
Open Access, Volume 11
Treatment of calcified residuals from severe acne with collagen biopeptide supplementation: Case report and literature review
Luisa Cerutti, MD, PhD1*; Arianna Bellitti, MD2; Federica Bartiromo, MD3; Federica Fazio, MD4
1Free Lance, Specialist in General Surgery, Aesthetic Doctor, External Professor at Sapienza University Level II Master: Aesthetic and Regenerative Medicine, Rome, Italy.
2Aesthetic Medicine, Specialist in Radiology, Medical Director at Sant’Andrew Hospital, Rome, Italy.
3Specialist in Gynecology and Obstetrics, Aesthetic Doctor, Rome, Italy.
4University of Magna Graecia, Department of Medical and Surgical Sciences, Aesthetic Medicine, Catanzaro, Italy.
Luisa Cerutti
Specialist in General Surgery, Aesthetic Doctor, External Professor at Sapienza University Level II Master: Aesthetic and Regenerative Medicine, Rome, Italy.
Email: luisacerutti66@gmail.com
Received : January 30, 2025,
Accepted : February 17, 2025
Published : February 28, 2025,
Archived : www.jclinmedcasereports.com
Abstract
We present the case of a patient with visible scarring from severe acne who sought medical-aesthetic consultation. The patient was treated with systemic therapy using a dietary supplement containing collagen biopeptides.
The treatment proved to be effective from a visual inspection perspective, and the result was supported by targeted and selective ultrasound imaging with a new diagnostic protocol specific for skin analysis, confirming a significant reduction in subdermal calcifications. This is the first reported case of this kind in the literature.
Keywords: Acne; Scarring; Dietary supplementation; Collagen biopeptides; Ultrasound imaging.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Cerutti L (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Cerutti L, Bellitti A, Bartiromo F, Fazio F. Treatment of calcified residuals from severe acne with collagen biopeptide supplementation: Case report and literature review. Open J Clin Med Case Rep. 2025; 2330.
Introduction
Acne is one of the most common skin conditions, often causing significant psychological distress, especially when visible scarring remains.
Its etiopathogenesis is multifactorial, with major contributing factors including:
• Genetic predisposition
• Hormonal imbalances (androgens, GH, IGF-1, polycystic ovary syndrome)
• Bacterial colonization of the pilosebaceous follicle
• Environmental factors (smoking, stress, pollution, improper cosmetic use, high-glycemic diet, dairy, saturated fats)
This results in the formation of both non-inflammatory (comedones) and inflammatory lesions (papules, pustules, nodules, cysts), often presenting with a chronic-relapsing course.
Acne treatments, whether invasive or non-invasive, are not always sufficiently effective, and camouflage techniques can only conceal but not eliminate the problem, forcing patients to live with persistent scars and skin irregularities.
The choice of pharmacological treatment depends on the severity of the condition, patient preferences, individual characteristics, and treatment tolerance.
Anti-acne medications can be administered either topically (local action) or orally (systemic action), and in severe cases, a combined approach is recommended.
Alpha-Hydroxy Acid (AHA) peels, particularly glycolic acid peels, are commonly used in aesthetic dermatology to improve skin texture and reduce acne-related damage.
Case Report
Patient R.B., a 58-year-old female, first developed acne at age 13, with a worsening of symptoms at menarche (age 14). Over the years, multiple dermatological evaluations documented severe acne with subdermal cysts.
Previous treatments
• Systemic therapy with isotretinoin (Roaccutan®)
• Topical pharmacological treatments
• Repeated glycolic acid peels
By age 35, the patient noticed improvement in subdermal cysts, but acne scars remained unchanged. Despite undergoing dermatological check-ups and various treatments, no significant improvement was observed.
Upon reaching menopause at age 50, she noticed a palpable increase in subdermal cysts. Repeated dermatological consultations failed to provide an effective therapeutic solution.
New therapeutic approach
The patient consulted us for aesthetic medical reasons unrelated to her acne scarring. She was prescribed a systemic supplementation therapy with collagen biopeptides, one vial per day for 60 days. She underwent clinical inspections, photographic documentation, and ultrasound imaging evaluations.
Ultrasound evaluation protocol
A targeted high-resolution ultrasound analysis was performed using Philips EPIQ Elite with «nSight Imaging» and ElastQ Imaging technology for shear wave elastography.
The transducer used was PureWave Crystal Technology eL18-4 Matrix Array, with a frequency range of 2 MHz to 22 MHz.
Key Findings:
• Morphological assessment: High-frequency (18 MHz) transversal scans at the cheek level, parallel to the mandibular branch, evaluating dermal and hypodermal thickness (Figure 1).
• Elasticity assessment: Shear Wave Elastography with color-coded confidence mapping, generating elastograms (color mapping from blue-green to orange-red, indicating different elasticity levels) (Figure 2).
Results
At 15 days of therapy, ultrasound imaging revealed a significant reduction in subdermal cysts. This result was confirmed at a 3-month follow-up ultrasound after cessation of supplementation.
Additionally, the patient reported the spontaneous drainage of some cysts during compression.
At the 3-month follow-up:
• The skin was more elastic, less fibrotic, and less seborrheic.
• A notable improvement in facial aesthetics was observed.
This case suggests that collagen biopeptide supplementation may be an effective adjuvant therapy for managing calcified post-acne residuals, warranting further studies to explore its potential therapeutic applications.
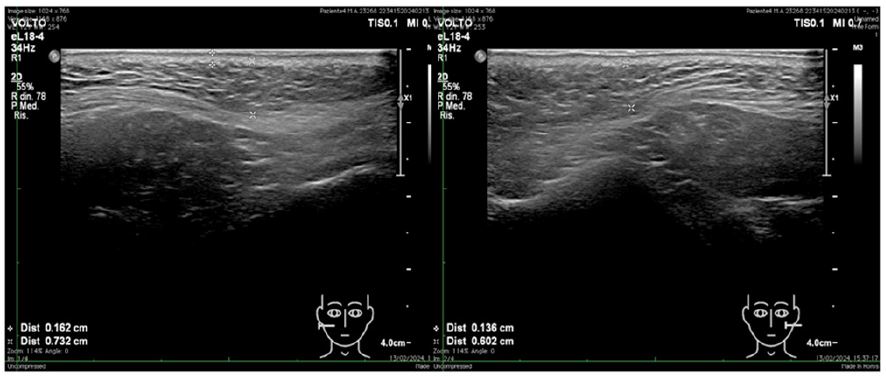
Figure 1: Ultrasound morphological assessment. High-frequency (18 MHz) transversal scans at the cheek level, parallel to the mandibular branch, evaluating dermal and hypodermal thickness.

Figure 2: Shear Wave Elastography with color-coded confidence mapping, generating elastograms (color mapping from blue-green to orange-red indicating different elasticity levels).
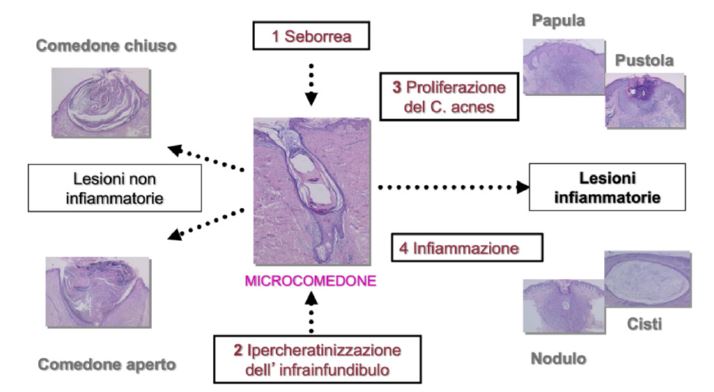
Figure 3: Types of acne lesions. [Cited from: James j leyden. New understanding of the pathogenesis of acne. Jam acad dermatol 1995].
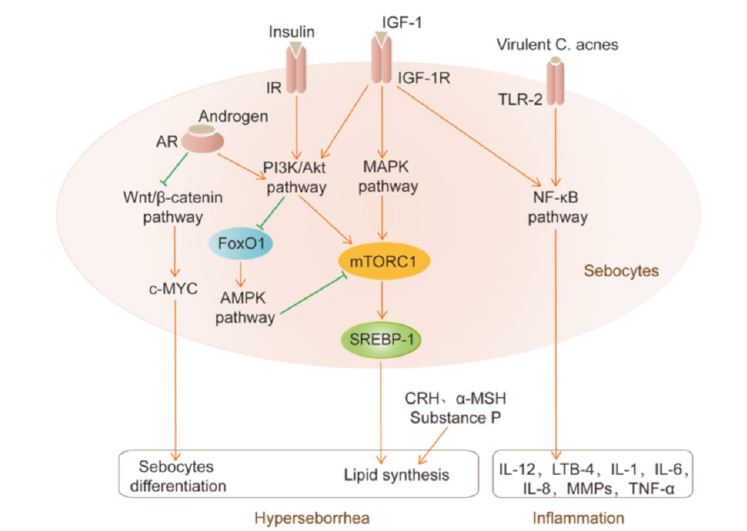
Figure 4: Mechanisms involved in the etiopatogenesis of acne. [Cited from: Cong, t.x. Et al. From pathogenesis of acne vulgaris to antiacne agents. Archives of dermatological research].

Figure 5: Ultrasound High-frequency (18 MHz) transversal scans at the cheek level, parallel to the mandibular branch before and after treatment, showing reduction in scar extension, decrease of calcifications and an improvement in dermal thickness and trophism.
Discussion and Literature Review
To date, the use of collagen-containing supplements for the treatment of subdermal cysts resulting from acne pathology does not appear to have been described in the literature. In our case, this therapy demonstrated clear efficacy in reducing subcutaneous cystic outcomes of chronic acne pathology, despite the patient having undergone numerous specific acne treatments over the years without success.
Etiopathogenesis of acne
Acne has a multifactorial etiopathogenesis, with both endogenous and exogenous components. These include genetic factors, hormonal imbalances (androgens, GH, IGF-1, polycystic ovary syndrome), bacterial colonization of the hair follicle, and environmental factors (smoking, stress, pollution, improper use of cosmetics, diet rich in high-glycemic-index foods, dairy products, and saturated fats). This leads to the formation of both non-inflammatory lesions (comedones) and inflammatory lesions (papules, pustules, nodules, cysts), often concomitant with a chronic-relapsing course.
Many mistakenly believe that acne is caused by poor personal hygiene; however, this is untrue, as it is well known that the use of aggressive cleansers or scrubs worsens the clinical picture. The cells involved in the pathogenic process include keratinocytes, sebocytes, dendritic cells, leukocytes, lymphocytes, and macrophages. Acne can be classified into comedonal, papulopustular, nodulocystic, and conglobate forms depending on the type of lesions present (Figure 3).
The microbiota, composed of approximately 90% C. acnes bacteria, varies within the pilosebaceous unit based on the individual’s age and is predominant during puberty. Several mechanisms involving C. acnes contribute to acne development (Figure 4):
1. Sebum production at the glandular level favors the growth of C. acnes [1,2], along with increased activity of an enzyme that enhances seborrhea [3].
2. Comedones form due to the accumulation of corneocytes and keratinocytes within the follicle, where C. acnes develops a biofilm that increases keratinocyte adhesion, activates the IGF-1 receptor signaling pathway, and promotes keratinocyte proliferation and comedone formation [4,5].
3. By binding to TLR-2/-4 receptors on keratinocytes, C. acnes stimulates the production of interleukins, TNF-α, and cytokines, increasing inflammation and damaging hair follicles and sebaceous glands through enzymatic activity [1].
Diet and acne
Diet appears to play a key role in acne pathogenesis, although definitive data on specific food correlations remain lacking. High-glycemic-index foods (bread, pasta, sweets, sugary drinks) and dairy products are implicated as cofactors in acne onset due to their ability to increase IGF-1 secretion, whereas low-carb/ketogenic diets appear to have a protective effect [6,7]. Observational studies on various ethnic populations have shown a minimal prevalence of acne in Asian and indigenous Latin American and Oceanian populations, which share diets rich in fish, tubers, and game while excluding refined foods, alcohol, and coffee. This suggests that environmental factors also influence acne development [8]. Polyphenols, such as those in green tea, exhibit antimicrobial properties and reduce sebum secretion, positively impacting acne pathology. Fat-rich foods and chocolate appear to have a mild role in acne exacerbation [9,10].
Hormonal Influence
Hormones regulate sebum production by stimulating sebaceous glands. Androgens, GH, and IGF-1 [11] promote sebum secretion, whereas estrogens exert a protective effect by inhibiting sebaceous gland activity [12] and reducing androgen production at the gonadal level. Patients with Polycystic Ovary Syndrome (PCOS) present with elevated cortisol and androgen levels, predisposing them to severe acne [13]. GH and IGF-1 also regulate sebum production both in pilosebaceous units and through androgen modulation. IGF-1 increases lipogenesis and androgen receptor expression, suggesting that reducing its levels may improve acne [14].
Environmental pollution
Air pollution increases oxidative stress on the skin, disrupts normal skin functions, and exacerbates inflammation, already heightened in acne patients due to altered lipid barrier function.
Therapeutic approaches
Pharmacological treatment of acne includes topical and systemic therapies. Topical treatments include retinoids (e.g., adapalene), which modulate cellular proliferation and differentiation, increasing turnover and reducing corneocyte adhesion; antimicrobials (antibiotics reducing bacterial colonization and inflammation, benzoyl peroxide combined with antibiotics to minimize resistance, azelaic acid with keratolytic and antimicrobial effects reducing hyperpigmentation); and salicylic acid for its keratolytic action. These are generally recommended for mild to moderate acne, with increased efficacy when combined. However, topical treatments often cause initial irritation (erythema, desquamation, burning).
For moderate to severe acne, oral hormonal therapies (especially antiandrogens and inhibitors of ovarian or adrenal androgen production) and isotretinoin are recommended [19]. Oral isotretinoin is among the most effective treatments for severe acne unresponsive to other therapies. It locally atrophies sebaceous glands, reduces sebum production, inhibits sebocyte differentiation, normalizes follicular keratinization, and lowers bacterial load. Systemically, it may cause nausea, vomiting, photophobia, desquamation, hypercholesterolemia, depression, myalgia, spontaneous abortion, and severe fetal malformations [20].
Our patient had undergone multiple cycles of glycolic acid peels without success. Glycolic acid corrects abnormal keratinization, loosens keratinocytes in sebaceous glands [22-24], stimulates dermal collagen, thickens the dermis, and improves acne scarring [25]. Studies indicate significant improvements in inflammatory and non-inflammatory acne lesions after 12 weeks, with benefits in post-acne pigmentation [26].
Collagen supplementation
The patient received a liquid dietary supplement containing bioactive collagen peptides (2 kDa molecular weight), administered as a 25 ml daily single-dose vial. This formulation provided 5000 mg of hydrolyzed collagen peptides per dose, partially surviving digestion, crossing the intestinal barrier intact, and exerting bioactivity on target tissues. These peptides were derived from enzymatic hydrolysis of bovine collagen and subsequently purified, concentrated, and sterilized.
Clinical studies indicate that oral collagen supplementation reduces signs of skin aging, has a favorable safety profile, and may synergize with other antioxidant or anti-inflammatory agents [27]. Optimal doses, molecular weights, and treatment duration remain to be determined.
Collagen comprises 75% of the extracellular matrix’s total weight, maintaining skin firmness and elasticity. Type I collagen, the most abundant in the dermis, provides structural support, while type III collagen contributes to skin flexibility. Collagen synthesis declines with age, increasing degradation and leading to visible skin imperfections. Hydrolyzed collagen supplements enhance skin density and firmness by stimulating fibroblast metabolism and hyaluronic acid production [28,29]. Studies show improved skin elasticity and reduced wrinkles, with sustained benefits post-treatment [30].
Collagen supplements often include additional synergistic components:
• Vitamin C (80 mg), a key antioxidant and collagen synthesis coenzyme [31,32]
• Vitamin E (3 mg), an antioxidant inhibiting lipid peroxidation and inflammation, preserving hydration [35]
• Biotin (0.15 mg), beneficial for skin hydration, elasticity, and hair/nail health
• Copper (0.15 mg) and Zinc (4 mg), essential for collagen synthesis and extracellular matrix stability
• Hyaluronic acid (15 mg), crucial for hydration and anti-inflammatory properties [38]
The use and benefits of the collagen biopeptide-based supplement have been highlighted in our case through a targeted ultrasound study of the skin, representing a new approach to imaging in aesthetic medicine.
A thorough literature review was conducted beforehand to identify a pilot study with parameters and reference values in healthy patients [40-43]. The selected region for morphological and elastosonographic evaluation was the cheek, as the skin layers of interest in this study are better represented and therefore more measurable in this area.
The morphological examination documented, in the initial ultrasound, a heterogeneous dermis with the presence of some calcifications within its structure and focal areas of relative linear hyperechogenicity, indicative of minor fibrotic scarring (the patient reported having suffered from severe acne during adolescence). However, during the final follow-up, a reduction in scar outcomes was observed, evidenced by a decrease in calcifications and an improvement in dermal thickness and trophism (Figure 5).
Conclusions
Dietary supplementation can play a crucial role in improving skin health, particularly in patients with complex conditions such as scar outcomes and subdermal cysts.
Treatment with active collagen biopeptides is well tolerated, free of significant side effects, and appears to provide several benefits, including skin collagen regeneration, improved hydration, scar reduction, and decreased skin inflammation.
This study suggests that the therapeutic approach adopted is effective not only in the short term but also in maintaining positive long-term results. The reduction of calcifications and the preservation of the dermis’ elastic properties represent a significant achievement in the management of complex dermal conditions.
The application of new ultrasound protocols, including Shear Wave Eastography (SWE), has allowed for an objective assessment of skin elasticity properties and, in our case, has demonstrated the efficacy of treatment with active collagen biopeptides.
Further prospective, large-scale studies will be necessary to confirm our findings.
References
- Xu H, Li H. Acne, the Skin Microbiome, and Antibiotic Treatment. American Journal of Clinical Dermatology. 2019; 20: 335–344.
- Leyden JJ, McGinley KJ, Vowels B. Propionibacterium acnes colonization in acne and nonacne. Dermatology. 1998; 196: 55–58.
- Inuma, K. et al. Involvement of propionibacterium acnes in the augmentation of lipogenesis in hamster sebaceous glands in vivo and in vitro. Journal of Investigative Dermatology. 2009; 129: 2113–2119.
- Jarrousse V, Castex-Rizzi N, Khammari A, Charveron M, Dréno B. Modulation of integrins and Wlaggrin expression by Propionibacterium acnes extracts on keratinocytes. Arch Dermatol Res. 2007; 299: 441–447.
- Isard O, et al. Propionibacterium acnes activates the IGF-1/IGF-1R system in the epidermis and induces keratinocyte proliferation. J Invest Dermatol. 2011; 131: 59–66.
- Bowe WP, Joshi SS, Shalita AR. Diet and acne. J Am Acad Dermatol. 2010; 63: 124–141.
- Melnik BC, Schmitz G. Role of insulin, insulin-like growth factor-1, hyperglycaemic food and milk consumption in the pathogenesis of acne vulgaris. Exp Dermatol. 2009; 18: 833–841.
- Conforti C, et al. Acne and diet: a review. International Journal of Dermatology Preprint at. 2021.
- Zouboulis CC, Katsambas AD, Kligman AM. Pathogenesis and treatment of acne and rosacea. Pathogenesis and Treatment of Acne and Rosacea. 2013.
- Mahmood SN, Bowe WP. Diet and acne update: Carbohydrates emerge as the main culprit. Journal of Drugs in Dermatology. 2014: 13.
- Hon KLE, Leung AKC. Acne: Causes, Treatment, and Myths. (Nova Science Publishers, 2010).
- Habif TP, Campbell JL, Chapman MS, Dinulos JG, Zug KA. Acne, rosacea and related disorders. in Skin Disease. 2011.
- Zaenglein A, Thiboutot D. Dermatology. in (eds. Bolognia, J. L., Jorizzo, J. L. & Rapini R.P.) (Gulf Professional Publishing. 2008).
- Melnik BC, Schmitz G. Role of insulin, insulin-like growth factor-1, hyperglycaemic food and milk consumption in the pathogenesis of acne vulgaris. Exp Dermatol. 2009; 18: 833–841.
- Katsambas AD, Cunliffe WJ, Zouboulis CC. Clinical aspects of acne vulgaris. in Pathogenesis and Treatment of Acne and Rosacea. 2014: 9783540693758 213–221.
- Moon J, Yoon JY, Yang JH, Kwon HH, Min S, Suh DH. Atrophic acne scar: a process from altered metabolism of elastic fibres and collagen fibres based on transforming growth factor-beta1 signalling. Br J Dermatol. 2019; 181: 1226-1237.
- Fabbrocini G, Annunziata MC, D’Arco V, De Vita V, Lodi G, Mauriello MC, et al. Acne scars: pathogenesis, classification and treatment. Dermatology Research and Practice. 2010.
- Tsuji T, Sawabe M. Elastic fibers in scar tissue: scanning and transmission electron microscopic studies. J Cutan Pathol. 1987; 14: 106-13.
- Guidelines of American Academy of Dermatology e dell’American Academy of Pediatrics.
- Rigopoulos D, Larios G, Katsambas AD. The role of isotretinoin in acne therapy: why not as first-line therapy? facts and controversies. Clin Dermatol. 2010: 28.
- Glycolic acid peel therapy - a current review. Sharad J. Clin Cosmet Investig Dermatol. 2013; 6: 281-8.
- Sarkar R, Ghunawat S, Garg VK. Comparative Study of 35% Glycolic Acid, 20% Salicylic-10% Mandelic Acid, and Phytic Acid Combination Peels in the Treatment of Active Acne and Postacne Pigmentation. J Cutan Aesthet Surg. 2019; 12: 158-163.
- Kessler E, Flanagan K, Chia C, Rogers C, Glaser DA. Comparison of alpha- and beta-hydroxy acid chemical peels in the treatment of mild to moderately severe facial acne vulgaris. Dermatol Surg. 2008; 34: 45-50.
- Takenaka Y, Hayashi N, Takeda M, Ashikaga S, Kawashima M. Glycolic acid chemical peeling improves inflammatory acne eruptions through its inhibitory and bactericidal effects on Propionibacterium acnes. J Dermatol. 2012; 39: 350–4.
- Sharad J. Combination of microneedling and glycolic acid peels for the treatment of acne scars in dark skin. J Cosmet Dermatol. 2011; 10: 317–23.
- Grover C, Reddu BS. The therapeutic value of glycolic acid peels in dermatology. Indian J Dermatol Venereol Leprol. 2003; 69: 148–50.
- D Morgado-Carrasco, J Gil-Lianes, E Jourdain, J Piquero-Casals. Oral Supplementation and Systemic Drugs for Skin Aging: A Narrative Review. Actas Dermosifiliograf. 2023; 114: 114-124.
- De Miranda RB, Weimer P, Rossi RC. Effects of hydrolyzed collagen supplementation on skin aging: A systematic review and meta-analysis. Int J Dermatol. 2021; 60: 1449-61.
- Ohara H, Ichikawa S, Matsumoto H, Akiyama M, Fujimoto N, Kobayashi T, et al. Collagen-derived dipeptide, prolinehydroxyproline, stimulates cell proliferation and hyaluronic acid synthesis in cultured human dermal fibroblasts. J Dermatol. 2010; 37: 330-8.
- Maia Campos PM, Franco RS, Kakuda L, Cadioli GF, Costa GM, Bouvret E. Oral supplementation with hydrolyzed fish cartilage improves the morphological and structural characteristics of the skin: A double-blind placebo-controlled clinical study. Molecules. 2021; 26: 4880.
- Rian AA Wijkmans, Koen Talsma. Modern scurvy. J Surg case rep. 2016; 2016: rjv168.
- Yong Cool Boo. Acorbic Acid (Vitamin C) as a Cosmeceutical to increase Dermal Collagen for Skin Antiaging purposes: Emerging Combination Therapies. Antioxidants (Based). 2022; 11: 1663.
- Ryu TK, Lee H, Yon DK, Nam DY, Lee SY, Shin BH, et al. The antiaging effects of a product containing collagen and ascorbic acid: In vitro, ex vivo, and pre-post intervention clinical trial. PLoS One. 2022; 17: e0277188.
- Al-Niaimi F, Chiang NYZ. Topical Vitamin C and the Skin: Mechanisms of Action and Clinical Applications. J Clin Aesthet Dermatol. 2017; 10: 14-17.
- Wang Z, Xu R, Yang H, Li R, Ding J, Chang Y, et al. Vitamin E Regulates the Collagen Contents in the Body Wall of Sea Cucumber (Apostichopus japonicus) via Its Antioxidant Effects and the TGF-beta/Smads Pathway. Antioxidants (Basel). 2024; 13: 847.
- Januszewski J, Forma A, Zembala J, Flieger M, Tyczyńska M, Dring JC, et al. Nutritional Supplements for Skin Health-A Review of What Should Be Chosen and Why. Medicina (Kaunas). 2023; 60: 68.
- Podgórska A, Kicman A, Naliwajko S, Wacewicz-Muczyńska M, Niczyporuk M. Zinc, Copper, and Iron in Selected Skin Diseases. Int J Mol Sci. 2024; 25: 3823.
- Hiroki Ohara, Satomi Ichikawa, Hitoshi Matsumoto, Minoru Akiyama, Norihiro Fujimoto, Takashi Kobayashi, et al. Collagen-derived dipeptide, proline-hydroxyproline, stimulates cell proliferation and hyaluronic acid synthesis in cultured human dermal fibroblasts. J Dermatol. 2010: 37.
- Hyaluronic Acid-Extraction Methods, Sources and Applications. Graciela CQ, José Juan EC, Gieraldin CL, Xóchitl Alejandra PM, Gabriel AÁ. Polymers (Basel). 2023; 15: 3473.
- Marcin Ambroziak, Bartłomiej Noszczyk, Piotr Pietruski, Wiesław Guz, Łukasz Paluch; Elastography reference values of facial skin elasticity; Adv Dermatol Allergol. 2019; 36: 626–634.
- Łukasz Paluch, Piotr Pietruski, Bartłomiej Noszczyk, Bartłomiej Kwiek, Marcin Ambroziak; Intra-rater reproducibility of shear wave elastography in the evaluation of facial skin; Adv Dermatol Allergol. 2020; 37: 371–376.
- Arinc Ozturk, Joseph R Grajo, Manish Dhyani, Brian W Anthony, Anthony E Samir. PRINCIPLES OF ULTRASOUND ELASTOGRAPHY; AbdomRadiol(NY). 2018; 43: 773–785.
- Marcin Ambroziak, Piotr Pietruski, Bartłomiej Noszczyk, Łukasz Paluch. Ultrasonographic elastography in the evaluation of normal and pathological skin – a review; Adv Dermatol Allergol. 2019; 36: 667-672.
