
Open Access, Volume 9
Surgical management of a spectacular bilateral genu valgum in renal osteodystrophy: A case report
Khaled Kamoun*; Samih Daoudi; Wajdi Arfa; Hassene Affes; Mourad Jenzri
Pediatric Orthopedic Department, Kassab Orthopedic Institute, El Manar Medical School, Tunis, Tunisia.
Khaled Kamoun
Pediatric Orthopedic Department, Kassab Orthopedic Institute, El Manar Medical School, Tunis, Tunisia.
Email: kamounkhaledanis@gmail.com
Received : March 01, 2023,
Accepted : April 07, 2023
Published : April 10, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Genu-Valgum is a common and usually benign condition, but some severe deformities are still challenging for orthopaedic surgeon. We report a case of a 27 years- old woman with neglected severe bilateral genu-valgum and a medical history of renal failure since the age of nine. Clinical exam shows a spectacular deformity with unusual crossing legs for stable standing. Patient complains from limping with scissor gait and knee instability. Both femoral and tibial osteotomy was performed and allowed a good correction improving functional outcome at follow up.
Keywords: Genu-valgum; Chronic kidney disease; Osteotomy.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kamoun K (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kamoun K, Daoudi S, Arfa W, Affes H, Jenzri M. Surgical Management of a Spectacular Bilateral Genu Valgum in Renal Osteodystrophy: A Case Report. Open J Clin Med Case Rep. 2023; 2014.
Introduction
Growth disturbances and angular knee deformities are among skeletal abnormalities related to renal osteodystrophy (ROD). Although improved by medical treatment, some severe cases are still challenging for orthopaedic surgeons even if surgical correction was indicated. In our case, we report a management of a spectacular bilateral genu-valgum.
Case Presentation
A 27-year-old woman presented to our department with severe bilateral genu valgum (Figure 1). The patient had been suffering from kidney failure since the age of nine and able to walk with a scissor gait. The knee’s range of motion was quite normal with a mild lack of extension (extension/ flexion: 10/120°of the right and left knee). Physical examination noted a slack medial collateral ligaments, dislocated patellae with no evidence of torsional tibial or femur abnormalities.
Lower limb x-ray showed the importance of femoro-tibial angle (FTA: Right limb 48°/ Left 56°), bilateral lateral femoral condyle and tibial plateau hypoplasia (Figure 2). This case was classified as a sever deformity according to the Keblish classification.
We performed a combined medial closing wedge osteotomy on the distal femur and the proximal tibia since the deformity interested both segments. Due to our experience with children, we decided to stabilise osteotomies with cross K-wires associating an above knee cast for two months (Figure 3).
Six months following surgery, patient seems very satisfied, walking with no limping, with a full range of knee motion (0/130°). Clinical correction was confirmed by plan lower limb x- ray showing a neutral mechanical axis and completely healed osteotomies (Figure 4).

Figure 1: Clinical aspect with unusual crossing leg stabilizing severe deformity.

Figure 2: Long-leg standing weight-bearing x-ray.
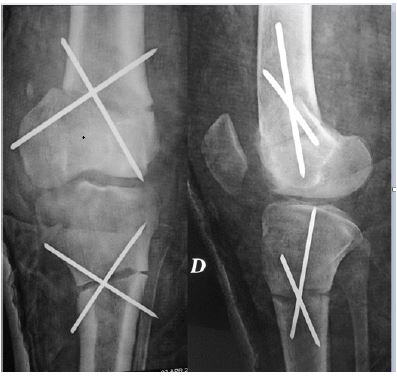
Figure 3: Post-operative x-ray with immediate correction and kwire stabilization.

Figure 4: Clinical and radiological results at the last follow-up with correction of limb mecanic axes.
Discussion
Genu-valgum is usually a benign condition at the age of 3-5 years when parents become concerned about the knocked knee appearence. Intermalleolar distance, between the medial malleoli in a standing patient, is still used to assess the degree of the deformity. An intermalleolar distance greater than 8 cm is considered pathologic [1]. These clinical criteria may correspond to a tibiofemoral angle greater than 10° [2].
Knee valgum has several aetiologies [2,3]. It can be bilateral (physiologic, skeletal dysplasias, metabolic bone diseases, lysosomal storage disease) or unilateral (post-traumatic, bone infection). Our patient had a renal osteodystrophy (ROD), a skeletal disorder complicating end-stage renal failure.
Secondary hyperparathyroidism, osteomalacia and aluminum intoxication due to kidney failure, can generate growth disturbance affecting physeal maturation in infancy. These growth disorders involves all skeleteal physis and generate various osteo-articular deformities such as genu valgum and varum, slipped capital femoral epiphysis, ankle valgum and varum, coxa vara, long-bone bowing, scoliosis….[4].
In addition, biomechanical factors could worsen these deformities. Based on the Hueter -Volkmann principle, some authors explain the genu-valgum by asymmetric weight distribution due to the physiologic knock-knee in early childhood [4].
This abnormal weight balance suppresses physeal maturation in overloaded knee compartments. Biomechanical factors associating to growth disturbance related to ROD can explain this spectacular genu-valgum in our case [4].
Typically, the genu-valgum results from bony and soft-tissue changes around the knee. The distal femur is frequently the most common site, but this deformity can arise from the proximal tibia as well [5].
Beside the aesthetic problem, osteoarthritis remains one of the most frequent complications [5]. Our patient was extremely annoyed from the physical appearance.
The preoperative planning should involve a long-leg standing weight-bearing x ray, 45-degree flexion anterioposterior views of both knees and lateral knee radiographs. These radiographies are sufficient to appreciate tibial and femoral mechanical axes, patellar height, and the joint line inclination [6].
Surgical correction of such deformity is based on lateral opening or medial closing wedge osteotomies around the knee (distal femur and proximal tibia) [6,8] proceeding by the site deformity location. Femoral osteotomies correct deformity in extension alone, since it has no accent on the posterior condyles. As for the tibia osteotomies, the deformity is corrected in both extension and flexion.
Our patient had bilateral knee valgum (56° on the left side and 48° on the right side) involving both femur and tibia. We performed both tibia and femoral closed wedging osteotomies stabilized by cross K-wires and above knee cast with a good healing at 3 month follow up.
To prevent sciatic nerve damage, we performed double closed wedge osteotomies instead of an opening one and cast was performed in 30° of flexion.
Crossed K-wires with cast were preferred to other stabilized device: locked plate, External fixators…. [3,5,7], to reduce time procedure (four osteotomies) and to prevent from complications. Patients with immunocompetence deficit and poor bone stock are known to have higher risk of wound infection and bone non-union.
To prevent these osteo-articular disturbances, some authors recommended early treatment of secondary hyperparathyroidism with bracing in early deformities or guided surgical growth’s technique [9].
Conclusion
Surgical treatment of knee deformities related to ROD is challenging. Bone growth disturbance associated to biomechanical factors can lead to severe deformities mainly when neglected. Surgical management remains possible in adult but preferable to be performed in childhood to optimize outcome and prevent from early osteoarthritis.
Conflict of interest: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
- Patel, Madhish. and Ryan Nelson. “Genu Valgum.” StatPearls, StatPearls Publishing, 2020.
- Lange J, Haas SB. Correcting severe valgus deformity: taking out the knock.” The bone& joint journal. 2017; 99: 60-64.
- Espandar, Ramin et al. Angular deformities of the lower limb in children. Asian journal of sports medicine. 2010;1: 46-53.
- Hruska, K. Pathophysiology of renal osteodystrophy. Pediatr Nephrol. 2000; 14: 636-640.
- Hisateru Niki, Haruhito Aoki, Takaaki Hirano, Moroe Beppu. Severe genu valgum deformity and slipped capital femoral epiphysis with renal osteodystrophy: a report of two cases.Journal of Orthopaedic Science. 2012; 4: 500-506.
- Brouwer GM, van Tol AW, Bergink AP, Belo JN, Bernsen RMD, et al. Association between valgus and varus alignment and the development and progression of radiographic osteoarthritis of the knee. Arthritis and rheumatism. 2007; 4: 1204-1211.
- Simone C, Lustig S, Servien E, Batailler C, Neyret P, et al. “Correction of Tibial Valgus Deformity.” J Knee Surg. 2017; 30: 421-425.
- Heerwaarden RV, Brinkman JM, Pronk Y. “Correction of Femoral Valgus Deformity.” J Knee Surg. 2017; 30: 746-755.
- Gigante C, Borgo A, Corradin M. Correction oflower limb deformities in children with renal osteodystrophy by guided growth technique. J Child Orthop. 2017; 11: 79-84.
