
Open Access, Volume 10
Perioperative use of pulmonary artery catheter in a patient with severe chronic thromboembolic pulmonary hypertension undergoing major gynaecological surgery: A case report
Laura Kekec1,2*; Radisavljević Vitas Sanja1; Bervar Mojca2,3; Taleska Štupica Gordana1,2
1Clinical Department of Anaesthesiology and Perioperative Intensive Therapy, University Medical Centre Ljubljana, Ljubljana, Slovenia.
2Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia.
3Department of Cardiology, University Medical Centre Ljubljana, Ljubljana, Slovenia.
Laura Kekec
Clinical Department of Anaesthesiology and Perioperative Intensive Therapy, University Medical Centre Ljubljana, Ljubljana, Slovenia.
Email: laura.kekec@gmail.com
Received : September 10, 2024,
Accepted : October 02, 2024
Published : October 15, 2024,
Archived : www.jclinmedcasereports.com
Abstract
Pulmonary Hypertension (PH) is one of the major risk factors for increased perioperative morbidity and mortality. It is crucial to prepare such patients preoperatively and to try to avoid substantial hemodynamic changes with optimal anaesthetic management.
A 52-year-old female patient was diagnosed with severe chronic thromboembolic pulmonary hypertension after presenting to the hospital with a cerebrovascular insult. Because of a big gynaecological tumor, lower median laparotomy with total hysterectomy and bilateral salpingo-oophorectomy was indicated. Perioperatively, we monitored pulmonary artery pressures with a Swan-Ganz Pulmonary Artery Catheter (PAC). Under glyceryl trinitrate infusion therapy, pulmonary pressures remained relatively stable.
The use of PAC usually depends on the severity of PH and right ventricular dysfunction, the level of surgical risk, and expertise. Our patient had severe PH with moderately weakened right ventricular function and underwent a moderate-risk non-cardiac surgical procedure. We decided on PAC over other monitoring techniques for continuous measurement of pulmonary artery pressures and right ventricular function parameters to manage this high-risk patient as beneficial as possible.
Keywords: Pulmonary hypertension; Chronic thromboembolic pulmonary hypertension; Pulmonary artery catheter; Non-cardiac surgery; Anaesthesia.
Abbreviations: ASA: American Society of Anaesthesiologists; CO: Cardiac Output; CVC: Central Venous Catheter; CVP: Central Venous Pressure; mPAP: Mean Pulmonary Artery Pressure; NYHA: New York Heart Association; PAC: Pulmonary Artery Catheter; PAP: Pulmonary Artery Pressure; PH: Pulmonary Hypertension; RV: Right Ventricle; TAPSE: Tricuspid Annular Plane Systolic Excursion; TDI: Tissue Doppler Imaging.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kekec L (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Kekec L, Sanja RV, Mojca B, Gordana TS. Perioperative use of pulmonary artery catheter in a patient with severe chronic thromboembolic pulmonary hypertension undergoing major gynaecological surgery: A Case Report. Open J Clin Med Case Rep. 2024; 2290.
Introduction
Pulmonary Hypertension (PH) is one of the major risk factors for increased perioperative morbidity and mortality [1]. Proper attention must be given to patients with PH undergoing surgical procedures as several perioperative situations can cause fluctuations in mean Pulmonary Artery Pressure (mPAP), filling pressures, and Cardiac Output (CO) [2]. It is crucial to prepare such patients preoperatively and to try to avoid substantial hemodynamic changes with optimal anaesthetic management.
Case Report
A 52-year old female patient was diagnosed with severe chronic thromboembolic pulmonary hypertension after presenting to the hospital with a cerebrovascular insult. Transthoracic echocardiography showed mildly impaired left ventricular function, a mildly enlarged right ventricle (Figures 1 and 2) with moderately impaired function (Figures 3 and 4), and severe pulmonary hypertension (Figures 5 and 6): systolic pulmonary artery pressure of 68 mmHg, mPAP of 41 mmHg, pulmonary vascular resistance 5.0WU. Transoesophageal echocardiography was done, which showed the absence of patent foramen ovale, the bubble study was negative (Figures 7 and 8). The electrocardiogram was normal. Lower extremity ultrasound showed fresh and old popliteal deep vein thrombosis bilaterally. She was started on a therapeutic dose of dalteparin. Laboratory tests were normal, except for S-NT-pro BNP of 957 ng/L and fibrinogen of 7.78 g/L. Screening for rheumatologic disease was done, with Sjögren syndrome and antiphospholipid syndrome suspected. Pulmonary function tests were normal.
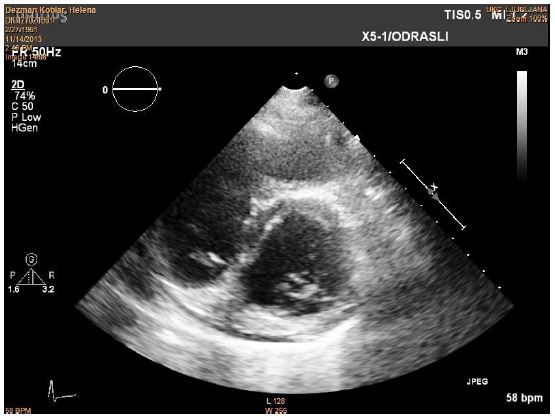
Figure 1: Enlarged right ventricle and D-sign, seen on parasternal short axis.
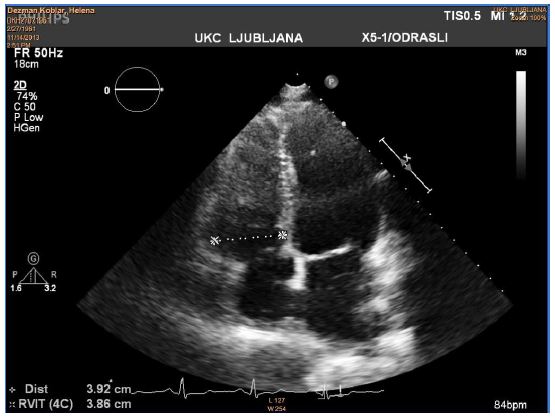
Figure 2: Enlarged right ventricle, seen on apical four-chamber view.
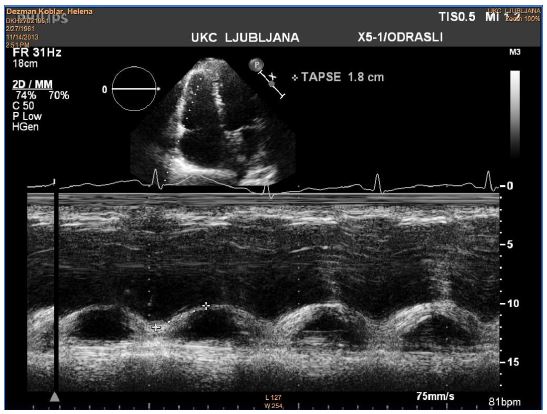
Figure 3: Measurement of tricuspid annular plane systolic excursion (TAPSE). TAPSE calculation in M-mode, using the four-chamber view.
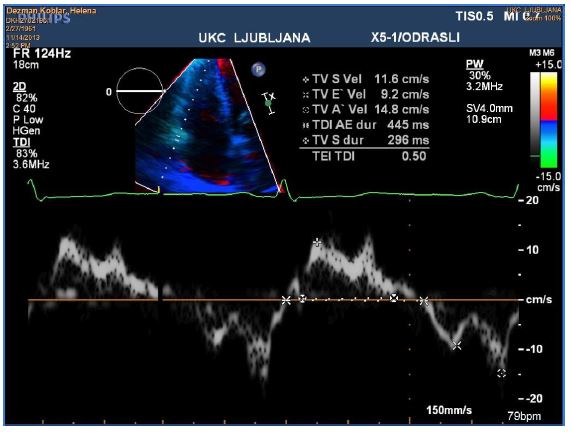
Figure 4: Tissue Doppler Imaging (TDI) velocities of tricuspid valve, using four-chamber view.
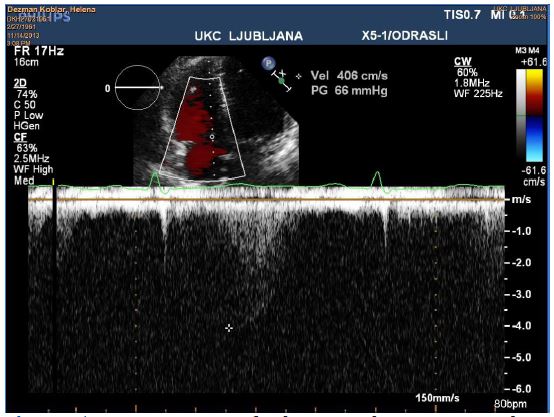
Figure 5: Measurement of velocity and pressure gradient across the tricuspid valve, using four-chamber view.
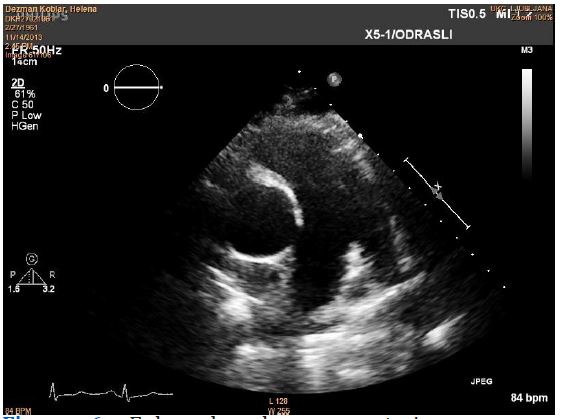
Figure 6: Enlarged pulmonary arteries, seen on parasternal short axis.
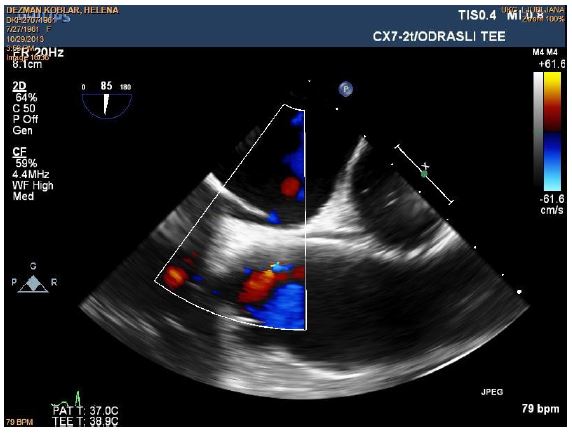
Figure 7: No signs of patent foramen ovale on transoesophageal echocardiography with colour doppler.
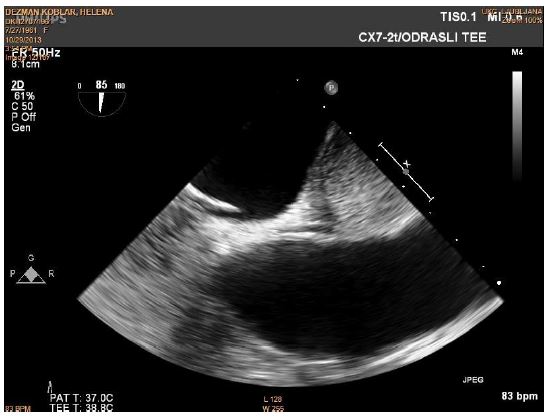
Figure 8: Transoesophageal echocardiography of interatrial septum during bubble study: No signs of passing bubbles through the interatrial septum.
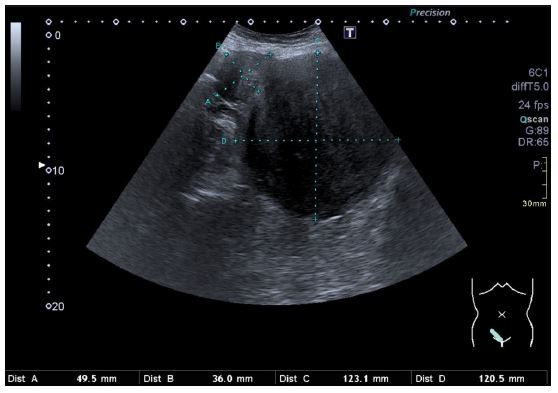
Figure 9: An abdominal ultrasound of the big tumorous mass in the uterus and the smaller mass next to it.
During the hospital stay, a mass in the abdomen could be palpated. An abdominal ultrasound revealed a big tumorous mass in the uterus measuring 12 x 12 cm and another, a bit smaller mass, measuring 5 x 3.5 cm (Figure 9). Lower median laparotomy with total hysterectomy and bilateral salpingo-oophorectomy was indicated. The surgery was performed 5 months after the cerebrovascular insult, meanwhile the patient was waiting at home in a stable condition.
Before the surgery, the patient weighed 62 kg, was 170 cm tall, and had an American Society of Anaesthesiologists (ASA) classification IV, New York Heart Association (NYHA) class II. There were no deviations in the clinical exam. The patient was cardiopulmonary compensated, she was eupnoeic, had no oedema, no abnormal lung sounds, and no hepatomegaly. One week before the surgery a vena cava filter was inserted.
Before the induction of general anaesthesia, an intravenous line and an arterial line were inserted. Monitoring with electrocardiogram, oxygen saturation, and invasive blood pressure were used. The first measured blood pressure was 140/82 mmHg, pulse was 65 beats per minute and oxygen saturation was 100%. For induction, 0.2 mg of fentanyl, 14 mg of etomidate and 40 mg of rocuronium were used. An infusion of glyceryl trinitrate 2 mg per hour was started to maintain the systolic blood pressure under 130 mmHg. Anaesthesia was maintained with sevoflurane and fentanyl. After the induction, a Central Venous Catheter (CVC) and a Swan-Ganz Pulmonary Artery Catheter (PAC) were inserted. During the procedure, Central Venous Pressure (CVP) remained in the range of 6 to 9 mmHg and mPAP in the range of 28 to 35 mmHg. The patient remained stable throughout the procedure, normocardic, with blood pressures in the normal range. The blood loss was minimal. Duration of anaesthesia was 1 hour and 40 minutes. The emergence from anaesthesia and extubation were done in the operating theatre.
After the procedure, the patient was observed in the intermediate care unit. She was receiving an infusion of glyceryl trinitrate 0.5-1 mg per hour. Until the next morning, the pulmonary artery pressures were monitored, with mPAP staying between 27 to 35 mmHg. On the morning of the first postoperative day, the Swan-Ganz catheter was removed, and the infusion of glyceryl trinitrate was stopped. Postoperative pain control was good with intravenous piritramide by patient-controlled analgesia and intravenous boluses of non-opioid analgesics (metamizole, paracetamol). On the sixth postoperative day, she was transferred to the ward, and on the eighth postoperative day, she was discharged home, receiving regular pre-operative therapy (dalteparin, rosuvastatin) and analgesics.
Discussion
The infusion of systemic vasodilator glyceryl trinitrate was used during and after the procedure, as it can help reduce pulmonary vascular resistance and increase CO by relaxing the blood vessels and increasing the supply of blood and oxygen to the heart while reducing its work load. The use of vasodilators in patients with PH undergoing surgery is recommended by many authors [2-4]. Although vasodilators like glyceryl trinitrate should be used with greatest care and only for patients with a sufficiently high mean arterial pressure value, as well as adequate preload, since they can cause a considerable decrease in blood pressure. We titrated the infusion to keep the mean arterial pressure in the range of 70-80 mmHg for sufficient coronary flow. Perioperatively, there was no need for vasopressor therapy at any stage.
For the continuous monitoring of blood pressure, the arterial line was placed before induction. In our patient, CVC was inserted after induction and CVP was maintained in the normal range. In PH patients, it is not possible to accurately assess left ventricular preload with CVP, but it can be used to assess right atrial and Right Ventricular (RV) filling pressures [2,5]. We decided that CVC was necessary also because of possible administration of vasoactive substances and electrolyte management. PAC can monitor changes in PAP, myocardial oxygen consumption, is useful for assessment of RV function and CO during the procedure, and interventions such as titration of vasoactive or inotropic therapy. On the other hand, it is invasive, it’s placement can induce arrhythmias, and rarely pulmonary artery branch rupture. The use of PAC usually depends on the severity of RV dysfunction and PH, the level of surgical risk, and expertise [2,6]. While some authors do not find it necessary for perioperative use [5,7], others believe it is crucial for intraoperative monitoring [8,9].
Our patient had severe PH and the procedure was moderate-risk. We decided on the insertion of Swan-Ganz PAC for continuous monitoring of pulmonary artery pressures, as well as right ventricular ejection fraction and right ventricular end diastolic volume due to moderately weakened right ventricular function in our patient. In this scenario, we also found important the monitoring of mixed venous oxygen saturation as a sensitive indicator of the patient’s status that generally precedes other indications of cardiopulmonary instability, and last but not least CO and systemic vascular resistance. An experienced cardiovascular anaesthesiologist was managing the patient, so the chance of unwanted events was low.
Transoesophageal echocardiography is widely recognized as the most important non-invasive alternative for monitoring of PAP, right and left ventricular function, as well as fluid management guidance, some even consider it to be advantageous to the monitoring by PAC [10]. Its use requires the operator’s skill and experience. We decided on PAC over transoesophageal echocardiography for easier postoperative management of this high-risk patient in the intermediate care unit at the Department of Obstetrics and Gynaecology, since no cardiac anaesthesiologists or cardiologists are regularly present there, and performing repeated echocardiography would be difficult.
References
- Smilowitz NR, Armanious A, Bangalore S, Ramakrishna H, Berger JS. Cardiovascular Outcomes of Patients With Pulmonary Hypertension Undergoing Noncardiac Surgery. Am J Cardiol. 2019; 123: 1532-7. https://doi.org/10.1016/J.AMJCARD.2019.02.006.
- Kaw RK. Unrecognized Pulmonary Hypertension in Non-Cardiac Surgical Patients: At-Risk Populations, Preoperative Evaluation, Intraoperative Management and Postoperative Complications. J Cardiovasc Dev Dis. 2023; 10: 403. https://doi.org/10.3390/JCDD10090403.
- Blaise G, Langleben D, Hubert B. Pulmonary Arterial HypertensionPathophysiology and Anesthetic Approach. Anesthesiology. 2003; 99: 1415-32. https://doi.org/10.1097/00000542-200312000-00027.
- Teo YW, Greenhalgh DL. Update on anaesthetic approach to pulmonary hypertension. Eur J Anaesthesiol. 2010; 27: 317-23. https://doi.org/10.1097/EJA.0B013E328335474E.
- Fox C, Kalarickal PL, Yarborough MJ, Jin JY. Perioperative management including new pharmacological vistas for patients with pulmonary hypertension for noncardiac surgery. Curr Opin Anaesthesiol. 2008; 21: 467-72. https://doi.org/10.1097/ACO.0B013E3283007EB4.
- Rajagopal S, Ruetzler K, Ghadimi K, Horn EM, Kelava M, et al. Evaluation and Management of Pulmonary Hypertension in Noncardiac Surgery: A Scientific Statement From the American Heart Association. Circulation. 2023; 147: 1317-43. https://doi.org/10.1161/CIR.0000000000001136.
- Rinne T, Zwissler B. Intraoperative anesthetic management in patients with pulmonary hypertension. Intensiv Notfallbehandlung. 2004; 29: 4-13. https://doi.org/10.1155/2012/356982.
- Caddigan S, Granlund B. Anesthesia for Patients With Pulmonary Hypertension or Right Heart Failure. StatPearls. 2023.
- Krug S, Sablotzki A, Hammerschmidt S, Wirtz H, Seyfarth HJ. Inhaled iloprost for the control of pulmonary hypertension. Vasc Health Risk Manag. 2009; 5: 465-74. https://doi.org/10.2147/VHRM.S3223.
- Poelaert JI, Trouerbach J, De Buyzere M, Everaert J, Colardyn FA. Evaluation of transesophageal echocardiography as a diagnostic and therapeutic aid in a critical care setting. Chest. 1995; 107: 774-9. https://doi.org/10.1378/CHEST.107.3.774.
