
Open Access, Volume 9
Stress fracture of ipsilateral femoral neck after total knee replacement: 2 cases report
Changjie Liu1; Quanxiang Sun1; Daotong Fu1; Xiaoguang Liu2; Shiwei Liu2; Zezhong Liu2; Yimin Zhang2*
1Weifang Medical University, Weifang 261000, Shandong, China.
2Department of Joint Surgery, Weifang People’s Hospital, Weifang 261000, Shandong Province, China.
Yimin Zhang
Department of Joint Surgery, Weifang People’s Hospital, Weifang 261000, Shandong Province, China.
Email: ymzh69@hotmail.com
Received : December 12, 2022,
Accepted : January 16, 2023
Published : January 20, 2023,
Archived : www.jclinmedcasereports.com
Abstract
The main complications after total knee replacement were pain, infection, thrombosis and nerve injury, but few patients had ipsilateral femoral neck fractures, which might be related to changes of the biomechanical axis of the knee joint, increasing activity level, osteoporosis, and high BMI, following TKR.
Keywords: Total knee replacement; Femoral neck fracture; Biomechanical axis; Osteoporosis; BMI.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Zhang Y (2023)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Liu C, Sun Q, Fu D, Liu X, Liu S, et al. Stress fracture of ipsilateral femoral neck after total knee replacement: 2 cases report. Open J Clin Med Case Rep. 2023; 1968.
Introduction
Total Knee Replacement (TKR) was the definitive methods for severe knee osteoarthritis, which postoperative complications such as pain, infection, thrombosis and nerve injury were relatively common, while ipsilateral femoral neck fracture was rare. We reported 2 cases in this paper whose ipsilateral femoral necks were fractured after TKR. The causality was considered of relating to changes in biomechanical axis, increased activity level and high BMI, osteoporosis, et al.
Case Reports
Case 1
A female, aged 55, with 153 cm in height, 85 kg in weight and 36.3 in BMI. She was admitted to hospital on July 24, 2021 due to severe osteoarthritis of the right knee. Physical examination manifested severe varus deformity of affected limb with limited flexion and extension activities, with ROM: 80°-10°-0° (Figure 1). The patient received TKR on July 27, 2021. She was permitted walking one day post-operatively, and was discharged one week later (Figure 2).

Figure 1: Case 1

Figure 2: Case 1 after knee replacement
The patient came back again to the hospital 4 months following TKR, and complained of pain in her right hip for a month. Clinical examination and X-ray film: show the diagnosis of fracture of the right femoral neck, The patient denied any traumas (Figure 3).
Total hip replacement was performed for her and she was allowed to walked weight-bearing with the help of a walker, 1 week later she was discharged from the hospital (Figure 4).
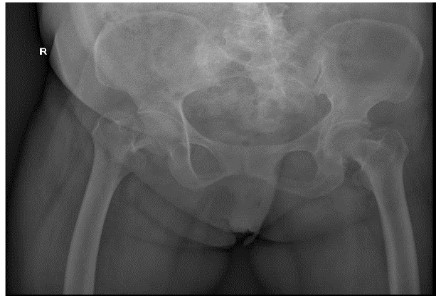
Figure 3: Case 1 fracture of the right femoral neck

Figure 4: Case 1 hip replacement
Table 1: Case 1 related blood test indicators after admission (osteoporosis indicators).
| Project | Result | Abnormal | Unit | Reference Range |
|---|---|---|---|---|
| β-CTx | 1097 | H | pg/ml | M 0-584 (30 to 50 years old), 0-704 (51 to 70 years old), 0-854 (71 years old) |
| F: Premenopausal: 0-573; Menopause: 0-1008 | ||||
| P1NP | 114.4 | H | ng/ml | M:15.13-58.59 |
| F: Premenopausal : L15.13-58.59: Menopause : 20.25-76.31 | ||||
| 25(OH)D | 7.13 | L | ng/ml | Deficiency<20; Inadequate 20-30; Adequate>30 |
| N-MID | 15.72 | ng/ml | Premenopausal: 11-43; Menopause; 13-48 |
Case 2
Case 2 was also a female with 58 in age, 160 cm in height, 65 kg in weight and 25.4 in BMI. She was admitted to hospital on December 08, 2020 due to severe osteoarthritis of the left knee. Physical examination manifested severe deformity of the affect limb with limited flexion and extension activities, with ROM: 100°-10°-0° (Figure 5).
TKR was implemented for her left knee under general anesthesia on December 08, 2020. And 1 day later after surgery, she began to walk with crutches (Figure 6). The patient was discharged 1 week post-operatively with satisfactory recovery.
The patient returned again nearly one year later, and complained of pain in her left hip for 20 days, especially during movement. Clinical examination and X-ray film; made the diagnosis of fracture of the left femoral neck. Also, the patient did not suffer any trauma (Figure 7).
FNS internal fixation was done for the fracture successfully. And she was permitted to sit in wheel-chair or stand on the unaffected leg within short period post-operatively (Figure 8).

Figure 5: Case 2 prior to admission

Figure 6: Case 2 after knee replacement
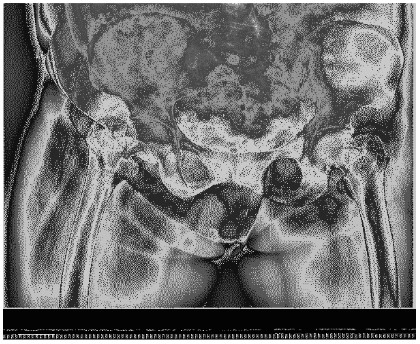
Figure 7: Case 2 fracture of the left femoral neck

Figure 8: Case 2 FNS internal fixation of femoral neck.
Table 2: Case 2 related blood test indicators after admission (osteoporosis indicators).
| Project | Result | Abnormal | Unit | Reference Range |
|---|---|---|---|---|
| β-CTX | 802.6 | PG/ml | M : 0-584 (30 to 50 years old), 0-704 (51 to 70 years old), 0-854 (>71 years old>) | |
| F : Premenopausal : 0-573; Menopause : 0-1008 | ||||
| P1NP | 82.14 | H | ng/ml | M : 15.13-58.59 |
| F : Premenopausal: 15.13-58.59; Menopause: `20.25-76.31 | ||||
| 25(OH)D | 23.4 | L | ng/ml | Deficiency < 20; Inadequate 20-30; Adequate; 30 |
| N-MID | 19.06 | ng/ml | Premenopausal: 11-43; Menopause: 13-48 |
Discussion
The common complications following TKR were pain, infection, thrombogenesis, nerve injury and so on, but stress fracture was rare. Only 22 cases have been described in English literature to date [1-10]. However, the incidence rate is on the increase with the popularity of TKR surgery.
Some researchers point out that the common risk factors of stress fracture of femoral neck after TKA are activity levels increased [1-10,12], osteoporosis [1,5-7,9,12], too much steroids [6], chronic rheumatoid arthritis, valgus deformity before knee replacement, changes in biomechanical axis of knee joint [4,8], and insertion of rotating hinge prosthesis [4,6,11].
In our cases, there were no over use of steroids, no long-term rheumatoid arthritis, no preoperative valgus deformity, and no use of rotary hinge implant. Bone mineral density was not measured in both patients.
As for the reasons, we deduced that post-operative changes in biomechanical axis of knee joint, increasing activity levels, osteoporosis and BMI mass index played great role in leading to stress fracture of femoral neck. Furthermore, the bilateral varus deformity of the knee joint was severe in these two patients, lower limb load axis after TKR is significant changed (Figures 1,2,5,6), resulting in concentrated creation on the femoral neck cortex. When full weight bearing, activity levels increased and excessive loading of the hip may cause the tendency of hip varus, bring about the possibility of fracture. Those two patients (Tables 1,2), Osteoporosis index 25 hydroxyvitamin D was lower than normal, they are osteoporosis, Bone density and mass decrease, and bone microstructure is destroyed, resulting in increased bone fragility, which can lead to fractures. The BMI of case 1 is 36.3, severe obesity, excessive loading of the right hip, so we assume that changes in biomechanical axis of knee joint after TKR, activity levels increased, osteoporosis and BMI mass index can lead this infrequent complication.
The interval between femoral neck fractures after TKR was 2 to 17 months, with an average of 8 months (4 and 12 months in our two cases, respectively). Amite Pankaj [11] proposed that early X-ray examination sometimes fails to detect femoral neck fracture, and safer MRI can provide earlier diagnosis. The early diagnosis is important, because it helps to the conservative treatment and avoid the shifting after the fracture, thus avoiding surgical treatment [2,8,10]. In our case, both patients experienced pain in the groin and presented to the doctor 1 month later. The patients did not pay much attention to these symptoms. Therefore, this complication should be highly suspected when ipsilateral hip pain occurs after TKR, especially in patients with poor mobility or obvious osteoporosis.
Joshi et al [8] point out that the increased stress in the femoral neck due to the change of hip biomechanical axis after the correction of valgus knee joint. However, in 26 cases (varus in our cases), only described valgus in 5 cases. Joshi et al [8] also point out that the design of total knee prosthesis to some extent has an effect on stress fracture of femoral neck, particularly in the hinged prostheses may change the kinematics of knee joint, results in the increased stress of tip and proximal of the femur prosthesis, which is sometimes easily overlooked.
In a word, patients with the knee deformity angle are large before replacement, severe osteoporosis and excessive load on the hips are higher risk of stress fracture of femoral neck after TKR. We should keep in mind this infrequent complication and prevent its occurrence. Among them, anti-osteoporosis is an effective method to avoid such complications.
Declarations
Ethics approval and consent to participate: This study was approved by the ethic committee of Medical Research Ethics Committee of Weifang People’s Hospital. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from the patients.
Consent for publication: Written informed consent was obtained from the patients.
Availability of data and materials: This published article contains all of the data generated and analyzed in this study.
Competing interests: The authors claim that they do not have competing interests.
Funding: This work was supported by (1) Natural Science Foundation of Shandong Province, China(Grant number:ZR2020MH094). (2) Scientific Research Project of Weifang Health and Family Planning Commission, No.WFWSJK-2020-034.
Authors’ contributions: CH.L was responsible for editing the main manuscript text, DT.F, ZZ.L and XR.S were responsible for writing the pictures, YM.Z and XG.L were mainly responsible for reviewing the manuscript, and all the authors participated in reviewing the manuscript.
Acknowledgements: The author, Changjie Liu feels grateful to the supports by his family during her study career.
References
- Lesniewski Pj TN. Stress fracture of the hip as a complication of total knee replacement. The Journal of bone and joint sur- gery.1982; 64: 304-306.
- Mc Elwaine Jp S J. Spontaneous fractures of the femoral neck after total replacement of the knee. The Journal of bone and joint surgery. 1982; 64: 323-325.
- Fipp G. Stress fractures of the femoral neck following total knee arthroplasty. The Journal of Arthroplasty. 1988; 3: 347-350.
- Hardy Dc, Delince Pe, Yasik E, Lafontaine MA. Stress fracture of the hip. An unusual complication of total knee arthroplasty. Clinical orthopaedics and related research.1992; 281: 140-4.
- Palanca Md, Albareda J, Seral F. Subcapital stress fracture of the femoral neck after total knee arthroplasty. International orthopaedics. 1994; 18: 308-309.
- Rawes M L, Patsalis T, Gregg PJ. Subcapital stress fractures of the hip complicating total knee replacement. Injury. 1995; 26: 421-423.
- Hendel D, Beloosesky Y, Weisbort M. Fracture of the hip after knee arthroplasty--an unusual case with pain in the knee. Acta Orthopaedica Scandinavica. 2009 ; 72: 194-195.
- Joshi N, Pidemunt G, Carrera L, Navarro-Quilis A. Stress Fracture of the Femoral Neck as a Complication of Total Knee Arthroplasty. The Journal of Arthroplasty. 2004; 20: 392-395.
- Hakan A, Nedim A M, Cuneyd G, Yavuz OY. Stress fracture of the femoral neck as a complication of revision arthroplasty of the knee: a case report. Acta orthopaedica Belgica. 2008; 74: 418-420.
- Sei M, Kenichi U, Yoshinobu M, Hashimoto N. Bilateral Stress Fractures of the Femoral Neck after Total Knee Arthroplasty: Importance of Early Diagnosis. Case reports in orthopedics. 2020; 2020: 3091693.
- Amite P, Rajesh M, Vivek L, Bhan S. Bilateral femoral neck stress fractures following total knee arthroplasty: a case report and review of literature. Archives of orthopaedic and trauma surgery. 2007; 127: 549-552.
- Cakmak S, Ogullari M, Kurklu M, Yıldız C. Bilateral femoral neck stress fracture following bilateral total knee arthroplasty: a case report. Acta orthopaedica et traumatologica turcica. 2012; 46: 312-315.
