
Open Access, Volume 10
Acute aortic regurgitation: Physical examination and echocardiography
Sayaka Takabayashi; Sakiko Honda; Michiyo Yamano; Tatsuya Kawasaki*
Department of Cardiology, Matsushita Memorial Hospital, Osaka, Japan.
Tatsuya Kawasaki
Department of Cardiology, Matsushita Memorial Hospital, Sotojima 5-55, Moriguchi, Osaka 570-8540, Japan.
Tel: +81-66992-1231;
Email: js-k@wf6.so-net.ne.jp
Received : September 04, 2024,
Accepted : September 24, 2024
Published : September 27, 2024,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Kawasaki T (2024)
Journal: Open Journal of Clinical and Medical Case Reports is an international, open access, peer reviewed Journal mainly focused exclusively on the medical and clinical case reports.
Citation: Takabayashi S, Honda S, Yamano M, Kawasaki T. Acute aortic regurgitation: Physical examination and echocardiography. Open J Clin Med Case Rep. 2024; 2289.
Description
A 79-year-old man presented with a 11-day history of dyspnea. His blood pressure was 149/61 mmHg, his pulse rate was 95 beats per minute, and his oxygen saturation level was 95% while breathing ambient air. The jugular venous pulsation was elevated to 20 cm H2O. Cardiac auscultation showed a systolic ejection murmur and an early diastolic murmur (i.e., a to-and-fro murmur) at the second sternal border (Figure 1A) and gallops at the apex (Figure 1B). Phonomechanocardiography showed a diastolic rumble, along with pulsus bisferiens, at the third sternal border (Figure 1C), all these findings consistent with acute severe aortic regurgitation (AR).
Transthoracic echocardiography revealed mitral regurgitation (MR) (Figure 1D) and AR (Figure 1E, arrow); MR was considered more predominant than AR. A diagnosis of decompensated heart failure with valvular heart disease was made.
Follow-up transthoracic echocardiography after treatment or one week after admission showed severe AR throughout diastole (Figure 1F), with improvement in MR severity. The cause of acute AR was considered to be cusp bending of the right coronary cusp, which was confirmed by transesophageal echocardiography.
Echocardiography plays a pivotal role in the diagnosis of valvular heart disease, but attention should be paid to the assessment of acute conditions, as shown in this case. Acute severe AR causes a sudden excessive volume load on an unprepared left ventricle and an extreme increase in the left ventricular diastolic pressure, leading to an early cessation of the AR flow and functional MR [1]. In the current patient, physical examination was more accurate than echocardiography in determining the etiology of heart failure. In conclusion, our case highlights the importance of physical examination performed in the clinical context, even in the era of advanced imaging technologies.
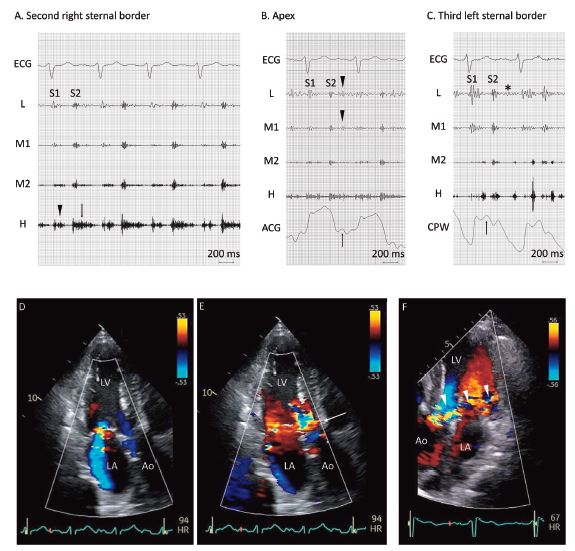
Figure 1: Phonocardiography on admission shows a high-pitched systolic ejection murmur (A, arrowhead) and an early- to mid-diastolic murmur (A, arrow) at the second right sternal border; note that the diastolic murmur starts immediately after the second sound (S2) and ends approximately 100 ms before the first sound (S1). At the apex, an additional low-pitched sound in early diastole (B, arrowheads) coincides with the rapid filling wave (B, arrow) of the apex cardiogram (ACG), findings consistent with the third sound. The carotid pulse wave (CPW) shows a biphasic pulse during systole, i.e., pulsus bisferiens (C, arrow), along with a diastolic rumble (C, asterisk). An apical three-chamber view of transthoracic echocardiography shows mitral regurgitation during systole (D). Note a flash of mosaic pattern in early diastole (E, arrow), in the absence of clear regurgitant flow. One week after admission, follow-up echocardiography shows severe aortic regurgitation throughout diastole (F, arrowheads). Ao denotes aorta; ECG: electrocardiography; H: high frequency; L: low frequency; LA: left atrium; LV: left ventricle; M1: lower-middle frequency; M2: higher-middle frequency.
Declarations
Acknowledgments: None declared.
Conflict of interest: None declared.
Conflict of interest covering all authors: None declared.
References
- Hamirani YS, Dietl CA, Voyles W, Peralta M, Begay D, et al. Acute aortic regurgitation. Circulation. 2012; 126(9): 1121-6.
