
Open Access, Volume 11
Bilateral diaphragmatic paralysis in infant treated by diaphragm pacemaker implantation: Case report
Andriy Pereyaslov1,2*; Bohdan Malovanyy2; Olesya Nykyforuk1,2; Liliya Gyzha1
1Department of Pediatric Surgery, Danylo Halytskyy L’viv National Medical University, Ukraine.
2Surgery Clinic with the Centre of Mini-Invasive Surgery and Reconstructive Gastrointestinal Surgery, Communal Noncommercial Enterprise of L’viv Regional Council Clinical Centre of Children’s Healthcare, Ukraine.
Andriy Pereyaslov
Department of Pediatric Surgery, Danylo Halytskyy L’viv National Medical University, Fedkovycha str., 26/7, 79018 L’viv, Ukraine.
Tel: +38 050 5168092;
Email: andrew_perejaslov@yahoo.com
Received : February 13, 2025,
Accepted : March 07, 2025
Published : March 28, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Phrenic nerve injury is not frequent, but well recognized complication of birth trauma that caused uni- or bilateral paresis/paralysis of diaphragm. There are no generally accepted guidelines of treatment of this pathology in newborns.
We presented the first experience of thoracoscopic implantation of diaphragm pacemaker for the treatment of infant with bilateral diaphragmatic paralysis.
A male infant was born transvaginal at 37-38 weeks of gestation. Immediately after delivery, he developed severe asphyxia and required the ventilatory support. Diagnosis of Kofferath’s syndrome was established. Despite on intensive care, for 7 months child required the mechanical ventilation. With the aim to restore spontaneous breathing, the implantation of diaphragm pacemaker was performed initially at the right side and next at the left side. The effectiveness of the treatment was confirmed by the electroneuromyography and ultrasonography.
Implantation of the diaphragmatic pacemaker may be the method of treatment in infants with bilateral diaphragmatic paralysis.
Keywords: Infant; Bilateral diaphragmatic paralysis; Diaphragm pacemaker.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Pereyaslov A (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Pereyaslov A, Malovanyy B, Nykyforuk O, Gyzha L. Bilateral diaphragmatic paralysis in infant treated by diaphragm pacemaker implantation: Case report. Open J Clin Med Case Rep. 2025; 2332.
Introduction
Phrenic nerve injury is not frequent, but well recognized complication of birth trauma during vaginal delivery caused by cervical plexus injury that in some cases could associated with brachial plexus affect [1,2]. The phrenic nerve is the only one that supplies the motility of diaphragm; thus, its injury can result in paresis or paralysis of diaphragm, mainly unilateral, with the subsequent decreasing ventilatory capacity, bulging eventration, and respiratory insufficiency [3,4].
There are no guidelines on how to manage the newborns with diaphragmatic paresis/paralysis [5]. Most of these patients required the prolonged ventilatory support or surgery, in patients that cannot wean from mechanical ventilation [6]. In case of unilateral diaphragmatic paralysis, the main method of treatment is diaphragmatic plication [7]. However, in newborns with bilateral paralysis the diaphragmatic plication often didn’t improve the respiratory function and required prolonged mechanical ventilation [8].
We presented the first experience of thoracoscopic implantation of diaphragm pacemaker for the treatment of infant with bilateral diaphragmatic paralysis.
Case Report
A male infant weighting 2.750 g was born transvaginally at 37-38 weeks of gestation (11.09.2020). Immediately after delivery, he developed severe asphyxia, which caused by funicle entwine, and required the ventilatory support. Due to that, September 11, 2020, he was transferred to the intensive care unit of our clinical hospital.
At the time of admission, he exhibited prominent respiratory failure with paradoxical breathing. On admission, his vital signs were as follows: heart rate 132 bmp, systolic blood pressure 72 mmHg, respiratory rate 48 bmp, and oxygen saturation 68% on room air. He was intubated and mechanical ventilation was started with pressure synchronized intermittent mandatory ventilation regime: FiO2–40%, PEEP–15 mm H2O, rate – 26 bmp.
Right diaphragm was elevated on the level of III rib and left – on the level of V rib with the asynchronized movements on a fluoroscopic examination (12.09.2020).
Diagnosis of Kofferath’s syndrome (trauma of brachial plexus, spinal cord on the CIII-CV level) was established.
Except of mechanical ventilation patient received the symptomatic therapy directed to restoration of nervus phrenicus function: Cerebrocurium – 2 mg on time in 2 days, Agvantar – 200 mg/day, and Bendazolum – 1 mg/day.
On MRI (30.09.2020) was revealed the straightened cervical lordosis, bodies of the cervical vertebrae of a normal configuration with a preserved cortical layer.
Attempts to wean the infant from the respiratory support over two months were unsuccessful (prominent decrease of oxygen saturation up to 82%), due to that tracheostomy was performed (11.11.2020), and next 7 months child required mechanical ventilation through tracheostoma.
On May 27, 2021, the electroneuromyography was performed – M-answer from nervous phrenicus is unstable, with the sharply decreased of amplitude on the right side and moderate decrease on the left side. Conclusion: Ischemic cervical myelopathy with the partial effects of both nervous phrenicus (more prominent of the right side).
Considering, the bilateral character of affection, impossibility of spontaneous breathing, and damage of nerves phrenicus, it was decided to do not apply the diaphragmatic plication but implanted the Diaphragm Pacemaker (Avery Biomedical Devices, Inc. USA) (Figure 1). The informed consent of parents for the applying of such method of treatment was received
On June 20, 2021, under the thoracoscopic guidance separated the right nervus phrenicus with the fixation of the Diaphragm Pacemaker on it (Figure 2).

Figure 1: View of diaphragm pacemaker.
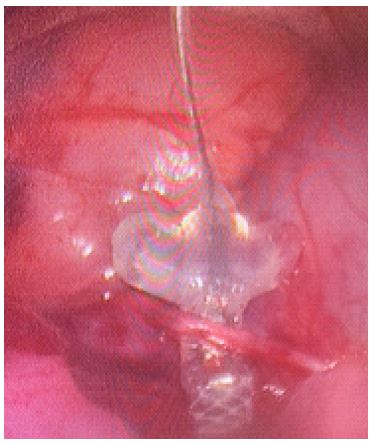
Figure 2: Thoracoscopy. Applying of pacemaker.
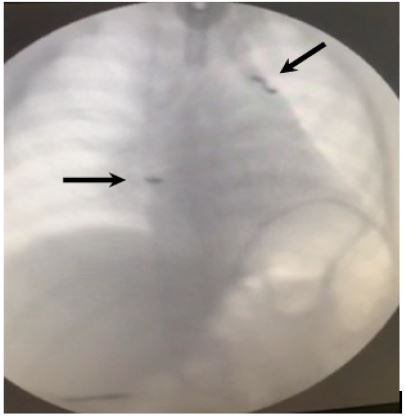
Figure 3: Postoperative chest radiograph. Pacemakers pointed by arrows.
On control electroneuromyography (June 26, 2021), the amplitude of the M-response on the right diaphragm increasing during the pacemaker functioning.
On July 14, 2021, the implantation of the Diaphragm Pacemaker on the left nervus phrenicus was performed.
After that, the spontaneous breathing restored without of need in respiratory support. The child was discharged from hospital on July 18, 2021.
On control electroneuromyography (August 9, 2021), the positive dynamic was noted on both sides.
On control ultrasonography (October 10, 2021), at M-mode the synchronous movements of the diaphragm and chest were noted.
For the present time, child breathing spontaneously (Figure 3), do not require respiratory support, and physically does not differ from peers.
Discussion
The diaphragm is the main inspiratory muscle that innervated by the right and left phrenic nerves, which are branches of the cervical plexus [5]. Paresis or paralysis of diaphragm, if is it not associated with the diaphragmatic hernia, is caused, in most newborns, by excessive cervical extension during delivery, occasionally combined with brachial plexus palsy, or cardiac surgery [2,9]. An incidence of phrenic nerve injury due to the birth trauma is 1 per 15,000-30,000 live births with estimated mortality of 10-15% [10-12]. In most cases, it was unilateral injury predominantly affecting the right side [13].
The diaphragm is an important inspiratory muscle in newborns, especially those born prematurely, and together with the intercostal muscles, it creates the force that ensures normal breathing in the child. Correspondingly, the paresis/paralysis one or both dome of diaphragm, the intercostal muscles must perform a dual function. Newborns has a relatively few fatigue-resistant type I fibers in respiratory muscles and due to that its endurance is limited [14]. Besides this, newborns spend more times in supine position that makes breathing especially difficult in case of paresis/paralysis of the diaphragm, and newborns intercostal muscles are the postural muscles, which inhibited during sleeping that its ability to compensate of diaphragmatic weakness is limited [14,15]. All of these determines the development of severe respiratory disturbances in a newborn with diaphragmatic paresis/paralysis.
Diaphragmatic paralysis presented as nonspecific respiratory disturbances with tachypnea, paradoxical breathing, cyanosis, and increased work of breathing [5,6,16] that consistent with our data.
Plain chest radiography/fluoroscopy and ultrasonography are the gold standard for confirmation of paresis/paralysis of diaphragm [5,17]. Diaphragmatic asymmetry is not present in bilateral diaphragmatic paralysis [9], however, in our case both hemidiaphragms were elevated with more prominent elevation on right side.
There are no guidelines for the management of newborns with continued respiratory distress caused by diaphragmatic paralysis [5,17]. There are few management options in case of diaphragmatic paresis/paralysis: 1) some authors advocated the waiting management tactic for 2-4 weeks due to the possibility of spontaneous recovery of phrenic nerve palsy [12,19]; 2) Initial supportive management includes intermittent positive pressure ventilation by nasal or oral mask, or mechanical ventilation in cases of severe respiratory distress [20,21], in case of prolonged ventilation, the ventilation through tracheostomy should be applied [9,22] with subsequent surgery, or 3) immediate diaphragmatic plication with the aim to reduce the need for mechanical ventilation, duration of hospital stay, and pulmonary infections [23,24].
The inability to wean from mechanical ventilation advised as indication for surgery [23,25]. The diaphragmatic plication via thoracoscopy or thoracostomy is the viable option in the surgical management of diaphragmatic paresis/paralysis independently of its etiology [8,9,11,23,24]. However, diaphragmatic plication is more effective in case of unilateral paralysis [23,24], and in case of bilateral paralysis its often required the prolonged oxygen therapy [8,11] or even consider as contraindication for plication [26].
Radecki and Tomatis firstly applied the eltctrophrenic pacing in an infant with diaphragmatic paralysin in 1976, however the child died at age 11½ month due to sepsis caused by confluent bronchpneumonia [27]. The recent experimental study of Kratz et al. confirmed that phrenic nerve seems to be the best location for direct stimulation by a unilateral thoracic diaphragm pacemaker [28]. In our case, the child resumed physical activity and did not require respiratory support for more than 36 months after pacemaker implantation.
Conclusion
Implantation of the diaphragmatic pacemaker may be the method of treatment in infants with bilateral diaphragmatic paralysis.
Declarations
Disclosure: This work was previously presented as a oral presentation at the 2023 on the 64th Annual Meeting of the Austrian Society of Surgery.
References
- K1. Reiter AJ, Rizeq YK, Many BT, Vacek JC, Abdullah F, Goldstein SD. A rare case of contralateral diaphragm paralysis following birth injury with brachial plexus palsy: A case report and review of the literature. Case Rep Pediatr. 2020; 2020: 8844029.
- Shiohama T, Fujii K, Hayashi M, Hishiki T, Suyama M, Mizuochi H, et al. Phrenic nerve palsy associated with birth trauma – case reports and a literature review. Brain Dev. 2013; 35: 363-366.
- Murty VSSY, Ram KD. Phrenic nerve palsy: a rare cause of respiratory distress in newborn. J Pediatr Neurosci. 2012; 7: 225-227.
- Garge SS, Passi GR, Ghanekar D. Early thoracoscopic plication of diaphragm in a newborn with brachial plexus palsy and concurrent phrenic nerve palsy. J Indian Assoc Pediatr Surg. 2017; 22: 165-167.
- Gerard‐Castaing N, Perrin T, Ohlmann C, Mainguy C, Coutier L, Buchs C, et al. Diaphragmatic paralysis in young children: A literature review. Pediatr Pulmonol. 2019; 54: 1367-1373.
- Rizeq YK, Many BT, Vacek JC, Reiter AJ, Raval MV, Abdullah F, et al. Diaphragmatic paralysis after phrenic nerve injury in newborns. J Pediatr Surg. 2020; 55: 240-244.
- Yongue C, Geraci TC, Chang SH. Management of diaphragm paralysis and eventration. Thorac Surg Clin. 2024; 34: 179-187.
- Van Smith C, Jacobs JP, Burke RP. Minimally invasive diaphragm plication in an infant. Ann Thorac Surg. 1998; 65: 842–844.
- Bhaskar P, Lone RA, Sallehuddin A, John J, Bhat AN, Rahmath MR. Bilateral diaphragmatic palsy after congenital heart surgery: management options. Cardiol Young. 2016; 26: 927-930.
- Stramrood CA, Blok CA, van der Zee DC, Gerards LJ. Neonatal phrenic nerve injury due to traumatic delivery. J Perinat Med. 2009; 37: 293-296.
- Shimizu M. Bilateral phrenic-nerve paralysis treated by thoracoscopic diaphragmatic plication in a neonate. Pediatr Surg Int. 2003; 19: 79-81.
- Yoshida K, Kawabata H. The prognostic value of concurrent phrenic nerve palsy in newborn babies with neonatal brachial plexus palsy. J Hand Surg Am 2015; 40: 1166 1169.
- Kraaijenga JV, Hutten GJ, de Jongh FH, van Kaam AH. Diagnosis of hemidiaphragmatic paresis in a preterm infant with transcutaneous electromyography: A case report. Neonatology 2015; 108: 38-41.
- Muller NL, Bryan AC. Chest wall mechanics and respiratory muscles in infants. Pediatr Clin North Am. 1979; 26: 503-516.
- Gibson GJ. Diaphragmatic paresis: pathophysiology, clinical features, and investigation. Thorax. 1989; 44: 960-970.
- Parker LA. Part 2: Birth trauma: injuries to the intraabdominal organs, peripheral nerves, and skeletal system. Adv Neonatal Care. 2006; 6: 7-14.
- Bowerson M, Nelson VS, Yang LJ. Diaphragmatic paralysis associated with neonatal brachial plexus palsy. Pediatr Neurol. 2010; 42: 234-236.
- Yoshida K, Kawabata H. The prognostic value of concurrent phrenic nerve palsy in newborn babies with neonatal brachial plexus palsy. J Hand Surg Am. 2015; 40: 1166-1169.
- Hoeksma AF, ter Steeg AM, Nelissen RG, Nelissen RG, van Ouwerkerk WJ, Lankhorst GJ, et al. Neurological recovery in obstetric brachial plexus injuries: an historical cohort study. Dev Med Child Neurol. 2004; 46: 76-83.
- Qureshi A. Diaphragm paralysis. Semin Respir Crit Care Med. 2009; 30: 315-320.
- Tokuda Y, Matsumoto M, Sugita T, Nishizawa J. Nasal mask bilevel positive airway pressure ventilation for diaphragmatic paralysis after pediatric open-heart surgery. Pediatr Cardiol. 2004; 25: 552–553.
- Dagan O, Nimri R, Katz Y, Birk E, Vidne B. Bilateral diaphragm paralysis following cardiac surgery in children: 10‐years’ experience. Intensive Care Med. 2006; 32: 1222‐1226.
- Garge SS, Passi GR, Ghanekar D. Early thoracoscopic plication of diaphragm in a newborn with brachial plexus palsy and concurrent phrenic nerve palsy. J Indian Assoc Pediatr Surg. 2017; 22: 165-167.
- Ahmadpour-Kacho M, Zahedpasha Y, Hadipoor A, Akbarian-Rad Z. Early surgical intervention for diaphragmatic paralysis in a neonate; report of a case and literature review. Iran J Pediatr. 2011; 21: 116-120.
- Snyder CW, Walford NE, Danielson PD, Chandler NM. A simple thoracoscopic plication technique for diaphragmatic eventration in neonates and infants: Technical details and initial results. Pediatr Surg Int. 2014; 30: 1013 1016.
- Podgaetz E, Garza-Castillon R Jr, Andrade RS. Best approach and benefit of plication for paralyzed diaphragm. Thorac Surg Clin. 2016; 26: 333-346.
- Radecki LL, Tomatis LA. Continuous bilateral electrophrenic pacing in an infant with total diaphragmatic paralysis. J Pediatr. 1976; 88: 969-971.
- Kratz T, Dauvergne J, Ruff R, Koch T, Breuer J, Asfour B, et al. In a porcine model of implantable pacemakers for pediatric unilateral diaphragm paralysis, the phrenic nerve is the best target. J Cardiothorac Surg. 2024; 19: 181.
