
Open Access, Volume 11
Tritirachium oryzae causing pulmonary infection: A rare case report from India
Renu Kumari Yadav; Immaculata Xess; Mragnayani Pandey; Bhaskar Rana; Gagandeep Singh*
Department of Microbiology, All India Institute of Medical Sciences, India.
Gagandeep Singh
Additional Professor, Department of Microbiology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi-110029, India.
Email: drgagandeep@gmail.com
Received : January 16, 2025,
Accepted : February 19, 2025
Published : February 28, 2025,
Archived : www.jclinmedcasereports.com
Abstract
The first case of Tritirachium oryzae isolated from pleural fluid of an Indian patient is reported. A 71-year-old female patient who is a follow up case of carcinoma colon, presented with complaint of recurrent vomiting, pain abdomen and loss of appetite. A possibility of disease relapse was kept and evaluation done. Whole body PET CT revealed bilateral pleural effusion. Fungal culture of pleural fluid revealed growth of a pigmented mould after 5 days of incubation. It was identified as Tritirachium oryzae on the basis of gross morphological characteristics and microscopic characterization on slide cultures. The diagnosis of T. oryzae was confirmed by PCR sequencing of the internal transcribed region of rDNA using the primer pairs ITS4 and ITS5. In vitro antifungal susceptibility test was also performed.
Initially before the fungal culture result came patient was started on ATT as patient had a history of pulmonary tuberculosis and no other diagnosis was made. After the fungal culture report patient was planned to start on voriconazole but patient condition deteriorates and she succumbed.
Keywords: Tritirachium spp., Pleural fluid; Fungal culture; AFST; PCR.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Singh G (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Yadav RK, Xess I, Pandey M, Rana B, Singh G. Tritirachium oryzae causing pulmonary infection: A rare case report from India. Open J Clin Med Case Rep. 2025; 2331.
Introduction
The genus Tritirachium is known to cause infection in insects. The natural habitat of this genus is soil and decaying plant material. Human infection by Tritirachium is rare; only a few case reports exist. Tritirachium is reported from corneal ulcer, scalp, nail and ear infections.
We report the first case of pulmonary infection caused by Tritirachium spp. isolated from pleural fluid from a 71-year-old immunocompromised female patient.
Case Report
A 71-year-old female patient who is a follow up case of carcinoma colon, diagnosed in april 2018, Right hemicoloctomy was done and patient was on chemotherapy. Patient also has a past history of pulmonary tuberculosis. Now patient presented with complaint of recurrent vomiting, pain abdomen and loss of appetite but passing flatus and stool. A possibility of disease relapse was kept and evaluation done, abdomen x-ray revealed multiple air fluid level; RT insertion with continuous drainage was done after surgical oncology opinion. Whole body PET CT revealed bilateral pleural effusion (L>R) and no other metabolically active lesion elsewhere. A diagnostic pleural tap was done and sent for AFB, gene xpert, amylase, sugar, ADA, malignant cytology, bacterial and fungal culture. All the investigations were negative and in mycology 10% potassium hydroxide preparation revealed no fungal elements but growth of a pigmented mould was seen on sabouraud dextrose agar with antibiotics after 5 days of incubation at 25 C. LPCB mount was prepared to identify the fungi.
Phenotypic Identification – Colonies on SDA showed vinaceous to lilac velvety surface growth on obverse and reverse was tan no pigmentation (Figure 1).
Slide culture preparations with LPCB stain showed subhyaline hyphae, which were pale to brown, smooth, and thin-walled. Conidiophores and conidiogenous cells were subhyaline. Conidiophores were well differentiated with thick-walled, suberect, and verticillately branched in the upper part of the conidiophores. Conidiogenous cells were arranged sympodially with strongly tapered and flask-shaped fertile rachis. Conidia were hyaline, smooth, and spherical to ellipsoidal. The isolate was identified morphologically as Tritirachium oryzae (Figure 2).
Confirmation of T. oryzae by Molecular Identification- Molecular identification was performed by sequencing the Internal Transcribed Sequence (ITS) region of rDNA using the primer pairs ITS4 and ITS5.
In vitro Antifungal Susceptibility Testing (AFST)- AFST was performed according to the CLSI standard; the results were- AmB 2.0 μg/ml, VOR 0.03 μg/ml, ITR 0.03 μg/ml, POS 0.03 μg/ml, CSP 0.12 μg/ml, and MFG 1.0 μg/ml.
Initially before the fungal culture result came patient was started on ATT as patient had a history of pulmonary tuberculosis and no other diagnosis was made. After 2-3 days of ATT her symptoms reduced and she started tolerating orally but suddenly her condition deteriorates. After the fungal culture report patient was planned to start on Voriconazole but patient condition deteriorate and she succumbed.
Table 1: Global review of Tritirachium human infections.
| Agent | Site of infection | Country | Age (yrs) | Gender | Identification | Treatment | Year | References |
|---|---|---|---|---|---|---|---|---|
| Tritirachiumroseum | Left eye corneal ulcer | USA | 29 | Male | Phenotypic | Nystatin, penetrating keratoplasty | 1975 | Rodrigues MM et al. [5] |
| Tritirachiumoryzae | Otomycosis | India | 45 | Male | Phenotypic | Clotrimazole | 2018 | Sharma SK et al. [6] |
| Tritirachiumoryzae | Finger nail | Iran | 44 | Female | Phenotypic and genotypic (ITS rDNA) | Oral itraconazole | 2013 | Naseri A et al.[7] |
| Tritirachiumoryzae | Human scalpinfection | Brazil | 4 | Female | Phenotypic | Topical treatmentwith ketoconazole shampoo | 2010 | Moraes RN et al.[8] |
| Tritirachiumoryzae | DLSO greattoe nail | India | 22 | Female | Phenotypic and genotypic (ITS rDNA) | Terbinafine, ketoconazole nailavulsion | 2018 | Vanam HP et al. [9] |
| Tritirachiumoryzae | Pleural fluid | India | 71 | Female | Phenotypic and genotypic (ITS rDNA) | ATT, Voriconazole | 2022 | Present study |

Figure 1: Growth of Tritirachium on Sabouraud Dextrose Agar.
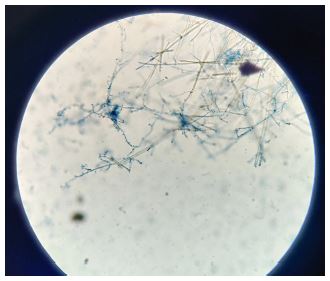
Figure 2: Tritirachium on Lacto phenol cotton blue mount (LPCB).
Discussion
The description of Tritirachium was first given by Limber in 1940 [1]. In India Tritirachium species was first described in 1967 [2]. Historically genus Tritirachium was placed in suborder Hyphomycetes which is obsolete now, and in recent taxonomical review, they are placed in subdivision Pezizomycotina. The new lineage Puccinomycotina includes class—Tritirachiomycetes, order— Tritirachiales, and family—Tritirachiaceae [3]. The genus Tritirachium has three accepted species: T. dependens, T. oryzae, and T. cinnamomeum. Other species which are under revision include T. roseum, T. egenum, and T. album [4]. Our isolate is matching with the description of T. oryzae. In this case of pleural effusion direct KOH mounts showed no fungal elements but grew readily on all the 3 tubes of SDA with cycloheximide, and gentamicin.
Though rare, human infections with T. oryzae have been reported in causing superficial mycoses which includes well-documented cases of corneal ulcers [5], otomycosis [6], onychomycosis [7], and scalp infection [8] but there have been no records of this fungus as the etiologic agent of pulmonary infection. In conclusion, T. oryzae is reported for the first time as the cause of pulmonary infection.
The paucity of isolates and fewer descriptions on T. oryzae bring out the succinct need for easy accessibility of molecular tools in making the identification less cumbersome. It is evident that T. oryzae is emerging as an opportunistic pathogen after its reported human cases. Future directions may include more studies on newer isolates and a robust antifungal agent reference spectrum. Molecular tools with classical description shall guide the trajectory of accurate taxonomical identification.
Declarations
Funding: The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Competing interests: The authors have no relevant financial or non-financial interests to disclose.
Author contributions: All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by [Dr. Gagandeep Singh], [Dr. Renu Kumari Yadav], [Dr. Immaculata Xess], [Bhaskar Rana]. The first draft of the manuscript was written by [Dr. Renu kumara yadav] and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
References
- Limber DP. A new form genus of the moniliaceae. Mycologia. 1940; 32: 23–30.
- Mehrotra BS, Basu M. A Tritirachium species from India. Mycopathologia et Mycologia Applicata. 1967; 32: 275–80.
- Schell WA, Lee AG, Aime MC. A new lineage in Pucciniomycotina: class Tritirachiomycetes, order Tritirachiales, family Tritirachiaceae. Mycologia. 2011; 103: 1331–40.
- Beguin H. Tritirachium egenum, a thiamine-and siderophore-auxotrophic fungal species isolated from a Penicillium rugulosum. FEMS Microbiol Ecol. 2010; 74: 165–73.
- Rodrigues MM, Laibson P, Kaplan W. Exogenous corneal ulcer caused by Tritirachium roseum. Am J Ophthalmol. 1975; 1975: 804–6.
- Sharma SK, Gupta S, Singh P, Kumar S. Otomycosis caused by Tritirachium oryzae: A rare fungal pathogen. Indian J Med Microbiol. 2018; 36: 257-8.
- Naseri A, Fata A, Najafzadeh MJ. First case of Tritirachium oryzae as agent of onychomycosis and its susceptibility to antifungal drugs. Mycopathologia. 2013; 176: 119–22.
- Moraes RN, Ribeiro MC, Nogueira MC, Cunha KC, Soares MM, Almeida MT. First report of Tritirachium oryzae infection of human scalp. Mycopathologia. 2010; 169: 257–9
- Vanam HP, Rao PN, Mohanram K, Yegneswaran PP, Rudramurthy SP. Distal lateral subungual onychomycosis owing to Tritirachium oryzae: a bystander or invader?. Mycopathologia. 2018; 183: 459-63.
