
Open Access, Volume 9
Bilateral osteochondrosis of the distal tibial epiphysis: An extremely rare condition: Case report with literature review
Mohamed Chaabouni1*; Khaled Anis Kamoun2; Emna Labbène1; Hend Riahi1; Mouna Chelli Bouaziz1
1Department of Radiology, M.T. Kassab Institute of Orthopedics, Ksar Said, Tunisia.
2Department of Pediatric Orthopedics, M.T. Kassab Institute of Orthopedics, Ksar Said, Tunisia.
Mohamed Chaabouni
Department of Radiology, M.T. Kassab Institute of Orthopedics, Ksar Said, Tunisia.
Email: dr.chaabounimed@gmail.com
Received : February 07, 2023,
Accepted : March 07, 2023
Published : March 10, 2023,
Archived : www.jclinmedcasereports.com
Abstract
Osteochondrosis is a developmental disease characterized by an abnormal endochondral ossification of the epiphyses or epiphyseal equivalents (round bones and apophyses). Distal tibial epiphysis is an uncommon location of this condition and bilateral involvement is extremely rare. Only two cases are known in the literature. The aim of this paper is to report the third case of bilateral distal tibial epiphysis osteochondrosis, to discuss its etiology, and to revise its clinical presentation, imaging features, and treatment.
Keywords: Bone diseases; Developmental; Osteochondrosis; Tibia; epiphyses; Imaging.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Chaabouni M (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Chaabouni M, Kamoun KA, Labbène E, Riahi H, Chelli Bouaziz M. Bilateral osteochondrosis of the distal tibial epiphysis: An extremely rare condition: Case report with literature review. Open J Clin Med Case Rep. 2023; 1993.
Introduction
Siffert and Arkin described the first case of distal tibial osteochondrosis in 1950 [1]. Since then, nine other cases were reported. The pathophysiology of this rare condition is still debated and is likely multifactorial. The clinical presentation is not specific but imaging findings are characteristic and worth to be known. Magnetic Resonance Imaging (MRI) represents the key tool for diagnosis. This condition has generally a good prognosis under conservative treatment. We herein report the case of osteochondrosis of the distal tibial epiphysis with bilateral involvement in a 13-year-old boy and review the literature on this disease.
Case Report
A 13-year-old boy was referred to the pediatric orthopedics department of our hospital with progressive pain in his right ankle over the past eight months. He did not recall any history of trauma to his ankle and had no medical history. He had no intensive sports training. On physical examination, he was overweight with a BMI of 27 Kg/m2. The right ankle was swollen, with normocoloured skin and without local heat. Its active and passive mobilization was painful with decreased mobility range. Neither foot deformity nor limb length discrepancy were noted. Blood tests were negative and an inflammatory or infectious etiology was ruled out. Antero-posterior radiographs of both ankles revealed a bilateral sclerotic and flattened median and lateral aspect of the distal tibial epiphyses predominantly on the right side (Figure 1).
An MRI of the right ankle was performed showing fragmentation of the distal tibial epiphysis with erosion and bone marrow edema of the epiphysis and adjacent metaphysis. A consequent osteochondral lesion of the talar dome was also noted (Figure 2).
The diagnosis of bilateral osteochondrosis of the distal epiphysis of the tibia was made and the patient was put under symptomatic treatment with restriction of podal support and temporary prohibition of sport activities. Within two months of follow-up, the patient reported a marked relief of pain and the clinical examination found a reduction of the swelling and a normal range of mobility of the right ankle.
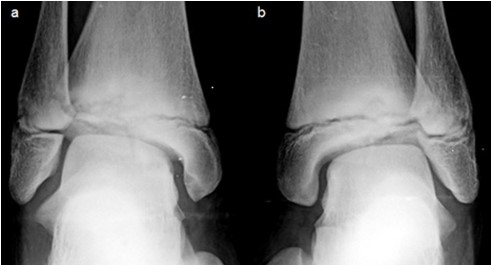
Figure 1: Antero-posterior ankle radiographs of the right (a) and left (b) ankle showing bilateral
flattening and sclerosis of the distal tibial epiphysis median and lateral aspect. Irregular narrowing of the distal physis is seen with sclerosis surrounding a lucency of the metaphyseal side
of the growth plate.
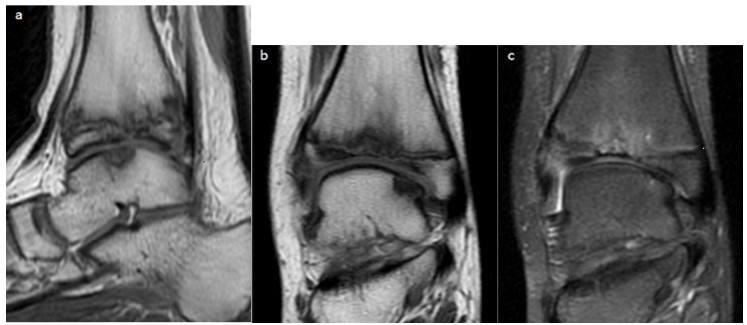
Figure 2: Sagittal T1 (a), coronal T1 (b) and coronal fat suppressed PD (c) weighted images of the right ankle show fragmentation of the tibial epiphysis and edema of the epiphysis and metaphysis. Note the consequent osteochondral lesion of
the talar dome.
Discussion
Osteochondrosis is a condition of unknown etiology that affects patients with an immature skeleton and is characterized by a breakdown of endochondral ossification. Different sites involving epiphyses or epiphyseal equivalents were listed, with similar clinical presentation and imaging features [2,3]. The most commonly affected epiphyses are the proximal capital femoral epiphysis and the second metatarsal head [4].
Osteochondrosis of the distal tibial epiphysis is a very uncommon location, with only ten cases reported since 1950 to the best of our knowledge [1,5-11]. Bilateral involvement of the distal tibial epiphysis is extremely rare with two case reports in 1993 [6] and 2015 [10].
Clinical presentation
This condition appeared within the second decade of life in all the reported cases.
Males are more often affected due to the constitutional delayed appearance of ossification centers in boys [12] and because of their greater susceptibility to childhood trauma and overuse injuries.
Clinical presentation and examination typically consist in a painful swollen ankle with decreased range of motion.
Imaging findings
Radiographs show epiphyseal flattening and sclerosis.
Three cases were explored with MRI [7-9], confirming epiphyseal irregularities and fragmentation with bone edema.
Etiology
The etiology of osteochondrosis of the distal tibial epiphysis is still debated in the literature and the exact mechanism of injury remains uncertain. Among the ten reported cases, two developed osteochondritis after ankle fracture [1,11]. A mild trauma without fracture or repetitive strain on the ankle was described in five cases [5-7,9].
Similar to a previous bilateral involvement case report [10], no history of trauma or sports injury was found in our observation.
Associated congenital abnormalities were also previously noted: A case of flexible Pes planovalgus of the same foot was reported [7]. Another case depicted a congenital sensitive neuropathy in the first patient and myelomeningocele and developmental dysplasia of the ipsilateral hip in the second patient [8].
Mechanical strain such as trauma and excessive overload may play a key role in the pathogenesis of osteochondrosis [13]. The ankle is the heaviest weight-bearing joint of the body, and excess of body weight, as seen in our observation, may overload this joint and predispose to an epiphyseal suffering.
The presence of bilateral lesions and the association of congenital conditions suggest the possibility of genetic cofactors in the pathogenesis of this condition.
Several hereditary, metabolic, and nutritional mechanisms were proposed to explain the pathogen esis of epiphyseal osteochondrosis [14].
Recent scientific investigations performed in the veterinary field put forward the hypothesis of an interruption of the blood supply to the epiphyseal cartilage. The epiphyseal growth cartilage is highly vascularized by cartilage canals that receive blood from the perichondrium or from the subchondral bone depending on the ossifying stage. Interruption of these blood supplies has been described as a triggering factor leading to the failure of endochondral ossification [15].
It is believed that the association of vascular, mechanical and constitutional anomalies contributes to the pathogenesis of distal tibia epiphysis Osteochondrosis.
Management and prognosis
Osteochondrosis of the distal tibial epipyhsis is a self-limited disease and is considered a benign condition.
The management generally consists of rest to avoid loading on the ankle joint along with analgesic medication.
The majority of the reported cases responded well and had a good prognosis with such conservative treatments.
Conclusion
This case report, alongside the previous ones, suggests that a child or an adolescent with persistent ankle pain without a specific injury should be investigated for osteochondrosis of the distal tibia. Characteristic imaging features include epiphyseal flattening and sclerosis on radiographs and fragmentation with bone marrow edema on MRI. Raising awareness towards this rare condition and the possibility of bilateral involvement will probably lead to improved diagnosis and better management.
Declarations
Funding: There is no funding source.
Conflict of interest: The authors declare that they have no conflict of interest.
Ethical approval: This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent: Informed consent was obtained from the relatives of the child included in the study.
References
- Siffert RS, Arkin AM. Post-traumatic aseptic necrosis of the distal tibial epiphysis; report of a case. J Bone Joint Surg Am. 1950; 32-A: 691-694.
- West EY, Jaramillo D. Imaging of osteochondrosis. Pediatr Radiol. 2019; 49: 1610-1616.
- Chelli Bouaziz M, Ladeb MF, Riahi H. Ostéochondroses de croissance. EMC (Elsevier Masson SAS, Paris) Radiodiagnostic-Squelette normal-Neuroradiologie-Appareil locomoteur. 2014 ; 31-190-B-10.
- Achar S, Yamanaka J. Apophysitis and Osteochondrosis: Common Causes of Pain in Growing Bones. Am Fam Physician. 2019; 99: 610-618.
- Robertson DE. Post-traumatic osteochondritis of the lower tibial epiphysis. J Bone Joint Surg Br. 1964; 46-B: 212-213.
- Holland CB, Thijn CJ, Visser JD. Bilateral osteochondrosis of the distal epiphysis. A case report. Rofo. 1993; 158: 171-172.
- Klein R, Burgkart R, Woertler K, Gradinger R, Vogt S. Osteochondrosis juvenilis of the medial malleolar epiphysis. J Bone Joint Surg Br. 2008; 90: 810-812.
- Gascó J, González-Herranz P, Minguez M-F, Gil-Albarova R. Avascular necrosis of distal tibial epiphysis: report of two cases. J Pediatr Orthop B. 2010; 19: 361-365.
- EL Hajj F, Sebaaly A, Kharrat K, Ghanem I. Osteochondritis of the distal tibial epiphysis. Case Rep Med. 2012; 2012: 629150.
- Turati M, Afonso D, Salazard B, Maillet Declerck M, Bigoni M, et al. Bilateral osteochondrosis of the distal tibial epiphysis: a case report. J Pediatr Orthop B. 2015; 24: 154-158.
- Kennedy JP, Weiner DS. Avascular necrosis complicating fracture of the distal tibial epiphysis. J Pediatr Orthop. 1991; 11: 234-237.
- Duthie RB, Houghton GR. Constitutional aspects of the osteochondroses. Clin Orthop Relat Res. 1981; 158: 19-27.
- Douglas G, Rang M. The role of trauma in the pathogenesis of the osteochondroses. Clin Orthop. 1981; 158: 28-32.
- Mobasheri A, Vannucci SJ, Bondy CA, Carter SD, Innes JF, Arteaga MF, et al. Glucose transport and metabolism in chondrocytes: a key to understanding chondrogenesis, skeletal development and cartilage degradation in osteoarthritis. Histol Histopathol. 2002; 17: 1239-1267.
- Olstad K, Ekman S, Carlson CS. An Update on the Pathogenesis of Osteochondrosis. Vet Pathol. 2015; 52: 785-802.
