
Open Access, Volume 9
A case of acute bacterial meningitis presenting with
cerebellar infarct
Sanjeev Kumar Singla
Department of Anaesthesiology and Intensive Care, Adesh Institute of Medical Sciences and Research Bhatinda, Punjab, India.
Email: drsanjeevsingla77@rediffmail.com
Received : February 15, 2023,
Accepted : March 30, 2023
Published : April 05, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Acute meningitis is a fatal infection of the central nervous system and may be associated with complications like cerebral infarcts, but Cerebellar infarcts are rare. We are presenting a 50 year female presented to emergency due to fever, altered sensorium and vomiting. Contrast MRI Brain revealed acute infarct in left middle cerebellar peduncle and left cerebellar hemisphere, periventricular ooze and leptomeningeal enhancement on post contrast FLAIR. Cerebrospinal fluid was suggestive of acute bacterial meningitis, the source of which could be middle ear infection by Methicillin Resistance Stapylococcus Aureous (MRSA). Patient required transient mechanical ventilation. She was managed with intravenous antibiotic, Dexamethasone and other supportive treatment. The patient was discharged on day 15 in a stable condition and Glassgow coma score of 15. Acute Bacterial meningitis and its complications can be fatal if not managed timely. The vasculitis cerebral hemispheres has been known complication. The cerebellar infarcts purely are rare.
Keywords: Acute bacterial Meningitis; Cerebellum; Ischemic infarct.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Singla SK (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Singla SK. A case of acute bacterial meningitis presenting with cerebellar infarct. Open J Clin Med Case Rep. 2023; 2006.
Introduction
Acute Bacterial meningitis is a lethal infection of the central nervous system. The annual incidence of which in adults is 4–6 cases per 100,000. The most common causative agents include Streptococcus pneumoniae, Neisseria meningitides and Haemophilus influenzae. With best of medical care, this has high mortality rate (10-40%) and neurological deficits are seen in 30–52% of survivors [1,2]. The complications of acute pyogenic bacterial meningitis include cerebral ischemic or hemorrhagic infarcts and sinus thrombosis [3]. We after taking written and informed consent are presenting a case of acute pyogenic bacterial meningitis associated with cerebellar infarct.
Case Presentation
A 50 year female known case of Diabetes Mellitus since 5 years not on any medication presented in emergency with history of fever, altered sensorium and vomiting since one day. She was shifted to ICU. Her Glasgow coma score was 8 (E2V1M5), blood pressure of 130/70 mmHg, heart rate of 110/min and respiratory rate of 24/min. Both pupils were equal in size and normal reaction to light and nuchal rigidity was present. She was intubated due to poor GCS and put on mechanical ventilation. Contrast MRI Brain revealed acute infarct in left middle cerebellar peduncle and left cerebellar hemisphere, periventricular ooze and leptomeningeal enhancement on post contrast FLAIR (Figure 1). Her blood investigations were normal except for leukocytes count of 17500 cells/μL, random blood sugar of 396 and procalcitonin 2.3. Lumbar puncture was done. Cerebrospinal Fluid was turbid yellow and showed protein 274 mg/dl, glucose 23 mg/dl(corresponding blood sugar was 382 mg %) and a total leucocyte count of 280/mm3 (neutrophills - 70%, Lymphocytes – 2%), no organism on gram ZN, Gram staining and KOH prepration. The CSF was also negative for gene expert for Tuberculosis, Polymerase chain reaction for herpes and cryptococcal antigen. She was treated with Monocef and vancomycin after Intravenous dexamethasone, Insulin infusion, intravenous fluids and other supportive treatment. Ear discharge was noted and sent for culture sensitivity. The culture after 24 hours revealed growth of gram-positive organism which later on confirmed to be methicillin resistant Staphylococcus Aureus (MRSA) sensitive to vancomycin. She responded to treatment with normalization of leucocytes and improved her GCS. On day 4, she was conscious oriented to time place and person, weaned from the ventilator and extubated. On day 9th, she was shifted in ward. After 2 weeks of intravenous antibiotlc therapy, she was discharged in stable condition on day 15th.
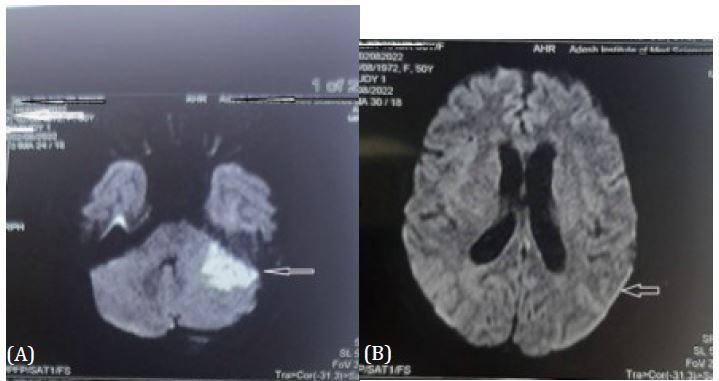
Figure 1: (A) MRI image Upper arrow showing left cerebellar infarct.
(B) Lower arrow showing leptomeningeal enhancement.
(B) Lower arrow showing leptomeningeal enhancement.
Discussion
Acute bacterial meningitis and its complications are fatal if left untreated. In this case the short history and CSF picture was suggestive of acute bacterial meningitis. The vasculitis is reported previously presenting as cerebral infarcts and sinus thrombosis [3]. Staphylococcus aureus infection as a risk factor for vasculitis has been reported previously [4], but pneumococcus is more commonly associated with this [5]. The hemorrhagic complication of cerebellum has been reported by Bodilsen, et al. [3] We noted left ear discharge, so planned for CSF analysis as middle ear infections are known cause of meningitis.
The MRI was done because of altered sensorium and to rule out any features of raised intracranial pressure, as lumbar puncture was to be done for CSF analysis. The MRI was suggestive of left cerebellar infarct with hemorrhagic conversion due to vasculitis and leptomeningeal enhancement on bilateral cerebral hemispheres. CSF revealed acute bacterial meningitis.
The acute bacterial meningitis leading to vasculitis and cerebellar infarct with hemorrhagic conversion. Since the cerebral circulation did not revealed any abnormality and her blood pressure was within normal limits there are less chance of hypertensive bleed and location of lesion was suggestive of primarily ischemic. Local depletion of coagulation factors, which together with microvascular damage, vasculitis and cerebral infarction, might lead to the observed manifest cerebral hemorrhages [6].
Conclusions
Acute Bacterial meningitis and its complications can be fatal if not managed timely. The vasculitis cerebral hemispheres have been known complication. The cereberllar infarcts are rare and has not been reported in literature.
Financial support: Nil.
Conflict of interest: None.
References
- Sigurdardottir B, Bjornsson OM, Jonsdottir KE, Erlendsdottir H, Gudmundsson S. Acute bacterial meningitis in adults. A 20-year overview. Arch Intern Med. 1997; 157: 425-430.
- Hussein AS, Shafran SD. Acute bacterial meningitis in adults. A 12-year review. Medicine (Baltimore). 2000; 79: 360-368.
- Bodilsen J, Dalager-Pedersen M, Schonheyder HC, Nielsen H. Stroke in community-acquired bacterial meningitis: a Danish population-based study.
- Int J Infect Dis. 2014; 20: 18-22.
- Bentley P, Qadri F, Wild EJ, Hirsch NP, Howard RS. Vasculitic Presentation of Staphylococcal Meningitis. Arch Neurol. 2007; 64: 1788-1789.
- Mook-Kanamori BB, Fritz D, Brouwer MC, van der Ende A, van de Beek D. Intracerebral hemorrhages in adults with community associated bacterial meningitis in adults: Should we reconsider anticoagulant therapy? PLoS One. 2012; 7: e45271.
- Vergouwen MD, Schut ES, Troost D, van de Beek D. Diffuse cerebral intravascular coagulation and cerebral infarction in pneumococcal meningitis. Neurocrit Care. 2010; 13: 217-227.
