
Open Access, Volume 11
Traumatic obturator dislocation of the hip: A case report
Sidimé S*; Diallo AMF; Aboud A; Barry A; Diallo MM; Camara T; Lamah L
Department of Orthopaedics Traumatology, Donka National Hospital, Conakry, Guinea.
Sory Sidime
Department of Orthopaedics Traumatology, Donka National Hospital, Conakry, Guinea.
Tel: 00-224-624-11-94-57;
Email: sidimesidex@yahoo.fr
Received : January 17, 2025,
Accepted : February 14, 2025
Published : February 28, 2025,
Archived : www.jclinmedcasereports.com
Abstract
Traumatic anterior dislocation of the hip without fracture of the acetabulum or femoral head is rare. They are often secondary to high-energy kinetic accidents. Early therapeutic management in a specialized facility prevents the risk of complications.
We report the case of an obturator dislocation of the left hip in a 31-year-old merchant following a road traffic accident.
Keywords: Dislocation; Obturator; Accident; Traffic; Road; Complications.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Sidime S (2025)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Sidimé S, Diallo AMF, Aboud A, Barry A, Diallo MM. Traumatic obturator dislocation of the hip: A case report. Open J Clin Med Case Rep. 2025; 2329.
Introduction
Traumatic coxofemoral dislocation in adults is defined as total and permanent posterior or anterior displacement of the femoral head from the acetabular cavity [1].
Hip dislocation has become more and more frequent in recent decades, due to the increase in road traffic accidents, particularly motorcycle cabs. There are 2 types of pure hip dislocation: posterior dislocation is the most common (75%) [2], with its two forms, iliac (50%) and ischial (25%), and anterior dislocation (25%), with its two forms, pubic (15%) and obturator (10%) [3]. The obturator variety, which occurs during forced flexion, abduction and external rotation [4], is rarely observed.
We report a case of obturator dislocation of the left hip in a 31-year-old merchant following a motorcycle traffic accident.
Clinical Observation
This is a 31-year-old merchant with no previous morbid history who was the victim of a road traffic accident. He was a rear passenger in a motorcycle cab with a shoe bag between his thighs when he collided with another motorcycle cab with an impact to the inside of the left knee.
One hour after the accident, he was admitted to the emergency department with pain and functional impotence of the left pelvic limb and hip deformity.
Clinical examination revealed a pelvic limb in flexion, abduction and external rotation (Figure 1).
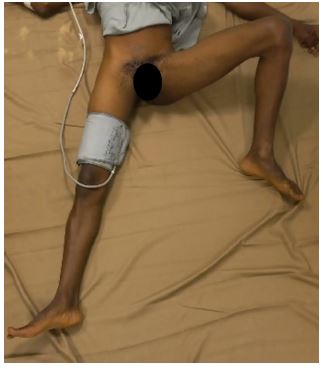
Figure 1: Clinical image at reception, showing the left pelvic limb in a vicious attitude, hip in flexion, abduction and external rotation.

Figure 2: Front pelvic X-ray showing left obturator dislocation.
The vascular and neurological examination was normal, and the rest of the examination was unremarkable. An emergency radiograph of the pelvis showed an anterior obturator dislocation of the left hip (Figure 2).
The patient was rushed to the operating room for reduction of his dislocation. The reduction was performed 30 minutes after his arrival at the emergency room, under general anesthesia. After sedation, he was placed on the floor and reduction was performed using the ALLIS maneuver : an assistant stabilizing the pelvis, knee flexed to release the hamstring, operator pulling in the axis of the femur with slight adduction and internal rotation of the hip. A clicking sound was audible during reduction. On testing, the hip was stable after reduction, with no inequality in pelvic limb length (Figure 3).
Radiographic control using an image intensifier confirmed reduction without associated bone lesions or intra-articular fragments (Figure 4), as did a control radiograph of the front pelvis at D2 (Figure 5).
CT scan before and after immediate reduction could not be performed. Related to what?.
Follow-up imaging at M22, in particular X-ray and CT scan, showed no evidence of osteonecrosis of the femoral head.
The 22-month follow-up showed a PMA functional score of 18, with no hip stiffness or pain.

Figure 3: Clinical image of the patient after reduction, showing normal attitude of the pelvic limbs.

Figure 4: Scopic inspection confirming reduction without associated bone lesions or intra-articular fragments.

Figure 5: Front view of pelvis after orthopedic reduction.
Discussion
Traumatic obturator dislocation is a rare variety of hip dislocation [5].
The rarity of obturator anterior dislocation of the hip is due to the strong anterior capsule and Y-shaped ligament of Bigelow [6]. Traffic accidents are responsible for the majority of this type of dislocation, and exceptional cases have been described during sports activities [7]. In our case, the dislocation occurred after a road traffic accident involving two two-wheeled machines.
The anterior dislocation occurred during flexion-abduction-external rotation on impact with the medial aspect of the knee, with a cam effect of the greater trochanter on the ilium in maximum abduction [4].
This mechanism was found in our case: the patient supported on a motorcycle with a shoe bag placed between the thighs, an attitude which puts the hip in abduction-external rotation flexion.
Several studies in the literature show different classifications of hip dislocations (classification by Levin, Dunn, Bigelow, Castaing, Pipkin etc.) [6,8]. We used Epstein’s classification for our patient.
Dislocation is an orthopaedic emergency, and closed reduction is the routine treatment for traumatic forms of the anterior obturator type [2,3].
The therapeutic management of obturator dislocation is an orthopaedic emergency, and reduction should be performed under general anaesthetic, with complete muscle relaxation using a first traction manoeuvre in the axis of the femur, followed by adduction and internal rotation of the femoral head [9]. The ideal time to achieve this reduction remains controversial. According to Houggard, it is less than six hours [10], but according to Brau AE, it could be up to twelve hours [11].
In our case, reduction was performed one hour and thirty minutes after the trauma. Under general anaesthesia, the patient was placed on a hard surface and the limb was pulled in line with the femur, followed by internal rotation and extension of the limb.
After reduction, some authors recommend light traction for analgesic purposes for a few days. A six-week period of offloading, with gradual resumption of weight-bearing, is the rule. Rehabilitation should be carried out early on, focusing on active mobilization [12].
At present, there are no scientific arguments to justify the benefits of traction and unloading in reducing the risk of cephalic necrosis of the femoral head [13]. Cantonné et al. recommend early weight-bearing, then total weight-bearing at d15, with avoidance of external rotation for 03 weeks in the case of anterior dislocation [14].
Traction was applied for 03 weeks, followed by non-weight-bearing walking for a further three weeks. Full weight-bearing was allowed on the 45th day of reduction.
The risk of cephalic necrosis increases with the delay in reduction. This risk is 30% in adults [15]. Houggard [10] observed 47% necrosis when the reduction delay exceeded 6 hours.
The long-term risk is marked by necrosis of the femoral head (4%); this risk is increased when the reduction time exceeds 3 hours [16], with a necrosis rate of less than 15% in the case of reduction before 12 hours and over 50% beyond that [17].
However, these figures mainly concern lesions associated with acetabular or femoral head fractures, and the rate is certainly lower in isolated dislocations, as observed in our study.
Conclusion
Anterior obturator dislocation of the hip is rare.
Its rarity is due to the stability of the hip joint, its deep position and the capsule of strong ligaments and muscles surrounding it. Early diagnosis and management are crucial to avoid aseptic necrosis of the femoral head.
Declarations
Conflicts of interest: The authors declare no conflict of interest in connection with the writing of this article.
Author’s contributions: Sidimé S: Principal author, designer of the data sheet, initiation of work and drafting of the article; Diallo AMF: Processing of files and completion of forms; Aboud A: Statistical study; Barry A: Reading; Diallo MM: Reading; Camara T: Correction; Lamah L: Correction.
References
- Goddar NJ. Classification of traumatic hip dislocation. Clin Orthop. 2000; 377: 11-14.
- Merle D’Aubigné R, Mazas F. Luxations postérieures traumatiques de la hanche. Ann Chir. 1963; 17: 1063-90.
- A Reigstad. Traumatic dislocation of the hip. J Trauma. 1980; 20: 603-606.
- Toms AD, Williams S, White SH. Obturator dislocation of the hip. J Bonne Joint Surg (Br). 2001; 83: 113-115.
- Pietu G, Malissar M, Maynaud G, Letenneur J. Luxations traumatiques pures de la hanche. EMC Paris. 1993: 14077.
- Phillips AM, Konchwalla A. The pathologic features and mechanism of traumatic dislocation of the hip. Clin Orthop Relat Res. 2000: 7-10.
- Bouya A, et al. Luxation obturatrice de la hanche : survenue rare en milieu sportif. J Traumatol Sport. 2017; 12-001.
- Pfeifer K, Leslie M, Menn K, Haims A. Imaging findings dislocations of Skeletal anterior. Radiol hip. 2017; 46: 723-730.
- Ries P, Gayet Le, Bonnet L, Clarac JP. Un cas de luxation obturatrice traumatique de la hanche chez une enfant de 4 ans. Rev ChirOrthop. 1991; 77: 49-52.
- Hougaard K. Traumatic posterior dislocation of the hip: pronostic factors influencing the incidence of avascular necrosis of femoral head. ArchOrthop Trauma Surg. 1986; 106: 32–5.
- Brau AE. Traumatic dislocation of the hip. J Bone Joint Surg (Am). 1962; 44: 1115-34.
- Chafik H. la luxation obturatrice traumatique de la hanche chez l’adulte à propos d’un cas et revue de la littérature. IOSR Journal of Dental and Médical Science (IOSR-JDMS). 2020; 19: 48-52.
- Pietu G, Mallisard M, Raynaud G. Letenneur J. Luxations traumatiques pures de la hanche. Encycl Med Chir app Locom. 1993; 6.
- Catonné Y, Meyer A, Sariali E, Biette G. Pathologie du complexe pelvi-fémoral du sportif. Pathologie du complexe pelvi-fémoral du sportif. 2009; 88-99.
- Glass A. Traumatic dislocation of the hip in children: an analysis of forty-seven patients. J Bone Joint Surg. 1961; 43: 29.
- Farag AW, Shohayeb KA. Intrapelvic dislocation of the head of femur through the obturator foramen associated with ipsilateral fracture femur. J Bone Joint Surg (Br). 2003; 85: 1056-1058.
- Olmi R, Toni A, Sudanese A, Del Prete G, Greggi L. Incidence of coxarthrosis as a result of traumatic hip dislocation, 14-year follow-up. Chir Organi Mov. 1986; 71: 325-330.
