
Open Access, Volume 8
All that glitters is not necrotizing fasciitis
Kallie E Wynens*; Luke Anders; Erin F Switzer; Andrew G Lawson; Elizabeth D Fox
Medical College of Georgia at Augusta University, Augusta, GA, USA.
Kallie E Wynens
Medical College of Georgia at Augusta University, Augusta, GA, USA.
Email: kwynens@augusta.edu
Received : Aug 25, 2022,
Accepted : September 21, 2022
Published : September 30, 2022,
Archived : www.jclinmedcasereports.com
Abstract
There are several mimics of necrotizing fasciitis, including post-traumatic subcutaneous emphysema. Here we present a case of a 17-year-old male who presented to the ED with diffuse crepitus after stabbing himself with a glitter pen in the posterior right calf. The patient was febrile, hypotensive, and ill appearing. Additionally, imaging several hours after injury revealed widespread subcutaneous emphysema. Considering these findings, he was taken to the OR for suspected necrotizing fasciitis. No evidence of infection was found. The patient recovered quickly and was discharged several days later. We hypothesize that the pen and musculature created a one-way valve mechanism which allowed air to enter but not exit the wound. Subcutaneous gas in the setting of injury is suggestive of necrotizing fasciitis, but non-infectious etiologies should also be considered.
Keywords: Post-traumatic; Imaging; Injury; Infection.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Wynens KE (2022)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Wynens KE, Anders L, Switzer EF, Lawson AG, Fox ED. All that glitters is not necrotizing fasciitis. Open J Clin Med Case Rep. 2022; 1910.
Introduction
Subcutaneous emphysema is the presence of air in subcutaneous tissues and can be the result of numerous etiologies. Non-infectious subcutaneous emphysema can have many causes including trauma, surgery, and perforation [1]. Compared to necrotizing soft tissue infections, pain is usually not out-of-proportion and not accompanied by warmth and erythema. Additionally, non-infectious etiologies usually present quicker and do not elevate inflammatory markers [2]. Here, we describe a case of diffuse subcutaneous emphysema associated with penetrating trauma to the right calf.
Our case involves a 17-year-old incarcerated male who presented to the ED 8 hours after stabbing his right posterior calf with a “glitter pen.” His only past medical condition was a well-controlled seizure disorder. Upon presentation, he was febrile (39.5 C), moderately tachycardic, hypotensive (90/50), ill appearing, with complaints of chest pain and shortness of breath. Physical exam revealed an approximately 1cm right calf puncture wound, calf tenderness, faint but non-spreading erythema in the area of the wound, and marked crepitus of the proximal right leg, abdomen, bilateral flanks, chest wall, and neck. Imaging revealed significant subcutaneous air involving these sites (Figure 1). White cell count, lactic acid, and CRP were all within normal limits. Broad spectrum antibiotics and aggressive volume resuscitation were initiated, and he was taken to the OR emergently out of concern for necrotizing soft tissue infection. In the OR, there was extensive gas within the muscles, but no purulent fluid, necrosis, or foul odor were present in three distinct sites explored.
Post-operative CT imaging demonstrated marked subcutaneous gas as well as a new moderate volume abdominal free fluid (Figure 1). On exam, the patient had a new complaint of abdominal tenderness. Considering this new finding in addition to free fluid, the patient was taken for exploratory laparotomy given the possibility of a retroperitoneal source of the subcutaneous gas. There was extensive retroperitoneal and omental emphysema without evidence of infection or necrosis. There was an additional finding of a moderate amount of simple-appearing as cites. After the operation, the patient spent 1 day in the ICU. Antibiotics were discontinued due to negative blood and wound cultures. He remained stable and without sign of infection and was discharged 3 days later.
It is important to consider infectious versus non-infectious pathology in the setting of crepitus. These two etiologies are difficult to distinguish. Necrotizing soft tissue infection alone can be a challenging diagnosis to make as it is a clinical diagnosis with minimal diagnostic tools and criteria [2]. However, delays in its diagnosis are associated with significantly increased mortality, which ranges from 6% to 76% when promptly diagnosed [2]. Furthermore, management of the different etiologies of crepitus differs greatly, with infectious origins necessitating immediate debridement and antibiotics, and non-infectious origins mostly allowing for conservative treatment.
Diffuse subcutaneous emphysema secondary to penetrating trauma is a rare clinical entity. Previous publications have hypothesized that air may be injected into the wound via the trauma; however, given the remarkable degree of subcutaneous air in this patient, we feel that this alone is unlikely to have caused this quantity of air [3]. In this case, we hypothesize that the glitter pen and musculature created a one-way valve mechanism, allowing air to enter but not exit the wound. The valve effect could be explained by muscle structure or wound edges forming a valve.3 The pumping effect provided by contracting muscles has been implicated in previous publications, although not to this extent [3,4].
Subcutaneous gas in the setting of infection or injury is suggestive of necrotizing soft tissue infection and should prompt aggressive antibiotic and possible surgical management for source control. However, in some circumstances, non-infectious traumatic wounds may create a one-way mechanism for introducing large volumes of air into soft tissues, mimicking more worrisome pathology.
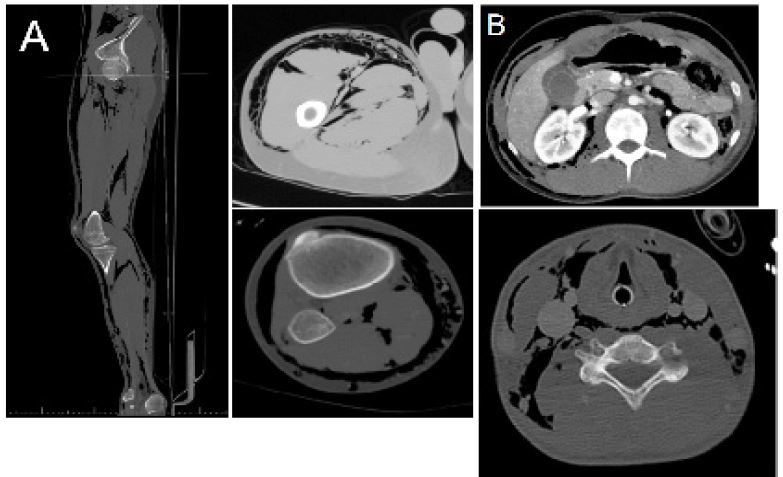
Figure 1: CT imaging of demonstrating subcutaneous emphysema. (A) CT of the right lower extremity, which, combined with the patient’s vitals were concerning for necrotizing fasciitis; however, exploration revealed no evidence of infection. (B) After the initial exploration, repeat imaging demonstrated new moderate-volume free fluid accompanied with new-onset abdominal tenderness, warranting a return to the operating room for exploratory laparotomy.
References
- Chaudhry AA, Baker KS, Gould ES, Gupta R. Necrotizing fasciitis and its mimics: what radiologists need to know. AJR Am J Roentgenol. 2015; 204: 128-139.
- Kamal RN, Paci GM, Born CT. Extensive subcutaneous emphysema resembling necrotizing fasciitis. Orthopedics. 2013; 36: 671-675.
- Filler RM, Griscom NT, Pappas A. Post-traumatic crepitation falsely suggesting gas gangrene. N Engl J Med. 1968; 278: 758-761.
- Jorgensen PS, Torholm C. Post-traumatic subcutaneous emphysema--misdiagnosed as gas gangrene. Ugeskr Laeger. 1990; 152: 2512-2513.
