mEq/L to 9.69 mEq/L, our potassium level was lower than the other cases (7.8 mEq/L)
The mechanism of neuromuscular damage is probably due to abnormal depolarization of the nerve membrane secondary to changes in the potassium gradient and the membrane action potential at rest. Sodium channels can be inactivated by this prolonged depolarization, resulting in reduced excitability of the membrane which manifests as muscle weakness or paralysis. These symptoms can manifest in the heart and / or skeletal muscles.
Conclusion
Hyperkalaemia is a rare cause of flaccid paralysis, its diagnosis should be sought before any paraparesis or non-traumatic quadriplegia. Failure to recognize this leads to an exhaustive assessment of neurological disease which can delay the management of hyperkalaemia. A strong index of suspicion should be the key to early diagnosis in any patient presenting to the emergency room with features of acute flaccid quadriparesia especially in kidney failure . Hyperkalemia may be a potentially life-threatening but rapidly reversible cause of quadriparesis. These observations remain rare but must be known by the clinician in emergency service.
Declarations
Conflicts of Interest: The authors declare that they have no conflicts of interest.
Authors’ Contributions: Ghislain EDJO NKILLY conceived the presented idea and wrote the manuscript with input and critical feedback from all authors.
Raphael OKOUE ONDO helped to revise the manuscript.
Stéphane OLIVEIRA helped to write the manuscript and followed the patients in the postoperative period.
Jean fidel NNANG ESSONE helped to acquire the data.
Jean Marcel MANDJI-LAWSON helped to write the manuscript.
Romain TCHOUA helped to revise the manuscript.
References
- Aboubacar Conté, Bernard Sawadogo, Nouaou Gbamou, Mariane Kouawo, Pauline Yanogo, et al. Epidemiological profile of acute flaccid paralysis (AFP) from 2009 to 2018 in Guinea. Journal of Interventional Epidemiology and Public Health. 2021; 4:7.
- ALLIEZ Jean Roch, BALAN Corneliu, DIALLO Oumar, ALLIEZ Bernard. Pott’s disease and Pott’s paraplegia. African Journal of Neurological Sciences. 2006; 25.
- Hima-Maiga A, Kelani A, Abdoulwahab I, Diop A, Sanoussi S, et al. Paraplegia associated to an intradural extra medullary tuberculoma in Niamey: A case report. Health Sci Dis. 2020; 21: 109-112.
- Kamel KS Wei C. Controversial issues in the treatment of hyperkalaemia. Nephrol Dial Transplant. 2003; 18: 2215-2218.
- Panichpisal K, Gandhi S, Nugent K, Anziska Y. Acute quadriplegia from hyperkalemia: a case report and literature review. Neurologist. 2010; 16: 390-393.
- Christian T. Braun, David S. Srivastava, Bianca Maria Engelhardt, Gregor Lindner, Aristomenis K. Exadaktylos. LazyLips: Hyperkalemia and Acute Tetraparesis-A Case Report from an Urban Emergency Department. Case Rep Emerg Med. 2014; 160396.
- Lauren A. Kimmons, Justin B. Acute Ascending Muscle Weakness Secondary to Medication-Induced Hyperkalemia. Usery Case Rep Med. 2014; 789529.
- Sanson G, Russo S, Iudicello A, Schiraldi F. Tetraparesis and failure of pacemaker capture induced by severe hyperkalemia: case report and systematic review of available literature. J Emerg Med. 2015; 48: 555-561.
- Paras Karmacharya, Dilli Ram Poudel, Ranjan Pathak, Andrew Rettew, Richard Alweis. Acute hyperkalemia leading to flaccid paralysis: a review of hyperkalemic manifestations. J Community Hosp Intern Med Perspect. 2015; 5.
- Suneel Kumar Garg, Sanjay Saxena, Deven Juneja, Omender Singh, Mukesh Kumar,Joy Dev Mukherji.Hyperkalemia: A rare cause of acute flaccid quadriparesis. Indian J Crit Care Med. 2014; 18: 46-48.
- Desport E, Leroy J, Nanadoumgar H, Chatellier D, Robert R. An unusual diagnostic of quadriparesia: Hyperkalemic paralysis. Report of four non-familial cases. Rev Med Interne. 2006; 27: 148-151.
