
Open Access, Volume 10
Targeting BCMA with belantamab mafodotin: A review of mechanisms, clinical efficacy and future directions
Mahith Varma Sayyaparaju*; Jannat Sheikh; Kalyani Kuthadi; Sriharsha Mandallika; Akhila Kanka
Researcher, Internal medicine, New York Medical College St. Clare’s/ St. Mary’s, New Jersey, USA.
Mahith Varma Sayyaparaju
Researcher, Internal medicine, New York Medical College St. Clare’s/ St. Mary’s, New Jersey, USA.
Email: varmamahith777@gmail.com
Received : September 11, 2024,
Accepted : October 03, 2024
Published : October 15, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Multiple Myeloma (MM) remains a challenging and incurable malignancy, particularly in patients with severe relapsed/refractory (RRMM) disease who struggle to achieve significant response despite being on combination therapy [1].
Despite the advent of various immunotherapies treating patients with RRMM especially in triple refractory populations has been challenging, the discovery of novel therapeutic agent Belantamab Mafodotin, an anti BCMA antibody-drug conjugate targeting B-cell maturation antigen, have opened new avenues for treating these patients [2].
Initially approved by the FDA in august 2020 for RRMM patients who had received at least 4 prior therapies, belantamab mafodotin demonstrates encouraging effectiveness with response rates around 31-34% as shown the phase 2 DREAMM-2 trial [3]. However, the use of belantamab mafodotin has been convoluted by ocular toxicities such as keratopathy, corneal adverse events and transfusion reactions [4].
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Sayyaparaju MV (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Sayyaparaju MV, Sheikh J, Kuthadi K, Mandallika S, Kanka A. Targeting BCMA with belantamab mafodotin: A review of mechanisms, clinical efficacy and future directions. Open J Clin Med Case Rep. 2024; 2291.
Introduction
MM accounts for 1.8% of new cancer diagnoses and 2.1% of all cancer related deaths in United States [5], with the median age of diagnosis being around 65-70 years [6].
MM is characterized by abnormal plasma cell proliferation in the bone marrow, producing an excess of Monoclonal protein (M-protein) detected in blood and urine [7]. This M-protein causes specific organ damage resulting in the signs and symptoms such as hypercalcemia, renal insufficiency, anemia, amyloidosis and osteolytic bone lesions [8]. The diagnosis of MM requires the presence of ≥10% plasma cells on bone marrow exam or biopsy proven plasmacytoma alongside at least one Myeloma defining event [9].
Treatment induction usually begins as combination therapy with a proteosome inhibitor, an immunomodulatory agent, a steroid and/or a monoclonal antibody [10,11]. However, less than 10% of patients achieve sustained response after 5-10 years, and overall survival in patients taking at least 3 lines of therapy is still poor [12].
MM progresses in a remitting relapsing manner and, due to its innate stem cell like nature and interactions with the microenvironment, eventually achieves drug resistance [13]. Prognosis is exceptionally poor in CD38 antibody resistant cell lines with median overall survival being less than 1 year [14].
This presents an unmet therapeutic need for novel agents to treat such patients with drug resistant RRMM. As such the B-cell maturation antigen has emerged as an attractive target for the treatment of MM in recent years.
Belantamab mafodotin acts as an antibody-drug conjugate, which specifically targets B-cell maturation antigen, a protein present on the cell surface, which is expressed selectively on plasma cells and all multiple myeloma cells [15].
This specific targeting permits for the direct delivery of Monomethyl Auristatin F (MMAF), a cytotoxic agent, to tumor cells thus contributing to a distinctly different mechanism of action compared to traditional chemotherapy or immunotherapy [16].
Its high efficacy in killing tumour cells and reduced off-target effects provide a dual advantage, considered critical in heavily pretreated populations who have exhausted other treatment options. However, the unique toxicity profile of Belantamab, particularly its penchant for ocular toxicities, has made its use somewhat challenging [17].
Our study aims to explore the mechanism of action and efficacy of Belantamab mafodotin through studying various drug trials and compares it to existing agents used in the treatment of MM.
Mechanism of Action
The structure of belantamab mafodotin is comprised of 3 main parts. An anti-BCMA monoclonal antibody component, which binds selectively to BCMA on myeloma cells and leads to internalization of the complex, A linker molecule which is cleaved in the lysosomal compartment of the cell, and monomethyl auristatin F, the cytotoxic component of the drug, which exerts its effects by disruption of the microtubule network essential for the cell division [16].
BCMA plays a vital role in the growth of the myeloma cells through various signalling pathways, such as NF-kB, which drives cell survival and proliferation [18]. Belantamab binds to BCMA and inhibits this pathway leading to apoptosis. Furthermore, the cytotoxic component, monomethyl auristatin F, is a potent disruptor of immune cell division; leading to the cell cycle arrest at the G2/M phase followed by apoptosis by binding to tubulin and inhibiting its polymerization, a step crucial for viability and cell division [19].
This conjugate mechanism of belantamab mafodotin allows for the direct delivery of cytotoxic components to the myeloma cells, minimizing its exposure to non-target cells. This contrasts with CD 38 antibodies like daratumumab and isatuximab, whose primary function is through immune mediated mechanisms and direct apoptosis without delivery of a cytotoxic component [20].
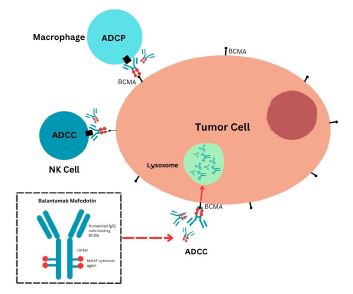
Figure 1:
Clinical Efficacy
DREAMM-1 was the first human open label study that assesed the safety and pharmocokinetics of Belantamab in patients with RRMM. The study, a phase II trial, testing the efficacy of 3.4 mg/kg of Belantamab on participants with results showing an Overall Risk Reduction (ORR) of 60% and Progression Free Survival (PFS) of 7.9 months. After a 14-month follow-up, the PFS had extended upto 12 months, and as such 54% of patients were deemed to have shown a Very Good Partial Response (VGPR) [21].
The success of DREAMM-1 study led to researchers expanding the trial as the DREAMM-2 study, an open-label, randomized trial studying the effects of 2 doses of belantamab: The original dose of 3.4 mg/kg vs a newer dose of 2.5 mg/kg, given intravenously once every 3 weeks [16,22]. The DREAMM-2 tested these doses on RRMM patients with ≥4 prior therapies; including an anti-CD38 mAb, a Protease Inhibitors and an Immunomodulatory agent. While both doses showed similar efficacies of 31% and 34% respectively, the incidence of adverse effects such as keratopathy, thrombocytopenia and anemia were significantly lower in the 2.5 mg/kg population, making it the FDA approved standard. Keratopathies were dealt with by dose reductions or dose delays.
| Trial Name | Phase | NCTNumber | Patient Demographics | Study Design | Primary Objectives | Outcome Measures | Key Findings | Current Status | References |
|---|---|---|---|---|---|---|---|---|---|
| DREAM M-1 | 1/2 | NCT02064 387 | Adultswith relapsed/refra ctory MM | Dose-escalation and expansion study | Evaluate safety, tolerability,and preliminary efficacy | ORR, safety profile, pharmacokin etics, dose- limiting toxicities | Identified optimaldosing and established preliminary efficacy; ORR of 60% in the dose-expansion cohort | Completed | [22] |
| DREAM M-2 | 2 | NCT03525 678 | RRMM with ≥4 prior therapies, including an anti-CD38 mAb, PI,and IMiD | Two-cohort, open-label | Assess efficacy and safety at two dose levels | ORR, duration ofresponse, time to response, PFS | ORR of 31% at 2.5 mg/kg and 34% at 3.4 mg/kg; significant keratopathy issues necessitated dose adjustments | Completed | [16] |
| DREAM M-3 | 3 | NCT04162 210 | RRMM, ≥2 prior lines including ananti-CD38 mAb | Randomized trial comparing belantamab mafodotin to pomalidomide + dexamethasone | Evaluate PFSwhen compared to standard treatment | PFS, ORR,safety profile,quality of life | Trial ongoing, aiming to establishsuperiority in efficacy and safety over current therapies | Ongoing | [23] |
| DREAM M-4 | 1/2 | NCT03848 845 | RRMM | Combination study with pembrolizumab | Assess safety andpreliminary efficacy ofthe combinati on therapy | ORR, safety profiles, biomarker analysis | Early resultsindicate manageable safety and potential for enhanced efJicacy with pembrolizu mab | Ongoing | [24] |
| DREAM M-5 | 2 | NCT04126 200 | RRMM | Platform trial testing various combinations with belantamab | Evaluate safety and efficacy acrossdifferent therapeutic combinations | ORR, PFS,safety profiles | Investigatingmultiple combinations to identify optimal therapeutic strategies; ongoing study | Ongoing | [25] |
| DREAM M-6 | 1/2 | NCT03544 281 | RRMM | Study combining belantamab mafodotin with bortezomiband dexamethasone | Explore the safety, tolerability, and efficacy of the combination | ORR, PFS, OS,safety and tolerability metrics | Early results show promise with manageableside effects; ongoingstudy | Ongoing | [26] |
| DREAM M-7 | 3 | NCT04484 623 | RRMM, ≥2 priortherapies | Randomized trial comparing different combinations involving belantamb mafodotin | Determine the efficacy and safety of various combination regimens | PFS, ORR,OS,safety profiles | Evaluates the efficacyof differenttherapeutic combinations;ongoing trial | Ongoing | [27] |
| DREAM M-8 | 3 | NCT04484 623 | RRMM, ≥2 priortherapies | Randomized trial comparing different combinations involving belantamab Mafodotin | Determin e the efficacy and safety of various combination regimens | PFS, ORR,OS,safety profiles | Evaluates the efficacyof differenttherapeutic combinations;ongoing trial | Ongoing | [28] |
| DREAM M-9 | 1 | NCT04091 126 | Newlydiagnosed MM | Evaluating belantama b mafodotin with afrontline therapy regimen | Assesssafety, efFicacy, and depth ofresponse in frontline settings | ORR, PFS,MRDstatus, safety proFiles | Early phase study to assess integration into frontline therapy; ongoing | Ongoin g | [29] |
Comparison with other Drugs
Immunotherapy
CD38 Antagonists: Daratumumab (DARA) is an Immunoglobulin G1 kappa (IgG1k) human monoclonal antibody that works by binding the cell surface antigen CD38 [30]. DARA induces tumor cell death through Complement Dependent Cytotoxicity (CDC) and Antibody-Dependant Cell-Mediated Cytotoxicity (ADCC) and has been shown to induce Antibody Dependant Cellular Phagocytosis (ADCP) due to it having Fc-de- pendent anti-tumor function [31-33]. DARA has also shown FcR-mediated crosslinking with CD38 expres- sing cancer cells and inducing apoptosis [31-34].
Slamf7/CS1: Elotuzumab is a monoclonal antibody that binds to CS1 adhesion molecules belonging to the SLAM (Signalling Lymphocytic Activation Molecule) family of receptors expressed on the surface of MM cells [35]. Elotuzumab activity is mediated by Fcy receptor mediated activation of Natural Killer (NK) cells via CS1 binding causing ADCP [36]. Furthermore, it also enhances NK cell cytotoxicity independent of ADCC through CS1-CS1 interactions between NK and target cells.
Immunomodulators
Immunomodulators (IMiDs) have both direct tumor cytotoxicity while indirectly interfering with the tumor microenviorment. They downregulate NF-κB signaling and induce JNK mediated apoptosis through the capsase 8 pathway [37]. They also inhibit the production of IL-6 and vascular endothelial growth factor preventing growth and proliferation of myeloma cells while simultaneously activating T-cells to produce IL-2, altering NK cell function and promoting NK-dependent cytotoxicity [38,39].
Additionally, Thalidomide and its derivatives, Lenalidomide and Pomalidomide, bind to cereblon causing the downregulation of IRF4, a prominent survival factor in MM cells. Decreased IRF4 levels lead to the degradation of transcription factors Ikaros (Ikaros family zinc finger protein 1) and Aiolos (Ikaros family zinc finger protein 3) required for tumor cell proliferation [40].
While Thalidomide and its derivatives demonstrate similar biologic properties, Lenalidomide and Pomalidomide are more potent, achieving better responses at lower doses and have better safety profiles [37].
Proteasome inhibitors
Proteosome Inhibitors (PI) have been the backbone of MM therapy. Bortezomib in 2003, carfilzomib in 2012 and ixazomib in 2015 were approved by the FDA for the treatment of patients with MM [41].
Bortezomib, the most commonly used proteasome inhibitor, is a 26S proteasome inhibitor which induces accumulation of intracellular misfolded or unfolded proteins causing Endoplasmic Reticular (ER) stress with which triggers the proapoptotic Unfolded Protein Response (UPR), it additionally prevents degradation of IκB and activation of NF-κB which supresses the production of survival factors [42]. It also causes immunogenic cell dealth via expression of heat shock protein 90, increasing cancer cell recognition by dendritic cells [43]. Additionally, it causes the release of Calreticulin (CALR) chaperone protein due to action ER stress kinase eIF2α kinase-3, and its migration to the plasma membrane surface where it initiates phagocytosis of dying cells by dendritic cells [44]. It also initiates the activation of the STING pathway that enhances cancer antigen presentation and upregulating detection and elimination by T cells [44].
Carfilzomib is a peptide epoxyketone and a second-generation PI that irreversibly binds proteasome triggering UPR mediated apoptosis [45]. Uniquely, it inhibits the chymotrypsin-like activity of proteasome inducing p53-mediated apoptosis [46]. Importantly, it shows increased efficacy and safety profile compared with bortezomib. It also shows efficacy against bortezomib- resistant MM cell lines [47,48].
Ixazomib is citrate ester of boronic acid and the first second-generation PI with oral bioavailability. It acts through the same mechanism as bortezomib by reversibly binding to and inhibiting the 26S proteasome responsible for protein degradation [49]. It, like carfilzomib, shows favourable safety profile and action against bortezomib-resistant MM [50].
Alkylating agents
The role of alkylating agents such as Melphalam, cyclophosphamide has changed from front-line agents in recent years, replaced by more active combinations of PI, IMiD and monoclonal CD38 antibodies.
These agents function by interfering with base repair by excision and opening of the guanine ring through alkylation of guanine. They also interfere with DNA transcription and replication through intra and inter strand cross linking [51].
Melphalan flufenamide (Melflufen) is recently creating traction for its role in the treatment of relapsed/refractory MM. Melflufen is a peptide drug conjugate that, on entry into tumor cells, is hydrolyzed by peptidases to release alkylating agents [52]. Melflufen has demonstrated action against both bortezomib- resistant as well as Melphalam resistent MM strains, and is 50 times more potent than melphalam due to its high lipophilicity and intracellular peptide binding potential [51].
Glucocorticoids
Steroid medication in combination with other agents help augment the treatment of MM with Dexamethasone being the most commonly used agent [53]. Dexamethasone has shown to induce apoptosis in MM cells by inhibiting NF-κB and upregulating IκB activity [54]. However their significant adverse effect profile impact patient quality of life and therefore limit their use [55].
Summary
Multiple myeloma is characterised by its relapsing remitting nature, despite various breakthroughs in treatment modalities and aggressive treatment, the long-term prognosis remains poor, especially in patients resistant to multiple lines of therapy [54,53].
As such CD38 monoclonal antibodies such as daratumumab, have become an essential component in the treatment of MM [56,57].
However, Cell lines resistant to CD38 mAb have become more prevalent [58]. The challenge of treating CD-38 resistant MM necessitates the development of novel treatment modalities that overcome or bypass this roadblock.
The discovery of belantamab mafodotin, an antibody-drug conjugate, introduces a new modality of treatment with combative potential against resistant disease, by targeting BCMA found on the surface of tumor cells [59].
The DREAMM clinical trials have been a game changer in the evaluation of clinical efficacy and safety of belantamab mafodotin in various patient populations. The DREAMM 1 phase I / II trial demonstrated an Overall Response Rate (ORR) of 60% and a Progression Free Survival (PFS) OF 7.9 months, which extended to around 12 months with a longer follow up [60].
The DREAMM 2 phase II trail, established the recommended dosage of belantamab mafodotin at 2.5 mg/kg with a reported ORR of 31% and better tolerability in terms of adverse effects, particularly ocular toxicities such as keratopathy and anemia [61].
Early results from the DREAMM 4 and DREAMM 6 trials studying the effects of adding Belatumab as part of combination therapy with pembrolizumab and bortezomib/dexamethasone, respectively, report enhanced efficacy when compared with control [24,26].
While Belantamab mafodotin opens new doors for the treatment of RRMM, it’s use remains controversial due to a significant side effect profile, mainly comprising of ocular toxicities such as keratopathy, anemia, thrombocytopenia and transfusion reactions, that are managed by either dose reductions or delays in treatment in conjunction to close monitoring of patients. The management of these side effects is key to maximizing the therapeutic potential of belantamab, alongside minimizing harm to the patient [62,2]. Despite promising results of the DREAMM trials, further studies are necessary to enhance and optimise the use of belantamab in clinical practice. Further research should focus on various strategies to negate prominent side effects, explore various combination therapies that enhance efficacy, and determine long term survival outcomes in patients treated with belantamab. Additionally, creating a deeper understanding of the mechanism of action of the drug may be critical in preventing drug resistance and developing future therapies for RRMM.
Conclusion
Belantamab an antibody drug conjugate, through targeting BCMA on the surface of tumour cells, displays significant benefits in progression free survival and overall response rate in patients with relapsed or refractory MM. This was especially important for patients with CD38 resistant cell lines and can be an avenue worthy of exploration for patients with multi drug resistant MM. However, the ocular side effects from its use create challenges in treatment that require careful management to optimise patient outcome.
References
- Rajkumar SV, Greipp PR. Prognostic Factors in Multiple Myeloma. Hematol Oncol Clin North Am. 1999; 13(6): 1295-1314. doi: 10.1016/S0889-8588(05)70128-3
- Offidani M, CorvaXa L, Morè S, Olivieri A. Belantamab mafodotin for the treatment of multiple myeloma: An overview of the clinical efficacy and safety. Drug Des Devel Ther. 2021; 15: 2401-2415. doi: 10.2147/DDDT.S267404
- Nooka AK, Cohen AD, Lee HC, et al. Single-agent belantamab mafodotin in patients with relapsed/refractory multiple myeloma: Final analysis of the DREAMM-2 trial. Cancer. 2023; 129(23): 3746-3760. doi: 10.1002/CNCR.34987
- Lassiter G, Bergeron C, Guedry R, et al. Belantamab Mafodotin to Treat Multiple Myeloma: A Comprehensive Review of Disease, Drug Efficacy and Side Effects. Current Oncology. 2021; 28: 640-660. doi: 10.3390/CURRONCOL28010063
- Myeloma-Cancer Stat Facts. 2024. hXps: //seer.cancer.gov/stafacts/html/mulmy.html
- Kazandjian D. Multiple myeloma epidemiology and survival: A unique malignancy. Semin Oncol. 2016; 43(6): 676-681. doi: 10.1053/J.SEMINONCOL.2016.11.004
- Hideshima T, Mitsiades C, Tonon G, Richardson PG, Anderson KC. Understanding multiple myeloma pathogenesis in the bone marrow to identify new therapeutic targets. Nature Reviews Cancer. 2007; 7(8): 585-598. doi: 10.1038/nrc2189
- Gerecke C, Fuhrmann S, Strifler S, Schmidt-Hieber M, Einsele H, Knop S. The Diagnosis and Treatment of Multiple Myeloma. Dtsch Arztebl Int. 2016; 113(27-28): 470. doi: 10.3238/ARZTEBL.2016.0470
- Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014; 15(12): e538-e548. doi: 10.1016/S1470-2045(14)70442-5
- Cowan AJ, Green DJ, Kwok M, et al. Diagnosis and Management of Multiple Myeloma: A Review. JAMA. 2022; 327(5): 464-477. doi: 10.1001/jama.2022.0003
- Rajkumar SV. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am J Hematol. 2022; 97(8): 1086-1107. doi: 10.1002/AJH.26590
- Usmani S, Ahmadi T, Ng Y, et al. Analysis of Real-World Data on Overall Survival in Multiple Myeloma Patients With ≥3 Prior Lines of Therapy Including a Proteasome Inhibitor (PI) and an Immunomodulatory Drug (IMiD), or Double Refractory to a PI and an IMiD. Oncologist. 2016; 21(11): 1355-1361. doi: 10.1634/THEONCOLOGIST.2016-0104
- Kellner J, Liu B, Kang Y, Li Z. Fact or fiction--identifying the elusive multiple myeloma stem cell. J Hematol Oncol. 2013; 6(1). doi: 10.1186/1756-8722-6-91
- Gandhi UH, Cornell RF, Lakshman A, et al. Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia. 2019; 33(9): 2266-2275. doi: 10.1038/S41375-019-0435-7
- Offidani M, CorvaXa L, Morè S, Olivieri A. Belantamab Mafodotin for the Treatment of Multiple Myeloma: An Overview of the Clinical Efficacy and Safety. Drug Des Devel Ther. 2021; 15: 2401-2415. doi: 10.2147/DDDT.S267404
- Lonial S, Lee HC, Badros A, et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): a two-arm, randomised, open-label, phase 2 study. Lancet Oncol. 2020; 21(2): 207-221. doi: 10.1016/S1470-2045(19)30788-0
- Offidani M, CorvaXa L, Morè S, Olivieri A. Belantamab mafodotin for the treatment of multiple myeloma: An overview of the clinical efficacy and safety. Drug Des Devel Ther. 2021; 15: 2401-2415. doi: 10.2147/DDDT.S267404
- Tai YT, Anderson KC. Targeting B-Cell Maturation Antigen in Multiple Myeloma. Immunotherapy. 2015; 7(11): 1187-1199. doi: 10.2217/IMT.15.77
- Yang L, Li X, Zhao L, Hu W, Qian Y. Design, synthesis and bioactivity evaluation of novel monomethyl auristatin F analogues. Mol Divers. Published online May 18, 2024: 1-16. doi: 10.1007/S11030-024-10873-1/METRICS
- Ferreri CJ, Lee HC. Antibody Drug Conjugates in Multiple Myeloma. Cancer Journal (United States). 2022; 28(6): 488-495. doi: 10.1097/PPO.0000000000000628
- Trudel S, Lendvai N, Popat R, et al. Antibody-drug conjugate, GSK2857916, in relapsed/refractory multiple myeloma: An update on safety and efficacy from dose expansion phase I study. Blood Cancer J. 2019; 9(4). doi: 10.1038/S41408-019-0196-6
- Eliason L, Opalinska J, Martin ML, Correll J, Gutierrez B, Popat R. DREAMM-1 Patient perspectives from the first-in-human study of single- agent belantamab mafodotin for relapsed and refractory multiple myeloma (RRMM). hXps: //doi.org/101200/JCO20203815_suppl.e20531. 2020; 38(15_suppl): e20531-e20531. doi: 10.1200/JCO.2020.38.15_SUPPL.E20531
- Dimopoulos MA, Hungria VTM, Radinoff A, et al. Efficacy and safety of single-agent belantamab mafodotin versus pomalidomide plus low-dose dexamethasone in patients with relapsed or refractory multiple myeloma (DREAMM-3): A phase 3, open-label, randomised study. Lancet Haematol. 2023; 10(10): e801-e812. doi: 10.1016/S2352-3026(23)00243-0
- Study Details | Study Evaluating Safety, Tolerability and Clinical Activity of GSK2857916 in Combination With Pembrolizumab in Subjects With Relapsed/Refractory Multiple Myeloma (RRMM) | ClinicalTrials.gov. Accessed August 14, 2024. hXps: //clinicaltrials.gov/study/NCT03848845
- Nooka AK, Weisel K, Van De Donk NWCJ, et al. Belantamab mafodotin in combination with novel agents in relapsed/refractory multiple myeloma: DREAMM-5 study design. Future Oncol. 2021; 17(16): 1987-2003. doi: 10.2217/FON-2020-1269
- Quach H, Gironella M, Lee C, et al. P941: Safety And Clinical Activity Of Belantamab Mafodotin With Lenalidomide Plus Dexamethasone In Patients With Relapsed/Refractory Multiple Myeloma (RRMM): DREAMM-6 ARM-A INTERIM ANALYSIS. Hemasphere. 2022; 6: 831-832. doi: 10.1097/01.HS9.0000846632.03623.AF
- Hungria V, Robak P, Hus M, et al. Belantamab Mafodotin, Bortezomib, and Dexamethasone for Multiple Myeloma. N Engl J Med. 2024; 391(5). doi: 10.1056/NEJMOA2405090
- Trudel S, Beksac M, Pour L, et al. Results from the randomized phase 3 DREAMM-8 study of belantamab mafodotin plus pomalidomide and dexamethasone (BPd) vs pomalidomide plus bortezomib and dexamethasone (PVd) in relapsed/refractory multiple myeloma (RRMM). hXps: //doi.org/101200/JCO20244217_supplLBA105. 2024; 42(17_suppl): LBA105-LBA105. doi: 10.1200/JCO.2024.42.17_SUPPL.LBA105
- Usmani S, Alonso A, Quach H, et al. P14: DREAMM-9: Phase I Study Of Belantamab Mafodotin Plus Standard Of Care In Patients With Transplant-Ineligible Newly Diagnosed Multiple Myeloma. Hemasphere. 2022; 6(Suppl): 19-19. doi: 10.1097/01.HS9.0000829628.48136.02
- de Weers M, Tai YT, van der Veer MS, et al. Daratumumab, a novel therapeutic human CD38 monoclonal antibody, induces killing of multiple myeloma and other hematological tumors. J Immunol. 2011; 186(3): 1840-1848. doi: 10.4049/JIMMUNOL.1003032
- Overdijk MB, Verploegen S, Bögels M, et al. Antibody-mediated phagocytosis contributes to the anti-tumor activity of the therapeutic antibody daratumumab in lymphoma and multiple myeloma. MAbs. 2015; 7(2): 311-320. doi: 10.1080/19420862.2015.1007813
- Grugan KD, McCabe FL, Kinder M, et al. Tumor-associated macrophages promote invasion while retaining Fc-dependent anti-tumor function. J Immunol. 2012; 189(11): 5457-5466. doi: 10.4049/JIMMUNOL.1201889
- Castella M, de Larrea CF, Marvn-Antonio B. Immunotherapy: A Novel Era of Promising Treatments for Multiple Myeloma. Int J Mol Sci. 2018; 19(11). doi: 10.3390/IJMS19113613
- Jansen JHM, Boross P, Overdijk MB, van Bueren JJL, Parren PWHI, et al. Daratumumab, a Human CD38 Antibody Induces Apoptosis of Myeloma Tumor Cells Via Fc Receptor-Mediated Crosslinking. Blood. 2012; 120(21): 2974-2974. doi: 10.1182/BLOOD.V120.21.2974.2974
- VeilleXe A, Guo H. CS1, a SLAM family receptor involved in immune regulation, is a therapeutic target in multiple myeloma. Crit Rev Oncol Hematol. 2013; 88(1): 168-177. doi: 10.1016/J.CRITREVONC.2013.04.003
- Kurdi AT, Glavey S V, Bezman NA, et al. Antibody-Dependent Cellular Phagocytosis by Macrophages is a Novel Mechanism of Action of Elotuzumab. Mol Cancer Ther. 2018; 17(7): 1454-1463. doi: 10.1158/1535-7163.MCT-17-0998
- Minařík J, Ševčíková S. Immunomodulatory Agents for Multiple Myeloma. Cancers (Basel). 2022; 14(23): 14. doi: 10.3390/CANCERS14235759
- Anderson KC. Lenalidomide and thalidomide: mechanisms of action--similarities and differences. Semin Hematol. 2005; 42(4 Suppl 4). doi: 10.1053/J.SEMINHEMATOL.2005.10.001
- Vallet S, Palumbo A, Raje N, Boccadoro M, Anderson KC. Thalidomide and lenalidomide: Mechanism-based potential drug combinations. Leuk Lymphoma. 2008; 49(7): 1238-1245. doi: 10.1080/10428190802005191
- Ito T, Handa H. Molecular mechanisms of thalidomide and its derivatives. Proc Jpn Acad Ser B Phys Biol Sci. 2020; 96(6): 189-203. doi: 10.2183/PJAB.96.016
- Ito S. Proteasome Inhibitors for the Treatment of Multiple Myeloma. Cancers (Basel). 2020; 12(2). doi: 10.3390/CANCERS12020265
- Hideshima T, Richardson PG, Anderson KC. Mechanism of Action of Proteasome Inhibitors and Deacetylase Inhibitors and the Biological Basis of Synergy in Multiple Myeloma. Mol Cancer Ther. 2011; 10(11): 2034. doi: 10.1158/1535-7163.MCT-11-0433
- Spisek R, Charalambous A, Mazumder A, Vesole DH, Jagannath S, et al. Bortezomib enhances dendritic cell (DC)-mediated induction of immunity to human myeloma via exposure of cell surface heat shock protein 90 on dying tumor cells: therapeutic implications. Blood. 2007; 109(11): 4839-4845. doi: 10.1182/BLOOD-2006-10-054221
- Mujtaba T, Dou QP. Advances in the Understanding of Mechanisms and Therapeutic Use of Bortezomib. Discov Med. 2011; 12(67): 471. Accessed August 12, 2024. /pmc/articles/PMC4139918/
- Kuhn DJ, Chen Q, Voorhees PM, et al. Potent activity of carfilzomib, a novel, irreversible inhibitor of the ubiquitin-proteasome pathway, against preclinical models of multiple myeloma. Blood. 2007; 110(9): 3281-3290. doi: 10.1182/BLOOD-2007-01-065888
- Pautasso C, Bringhen S, Cerrato C, MagaroXo V, Palumbo A. The mechanism of action, pharmacokinetics, and clinical efficacy of carfilzomib for the treatment of multiple myeloma. Expert Opin Drug Metab Toxicol. 2013; 9(10): 1371-1379. doi: 10.1517/17425255.2013.817556
- Carfilzomib (Kyprolis): A Novel Proteasome Inhibitor for Relapsed And/or Refractory Multiple Myeloma - PMC. 2024. hXps: //www.ncbi.nlm.nih.gov/pmc/articles/PMC4849338/
- Jayaweera SPE, Wanigasinghe Kanakanamge SP, Rajalingam D, Silva GN. Carfilzomib: A Promising Proteasome Inhibitor for the Treatment of Relapsed and Refractory Multiple Myeloma. Front Oncol. 2021; 11. doi: 10.3389/FONC.2021.740796
- Muz B, Ghazarian RN, Ou M, Luderer MJ, Kusdono HD, Azab AK. Spotlight on ixazomib: potential in the treatment of multiple myeloma. Drug Des Devel Ther. 2016; 10: 217. doi: 10.2147/DDDT.S93602
- Xie J, Wan N, Liang Z, Zhang T, Jiang J. Ixazomib - the first oral proteasome inhibitor. Leuk Lymphoma. 2019; 60(3): 610-618. doi: 10.1080/10428194.2018.1523398
- Schjesvold F, Oriol A. Current and Novel Alkylators in Multiple Myeloma. Cancers (Basel). 2021; 13(10): 13. doi: 10.3390/CANCERS13102465
- Mateos MV, Bladé J, Bringhen S, et al. Melflufen: A Peptide-Drug Conjugate for the Treatment of Multiple Myeloma. J Clin Med. 2020; 9(10): 1-16. doi: 10.3390/JCM9103120
- Burwick N, Sharma S. Glucocorticoids in multiple myeloma: Past, present, and future. Ann Hematol. 2019; 98(1): 19-28. doi: 10.1007/S00277-018-3465-8
- Rosenberg AS. From mechanism to resistance - changes in the use of dexamethasone in the treatment of multiple myeloma. Leuk Lymphoma. 2023; 64(2): 283-291. doi: 10.1080/10428194.2022.2136950
- McKenzie F, Gazzé G, HewiX J, et al. Canadian perspectives in multiple myeloma on the use of steroids in clinical practice based on patient and healthcare provider interviews. Front Oncol. 2022; 12: 1061417. doi: 10.3389/FONC.2022.1061417
- Nishihori T, Alsina M. Relapsed and Refractory Multiple Myeloma. Emerging Cancer Therapeutics. 2023; 1(2): 383-402. doi: 10.5003/2151- 4194.1.2.383
- Nooka AK, Kaufman JL, Hofmeister CC, et al. Daratumumab in multiple myeloma. Cancer. 2019; 125(14): 2364-2382. doi: 10.1002/CNCR.32065
- Van De Donk NWCJ, Usmani SZ. CD38 antibodies in multiple myeloma: Mechanisms of action and modes of resistance. Front Immunol. 2018; 9(SEP): 406716. doi: 10.3389/FIMMU.2018.02134/BIBTEX
- Behren Ketchum, PharmD E, Clarke, PharmD, BCOP A, B. Clemmons, PharmD, BCOP A. Belantamab Mafodotin-blmf: A Novel Antibody- Drug Conjugate for Treatment of Patients With Relapsed/Refractory Multiple Myeloma. J Adv Pract Oncol. 2022; 13(1): 77. doi: 10.6004/JADPRO.2022.13.1.7
- Eliason L, Opalinska J, Martin ML, Correll J, Popat R, et al. DREAMM-1 Patient perspectives from the first-in-human study of single- agent belantamab mafodotin for relapsed and refractory multiple myeloma (RRMM). hXps: //doi.org/101200/JCO20203815_suppl.e20531. 2020; 38(15_suppl): e20531-e20531. doi: 10.1200/JCO.2020.38.15_SUPPL.E20531
- Lonial S, Lee HC, Badros A, et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): a two-arm, randomised, open-label, phase 2 study. Lancet Oncol. 2020; 21(2): 207-221. doi: 10.1016/S1470-2045(19)30788-0
- Abeykoon JP, Vaxman J, Patel S V, et al. Impact of belantamab mafodotin-induced ocular toxicity on outcomes of patients with advanced multiple myeloma. Br J Haematol. 2022; 199(1): 95-99. doi: 10.1111/BJH.18298
