
Open Access, Volume 11
Etiology and severity of traumatic spinal cord injury among patients admitted at KCMC from October 2020 to September 2023: A cross- sectional study
Tumaini Kinabo1*; Honest Massawe1; Peter Magembe2; Godlisten Kawiche3; Rogers Temu3
1Kilimanjaro Christian Medical University College, Kilimanjaro, Tanzania.
2Department of Orthopedics and Traumatology, Kilimanjaro Christian Medical Centre, Kilimanjaro, Tanzania.
3Mirembe National Mental Hospital, Dodoma, Tanzania.ssss
Tumaini Kinabo
Department of Orthopedic and Traumatology Surgery, PO Box 3010, Moshi, Tanzania.
Email: tumainikinabo@yahoo.com
Received : February 23, 2025,
Accepted : March 13, 2025
Published : March 28, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Background: Spinal cord injury is a devastating life changing injury with morbidity not only limited to physical aspect but also social, emotional and vocational life areas [2]. SCI may result from trauma (TSCI) or from degeneration of the spinal cord (non-traumatic SCI) [7].
Aim: To describe the etiology and severity of traumatic spinal cord injury among patients admitted at KCMC with traumatic spinal cord injury from October 2020 to September 2023.
Methodology: A descriptive cross-sectional study which was conducted at KCMC, Moshi Kilimanjaro which included all patients admitted at KCMC with TSCI. Data was collected from the hospital EHMS using a self- designed data collection tool. Patients with missing data were excluded. Sample size was 208 and a non- probability convenient sampling technique was used. Data was analyzed according to objectives using SPSS version 25 and presented using tables, charts and graphs.
Results: The study included 208 participants of whom 91.4% were male and 62.9% of participants were peasants. Median age for TSCI was found to be 36.0 (28.0-49.0) years. Most common etiology was found to be by fall 59.6%, and then followed by MTC 27.5%. The most injured spine segment was the cervical spine by 43.3%. Complete SCI (ASIA A) accounted for 64.4% of all TSCI.
Conclusion: TSCI remains a devastating life changing condition where most common cause falls and the most common injured segment is the cervical spine and most of the patients sustaining TSCI end up with complete SCI (ASIA A).
Abbreviations: ASIA: American Spinal Injury Association; EHMS: Electronic Health Management System; KCMC: Kilimanjaro Christian Medical Centre; KCMUCo: Kilimanjaro Christian Medical University College; MTC: Motor Traffic Crash; SCI: Spinal Cord Injury; TSCI: Traumatic Spinal Cord Injury.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kinabo T (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kinabo T, Massawe H, Magembe P, Kawiche G, Temu R. Etiology and severity of traumatic spinal cord injury among patients admitted at KCMC from October 2020 to September 2023: A cross-sectional study. Open J Clin Med Case Rep. 2025; 2334.
Introduction
Spinal cord is part of the central nervous system, acting as a major reflex center. It is a conduction pathway between body and brain. It is cylindrical in structure, protected by vertebrae and associated ligaments and muscles. In adults, the spinal cord is 42 to 45 cm long and it extends from the foramen magnum to the level of the L1 or L2 vertebra [15] (moore - Clinically oriented anatomy, 7th edition).
Spinal cord injury is an insult to the spinal cord leading to either permanent or temporary change in its neural and supportive function [12]. Spinal cord injury is the second most severe traumatic event after traumatic brain injury in terms of morbidity and disability. A study done at MOI by [10] shows that the burden of TSCI is 1.6 times higher in low to middle income countries than high income countries.
Spinal Cord Injury (SCI) can be caused by either traumatic injuries such as vertebral fractures or non-traumatic causes like infections and vascular damages [7]. TSCI may be grouped into two major groups, which are complete spinal cord injury (ASIA A) were there is complete loss of sensory and motor function and incomplete spinal cord injury were some of the motor or sensory functions are spared (ASIA B, C, D and E) [3].
| ASIA (American Spine Injury Association) impairment scale | ||
|---|---|---|
| A | Complete | No motor or sensory function is preserved below the neurological level and in the sacral segments S4–S5. |
| B | Incomplete | Sensory function preserved but motor function is not preserved below the neurological level and includes the sacral segments S4–S5. |
| C | Incomplete | Motor function is preserved below the neurological level, and more than half of key muscles below the neurological level have a muscle grade less than 3. |
| D | Incomplete | Motor function is preserved below the neurological level, and at least half of key muscles below the neurological level have a muscle grade of 3 or more. |
| E | Normal | Motor and sensory functions are normal. |
Methodology
Study design
Hospital based cross-sectional study from October 2020 to September 2023.
Study area
Kilimanjaro Christian Medical Center (KCMC). A zonal hospital found in northern east Tanzania with bed capacity of 630. It is found in Moshi municipality, Kilimanjaro region.
Study population and time
All patients with traumatic spinal cord injury admitted at KCMC hospital from October 2020 to September 2023.
Inclusion criteria: All patients with TSCI admitted at KCMC with TSCI from October 2020 to September 2023.
Exclusion criteria: Patients with incomplete data.
Sample size
Sample size was calculated using formula n= Z² P(1-P)/e²
• Where
- n = sample size required
- Z = statistical corresponding to 95% level of confidence (1.96)
P = prevalence (15.5%) [1]
- e = marginal error set at 5% (5)
• Minimum sample size = 201
Sampling technique
Non probability convenient sampling method.
Dependent variables
• Spine segment
• Severity of TSCI
Independent variables
• Age,
• sex,
• marital status
• Etiology of TSCI,
• Occupation,
• Residence
Data collection procedure
All patients with SCI who were admitted at KCMC from October 2020 to September 2023 were identified in the Electronic Hospital Management System (EHMS), by using International Classification of Diseases version 10(ICD 10) diagnosis codes. Diseases with codes T08 (fracture of spine), T09.3 (injury of spinal cord level unspecified), T91.3 (sequelae of injury of spinal cord), S24.1 (other and unspecified injury of thoracic spinal cord), S14.1 (other and unspecified injury of cervical spinal cord), G95.9 (disease of spinal cord unspecified), S32 (fracture of lumbar spine and pelvis), S22.1 (multiple fracture of thoracic spine) and S12.7 (multiple fracture of cervical spine). The disease code T91.3 (sequelae of injury of spinal cord) (n=752) was used as it contained all patients from all other disease codes. Patients with repeated data entry were identified, sorted and removed (n=428). Patients with non-traumatic SCI were identified and excluded from the study (n=73). Patient with incomplete data were also excluded from the study (n=43). Remained with 208 participants for the study. Data was collected from EHMS using a data collection tool. Starting from demographic data (sex, age, residence, occupation, marital status), then Etiology of TSCI (MTC, fall from height and others). Others in the etiology included Assaults (stab, blunt force trauma), weight falling on the head (load, wall, land slide or a tree falling on the head) and animal attacks. Segments involved in the TSCI (cervical spine, thoracic spine, lumbar spine, others (cervicothoracic or thoracolumbar)), and the severity of injury in the TSCI grouped as complete (ASIA A) and incomplete SCI (ASIA B, C, D or E).
Data analysis plan
Collected data was analyzed according to the objectives using SPSS version 25 for windows.
Numerical variables were analyzed by measure of central tendency with respective measure of dispersion. Categorical variables were analyzed by frequency and proportion.
Fisher’s exact test was used to test the relationship between etiology and severity of TSCI.
Logistic regression was performed to obtain crude and adjusted odds ratios for the association between severity of TSCI and etiology of TSCI.
The results were presented using tables, charts and graphs.
Ethical considerations
Permission to conduct this study was obtained from KCMUCo ethical committee and was given research ethical clearance certificate No: PG 58/2023.
Only Principal Investigator and Research Assistant shall have the access to the database.
Results
Characteristics of the study participants
This study included a total of 208 study participants. The median (IQR) age of the study participants was 36.0 (28.0-49.0) years. Majority of the study participants; 107(51.4%) were aged 21-40 years, 190(91.4%) were males, 136(65.4%) were married, 131(62.9%) were peasants, 127(61.1%) were residing in Kilimanjaro, 105(50.5%) were not using alcohol and 168(80.8%) were not smoking. This is well summarized on (Table 1).
Etiology leading to TSCI among patients admitted at KCMC from October 2020 to September 2023.
The etiological factors leading to TSCI among patients admitted at KCMC from October 2020 to September 2023 were Falling 124(59.6%) followed by motor traffic crash 57(27.5%) and other injuries 27(12.9%). NB: Others in the etiology included Assaults (stab, blunt force trauma), weight falling on the head (load, wall, land slide or a tree falling on the head) and animal attacks. This is shown on (Figure 1).
Spine segments associated with TSCI among patients admitted at KCMC from October 2020 to September 2023
Spine segments associated with TSCI among patients admitted at KCMC from October 2020 to September 2023 were as follows; cervical 90(43.3%), thoracic 70(33.6%), lumbar 32(15.4%), cervicothoracic 10(4.8%) and thoracolumbar 6(2.9%). This is shown on (Figure 2).
Table 1: Characteristics of the study participants (n=208).
| Characteristics | n (%) |
|---|---|
| Age (median IQR) (years) | 36.0 (28.0–49.0) |
| Age (years) | |
| ≤20 | 16 (7.7) |
| 21–40 | 107 (51.4) |
| 41–60 | 63 (30.3) |
| >60 | 22 (10.6) |
| Sex | |
| Male | 190 (91.4) |
| Female | 18 (8.6) |
| Marital status | |
| Not married | 72 (34.6) |
| Married | 136 (65.4) |
| Occupation | |
| Employed | 20 (9.6) |
| Self employed | 46 (22.1) |
| Peasants | 131 (62.9) |
| Students | 11 (5.3) |
| Residence | |
| Arusha | 60 (28.8) |
| Kilimanjaro | 127 (61.1) |
| Others | 21 (10.1) |
| Alcohol use | |
| No | 105 (50.5) |
| Yes | 103 (49.5) |
| Smoking | |
| No | 168 (80.8) |
| Yes | 40 (19.2) |
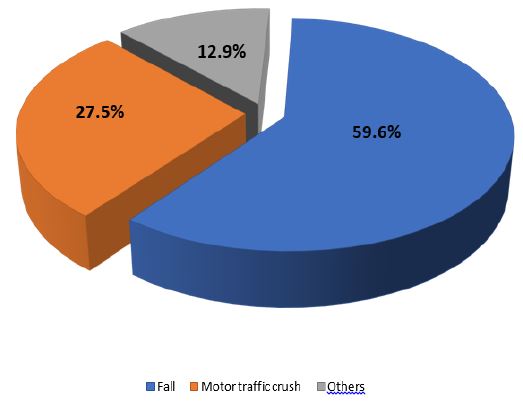
Figure 1: Etiological factors leading to TSCI (n=208).
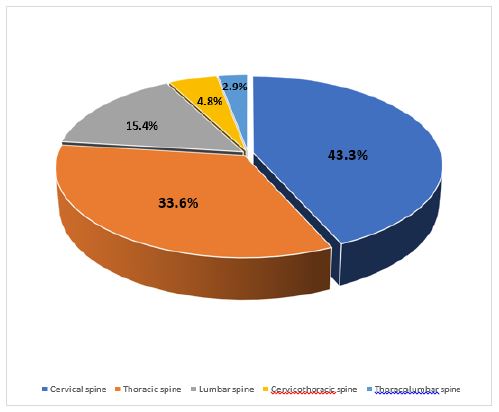
Figure 2: Spine segments associated with TSCI (n=208).
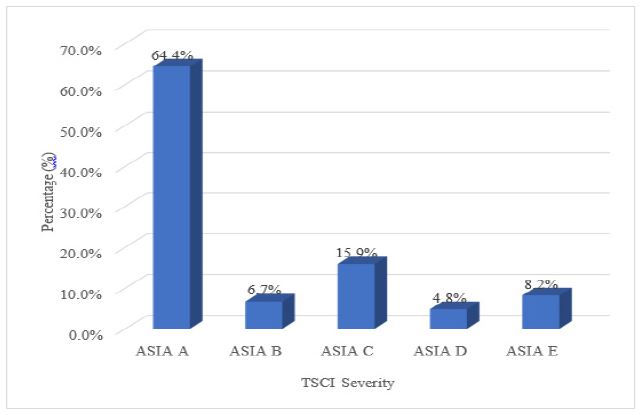
Figure 3: Severity of TSCI.
Severity of TSCI among patients admitted at KCMC from October 2020 to September 2023
The severity of TSCI among patients admitted at KCMC from October 2020 to September 2023 was as follows; ASIA A 127(63.2%), ASIA B 14(6.9%), ASIA C 33(16.5%), ASIA D 10(4.9%) and ASIA E 17(8.5%). This is shown on (Figure 3).
Discussion
The results of this study found that leading etiology of TSCI was falls (59.6%) and the most injured segment was cervical spine (43.3%). It also found that most of the participants (64.4%) with TSCI had a complete spinal cord injury (ASIA A).
Characteristics of study participants
The study included total of 208 participants aged from 10 years old to 93 years old. Majority of participants, 107(51.4%) were aged between 21 years to 40 years followed by 63(30.4%) participants aged between 41 years to 60 years. Total of 170(81.8%) participants are within the working age of the society. This shows that, TSCI significantly affects the working class of the society/community. This study also found that TSCI affects male 190(91.4%) more as compared to female 18(8.6%). This may be due to the activities which significantly puts a person at risk of getting TSCI are mostly done by men. This includes climbing trees to harvest fruits for business or home use, construction sites during roofing, mining activities, and motorcycle riders, etc. are mostly done by men. On occupation, this study found that peasants are mostly affected 131(62.9%). This may be secondary to low social economic status of peasants that they are the ones mostly paid by other classes of the society to do dangerous works which puts them at greater risk for getting TSCI. Most participants of this study were from Kilimanjaro, this may be due to the fact that the study area was KCMC, which is in Kilimanjaro and so it mostly provides services to people around Kilimanjaro.
Studies have been done which shows similar results to this study. A study done in Spain by [4], male was more affected with TSCI by 78.4% as compared to females 21.6%. same results were seen in a study done in Cameroon by [14], where males were affected more by 80% and females makes up 20% of patients with TSCI. Another study done in Tanzania by [13] found that males were more affected with TSCI by 85.6% as compared to females 14.4%. These results show that all over the world, males are affected with TSCI at much higher rate as compared to females because males are more involved in activities that are the greatest risk of acquiring TSCI as compared to females.
Etiology of TSCI
On the etiology of TSCI this study found that falls from heights were the leading cause of TSCI at 59.6% (most patients fell from avocado and mango trees), followed by motor traffic accidents at 27.5% and other causes accounted for 12.9%. This may be due to increasing demand of mangoes and avocadoes as a commercial fruits/product, which are abundant in Kilimanjaro and thus during their seasons many peasants are involved in climbing the trees for harvesting the fruits and thus end up falling and acquiring TSCI.
A study done in USA by [6] found different results from this study. The major cause of TSCI was motor traffic crash at 38.3% followed by falls at 25.3% and gunshot 10.4%. another study done in South Africa by [8] had different results as the major cause of TSCI was assault at 59.3%. One study done in Muhimbili Orthopedic Institute [9] found that the leading cause of TSCI was MTC (45%) followed by falls (32.8%). Another study done in northern Tanzania by [11] found similar results to this study where the most common cause of TSCI was falls 66.6% followed by road traffic accidents 28.7% and 4.6% were from other causes like assault, animal attacks, etc. These results showed that, the cause of TSCI is dependent of the environment. For the developing countries like Tanzania and in more rural areas the major cause of TSCI was falls as people works in risk environment and don’t have any protective gears while in more developed world or urban areas/cities the major cause of TSCI is MTC due to high use of motor vehicles. South Africa showed different results where major cause of TSCI was assault may be due to high rate of criminal activities in the country.
This study also found that a person who falls has equal chance of injuring either cervical spine or thoracic spine by 37.9% and lumbar spine by 16.1%. But when a person sustains a MTC is more likely to injure cervical spine by 49.1% followed by thoracic spine 35.1% and lumbar spine by 10.5%.
Spine segment associated with TSCI
Regarding spine segment associated with TSCI it was found that the most injured spine segment was cervical spine at 43.3% then followed by thoracic spine 33.6% and lumbar spine 15.4%. This may be due to the flexibility of the neck and its wide range of motion thus when an abrupt force is applied to it can easily be injured. One study done in Spain by [4] showed similar results to this study where the most injured spine segment was cervical 50.9% followed by thoracic spine 35.6% and lastly is lumbar 13.5%. another study done in Muhimbili Orthopedic Institute (MOI) [9] showed similar results were cervical spine (43.3%) was the most injured segment in TSCI. A study done in South Africa [2] showed different results where the most injured segment was thoracic spine 66.5% followed by cervical spine 20.8% and last was lumber 12.7%. This difference may be accounted to the fact that the most common cause of TSCI in this study from South Africa is assault. So may be direct blows to the spine during an assault is usually at the level of the thoracic spine.
Severity of TSCI
On the severity of spinal cord injury, it was found that most patients sustained a complete SCI (ASIA A) at 64.4% whereas combination of incomplete SCI (B, C, D, E) was 35.6%. Incomplete SCI was distributed as ASIA B at 6.7%, ASIA C 15.9%, ASIA D 4.8% and ASIA E 8.2%. A study done in South Africa by [2] showed a similar result to this study where complete SCI (ASIA A) accounted for 56.9% of all TSCI and incomplete SCI (ASIA B, C, D, E) accounted for 43.1%. Similar results were seen in a study done in USA [6] where complete SCI (ASIA A) was leading severity accounted for 43.6% of all injuries. These results shows that injury to the spinal cord predisposes a person to getting complete SCI (ASIA A) and this may be due to the delicacy of the spinal cord and complexity of the structures that encompasses the spinal cord.
Strength of the study: Study was conducted in a tertiary hospital where almost all the cases of TSCI from northern Tanzania are referred to KCMC. Also, KCMC has a special unit (Orthopedic Rehabilitation Unit (ORU)) specialized in rehabilitation of all SCI patients. This improved the strength of this study.
Limitations: This study was a retrospective study, all the patient’s assessment and grading depended on the documented data in the system. There was no assessment of the patient’s injury on day of injury. Also, some important patient information was missing from the EHMS.
Conclusion
TSCI remains a devastating life changing condition. Most of the patients sustaining a TSCI are caused by falls and most of the affected individuals acquire a complete SCI (ASIA A) which means that they lose their motor and sensory functions below the injury level. And most of the affected individuals with TSCI end up injuring the cervical spine.
Recommendations
This study found that the most common cause of TSCI was fall followed by MTC. People in our community should be educated on the devastating effect of falling from heights so as care should be taken and protective gears are used when engaging in activities that require climbing heights or when walking while carrying a load on the head.
More research should be done to elicit the effect of different heights in the TSCI. Thus, at what height we expect a person to sustain a severe form of TSCI. Further studies are needed to understand in details the social-economic and psychological impact of TSCI to individual suffering from TSCI.
Declarations
Conflict of interest: The author declared no conflict of interest.
Authors contribution: TK: He developed the research title, proposal writing, data collection and analysis as well as manuscript writing for publication. HM and RT were the main supervisors who oversaw this research work in every step. PM, GK, were consulted for their expert contributions in this research work.
Acknowledgement: I would like to start by thanking The All-Mighty God for giving me strength, good health and right support to complete my dissertation.
I would like to send my sincere gratitude to my supervisor, Dr Honest Massawe for his tireless efforts in making my research possible and tangible.
A lot of gratitude to all doctors (residents and specialists) in orthopedic department at KCMC for their support in improving my research writing. Their constructive inputs in development of this research have made a big difference.
I will also like to thank my parents, Doc. Leandri Kinabo and Mrs. Alberta Kinabo for their tireless support to the completion of this research. Without forgetting to thank my uncles, Nixon Matowo and Efatha Kitali and my aunt Leticia for their big support that made this research possible.
I will also like to send my sincere gratitude to my lovely wife, Gloria Maholo for her exquisite support and endless encouragement during development of this research.
References
- Adeolu AA, et al. Clinical outcome of closed reduction of cervical spine injuries in a cohort of Nigerians. Spinal Cord Series and Cases. 2019: 2–10.
- Alves MA, Pilusa S. The prevalence and pro fi le of spinal cord injury in public healthcare rehabilitation units in Gauteng, South Africa. 2023: 1–10.
- Apley A, Solomon L. Apley & Solomon’s System of Orthopaedics and Trauma. 2018.
- Bárbara-bataller E, et al. Change in the profile of traumatic spinal cord injury over 15 years in Spain. 2018: 1–8.
- Bullets O. ‘Trauma 2017’. 2017.
- Chen Y, et al. Causes of Spinal Cord Injury. 2013; 19: 1–8.
- Ding W, et al. Prevalence, and Disability from the Global Burden. 2022; 47: 1532-1540.
- Joseph C, et al. Incidence and aetiology of traumatic spinal cord injury in Cape Town, South Africa: A prospective, population-based study. Spinal Cord. 2015; 53: 692–696.
- Leidinger A, et al. Spinal trauma in Tanzania: Current management and outcomes. Journal of Neurosurgery: Spine. 2019; 31: 103–111.
- Magogo J, et al. Operative Treatment of Traumatic Spinal Injuries in Tanzania: Surgical Management, Neurologic Outcomes, and Time to Surgery. 2021; 11: 89–98.
- Moshi HI, et al. A one-year prospective study on the occurrence of traumatic spinal cord injury and clinical complications during hospitalisation in North-East Tanzania. 2021; 21: 788–794.
- Ngaiza WI, Olotu FI, Massawe HH. The patterns and management outcomes of traumatic thoracic and lumbar spinal cord injuries among patients admitted at Kilimanjaro christian medical centre from 2017 to 2018. Open Journal of Clinical and Medical Images. 2022; 2: 3–7.
- Rashid SM, et al. The characteristics of traumatic spinal cord injuries at a referral hospital in Northern Tanzania. Nature Publishing Group. 2017: 2–5.
- Shu PC, et al. ‘Thoracolumbar spine injury in Cameroon: etiology, management, and outcome. 2023: 1–9.
- Yusri AZ, dan D. Clinically Oriented Anatomy, 7th Edition. Jurnal Ilmu Pendidikan. 2020.
